2498
Altered patterns of cerebral perfusion in systemic lupus erythematosus patients with cognitive dysfunction, pain and fatigue.1Department of Clinical Sciences/Radiology, Lund University, Lund, Sweden, 2Department of Clinical Sciences/Division of Logopedics, Phoniatrics and Audiology, Lund University, Lund, Sweden, 3Department of Clinical Sciences Lund/Rheumatology, Lund University, Skåne University Hospital, Lund, Sweden, 4Department of Clinical Sciences Lund/Neurology, Lund University, Skåne University Hospital, Lund, Sweden, 5Department of Medical Radiation Physics, Lund University, Lund, Sweden, 6Department of Medical Imaging and Physiology, Skåne University Hospital, Lund, Sweden, 7F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States, 8Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 9Lund University Bioimaging Center, Lund University, Lund, Sweden
Synopsis
Keywords: Neuroinflammation, DSC & DCE Perfusion, Systemic Lupus Erythematosus, Cognitive dysfunction, Fatigue, Pain, Fibromyalgia, Blood-brain barrier
Motivation: Cognitive dysfunction (CD), fatigue and pain are common and debilitating in systemic lupus erythematosus (SLE). Symptom-based neuroimaging could contribute to pathophysiological models and patient-centered care.
Goal(s): Investigating brain perfusion and blood-brain barrier permeability in SLE patients with CD, fatigue and pain.
Approach: 66 SLE patients underwent 3T dynamic susceptibility contrast (DSC) MRI. The leakage parameter K2 and normalized leakage corrected perfusion parameters were estimated in 14 brain regions, compared by symptomatology.
Results: Patients with CD or fibromyalgia displayed increased cerebral blood flow and/or cerebral blood volume in regions associated with pain processing. No differences were found for fatigue, K2 or mean transit time.
Impact: DSC-MRI detects cerebral hyperperfusion in systemic lupus erythematosus patients with cognitive dysfunction or the pain syndrome fibromyalgia, but not fatigue, suggesting different inflammatory or compensatory mechanisms. Investigating each of these debilitating symptoms separately might further characterize and guide patient-centered interventions.
Introduction
Patients with systemic lupus erythematosus (SLE) can present a wide range of neuropsychiatric complaints, with cognitive dysfunction (CD) being a common manifestation1. CD impacts the quality of life in SLE, alongside associated debilitating symptoms of pain and fatigue2. Recent magnetic resonance imaging (MRI) studies suggest that blood-brain barrier (BBB) dysfunction could contribute to the pathophysiology of CD1,3, highlighting the need for patient-centered neuroimaging, based on individual symptoms, to further investigate, predict and guide interventions. Additionally, studies using contrast agent-based perfusion MRI have revealed differences in cerebral perfusion and BBB leakage in patients with SLE compared to healthy controls4,5. However, fatigue and pain have not previously been investigated with perfusion MRI. Thus, the aim of this study was to investigate symptoms of CD, fatigue and pain in a cohort of SLE patients, applying the hypothesis that SLE patients with these symptoms present altered cerebral perfusion and BBB permeability.Methods
This study was conducted in an established outpatient SLE cohort, where the patients had previously undergone 3T structural and dynamic susceptibility contrast (DSC) MRI (MAGNETOM Skyra, Siemens, Germany)4. CD was clinically evaluated and considered to be present if the symptom could be attributed to SLE in accordance with the American College of Rheumatology (ACR) 1999 case definitions for neuropsychiatric SLE (NPSLE)6. Fatigue and pain were evaluated using the Fatigue Severity Scale (FSS)7 and the 1990 ACR classification of the chronic pain syndrome fibromyalgia (FM)8. Regions of interest were placed bilaterally in 14 predefined brain regions: medial temporal lobe (MTL), anterior and posterior insula, nucleus caudatus, putamen, thalamus, hypothalamus, corpus callosum, dorsolateral and ventromedial prefrontal cortex, frontal white matter (FWM), superior parietal lobule (SPL), anterior and posterior cingulate cortex. Tracer kinetic analysis, and the Boxerman-Schmainda-Weisskoff leakage correction method, enabled calculation of cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT) and the leakage parameter K29. CBF, CBV and MTT were normalized to normal appearing white matter in the middle cerebellar peduncles. The cohort was divided into symptom-specific groups and control groups based on: NPSLE-related CD (23 with CD and 43 without CD), FM (9 with FM and 57 without FM) and fatigue (44 with FSS > 35, indicating severe fatigue, and 22 with FSS ≤ 35). Analysis of covariance was performed with each perfusion and leakage measurement separately, adjusting for age, disease duration, smoking and corticosteroid treatment. The results were corrected for multiple comparisons.Results
A total of 66 SLE patients were investigated (median age 37.5 years, range 18-52 years, and median disease duration 10 years, range 0-26 years). Patients with CD displayed significantly increased CBF in the right nucleus caudatus, left FWM and bilateral hypothalami (Figure 1), and increased CBV in the left MTL, left FWM and bilateral hypothalami (Figure 2), compared to patients without CD. Patients with FM showed significantly increased CBF in the right posterior insula, right MTL, left FWM, and bilaterally in the putamina, thalami, and SPL, and increased CBV in the right posterior insula, right putamen, left FWM and left SPL, compared to patients without FM (Table 1). No significant differences were seen in MTT or K2, or in patients with higher FSS scores.Discussion
Brain perfusion and CD have previously been investigated in SLE using arterial spin labeling and single photon emission computed tomography (SPECT), with inconsistent results10,11. Our study found that SLE patients with CD show increased regional CBF and CBV, suggesting compensatory mechanisms or inflammation in this subgroup12. Furthermore, we found widespread perfusion alterations in SLE patients with FM. This is consistent with previous research suggesting brain activation and increased perfusion in regions such as the insula, thalamus and SPL in patients with chronic pain13,14. Our findings are in agreement with an earlier SPECT study that found no perfusion differences in SLE patients with fatigue15. In our study, we did not find any significant changes in K2. Some studies, using dynamic contrast enhanced MRI, have reported that SLE patients with CD show increased Ktrans, indicating a disrupted BBB3,5. However, Ktrans is a composite parameter, mixing perfusion and permeability, and this complicates a direct comparison between K2 and Ktrans.Conclusion
We found that SLE patients with CD or FM show higher CBF and CBV in regions associated with pain processing compared to SLE patients without these symptoms. This suggests altered cerebral perfusion in these subgroups, but not in SLE patients with fatigue. Further research using perfusion MRI is needed investigating individual symptoms in SLE, as well as deficits in specific cognitive domains.Acknowledgements
The study was supported by funding from Gustav V 80 Years Foundation, Skåne University Hospital Research Funding, Swedish Rheumatism Association, Alfred Österlunds Research Foundation, Greta and Johan Kocks Foundation, Swedish Research Foundation and the Swedish Brain Foundation. The funding sources had no involvement in the study design, collection and interpretation of data, nor in the writing or submission of the abstract.
The authors would like to thank Markus Nilsson at Lund University, Lund, Sweden, for providing the software Eval GUI used in the analysis.
References
1. Mizrachi M, Anderson E, Carroll KR, Tehrani N, Volpe BT, Diamond B. Cognitive dysfunction in SLE: An understudied clinical manifestation. J Autoimmun 2022;132:102911.2. Kim MY, Sen D, Drummond RR, et al. Cognitive dysfunction among people with systemic lupus erythematosus is associated with reduced participation in daily life. Lupus 2021;30:1100–1107.
3. Hanly JG, Legge A, Kamintsky L, et al. Role of autoantibodies and blood-brain barrier leakage in cognitive impairment in systemic lupus erythematosus. Lupus Sci Med 2022;9.
4. Salomonsson T, Rumetshofer T, Jönsen A, et al. Abnormal cerebral hemodynamics and blood-brain barrier permeability detected with perfusion MRI in systemic lupus erythematosus patients. Neuroimage Clin 2023;38:103390.
5. Kamintsky L, Beyea SD, Fisk JD, et al. Blood-brain barrier leakage in systemic lupus erythematosus is associated with gray matter loss and cognitive impairment. Ann Rheum Dis 2020;79:1580–1587.
6. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum 1999;42:599–608.
7. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 1989;46:1121–1123.
8. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum 1990;33:160–172.
9. Boxerman JL, Schmainda KM, Weisskoff RM. Relative cerebral blood volume maps corrected for contrast agent extravasation significantly correlate with glioma tumor grade, whereas uncorrected maps do not. AJNR Am J Neuroradiol 2006;27:859–867.
10. Sahebari M, Rezaieyazdi Z, Khodashahi M, Abbasi B, Ayatollahi F. Brain Single Photon Emission Computed Tomography Scan (SPECT) and functional MRI in Systemic Lupus Erythematosus Patients with Cognitive Dysfunction: A Systematic Review. Asia Ocean J Nucl Med Biol 2018;6:97–107.
11. Jia J, Xie J, Li H, et al. Cerebral blood flow abnormalities in neuropsychiatric systemic lupus erythematosus. Lupus 2019;28:1128–1133.
12. Wang PI, Cagnoli PC, McCune WJ, et al. Perfusion-weighted MR Imaging in Cerebral Lupus Erythematosus. Acad Radiol 2012;19:965–970.
13. Schmidt-Wilcke T. Neuroimaging of chronic pain. Best Pract Res Clin Rheumatol 2015;29:29–41.
14. Foerster BR, Petrou M, Harris RE, et al. Cerebral blood flow alterations in pain-processing regions of patients with fibromyalgia using perfusion MR imaging. AJNR Am J Neuroradiol 2011;32:1873–1878.
15. Omdal R, Sjöholm H, Koldingsnes W, et al. Fatigue in patients with lupus is not associated with disturbances in cerebral blood flow as detected by SPECT. J Neurol 2005;252:78–83.
Figures
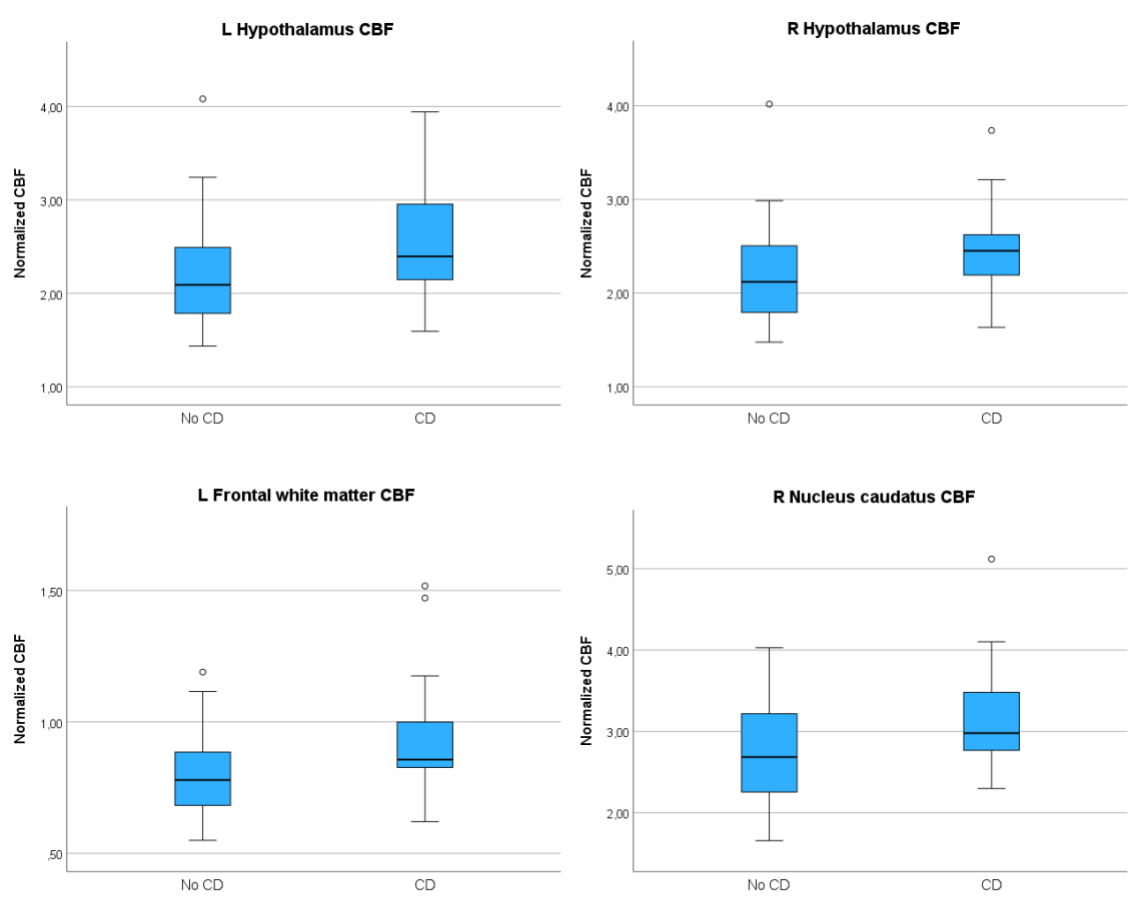
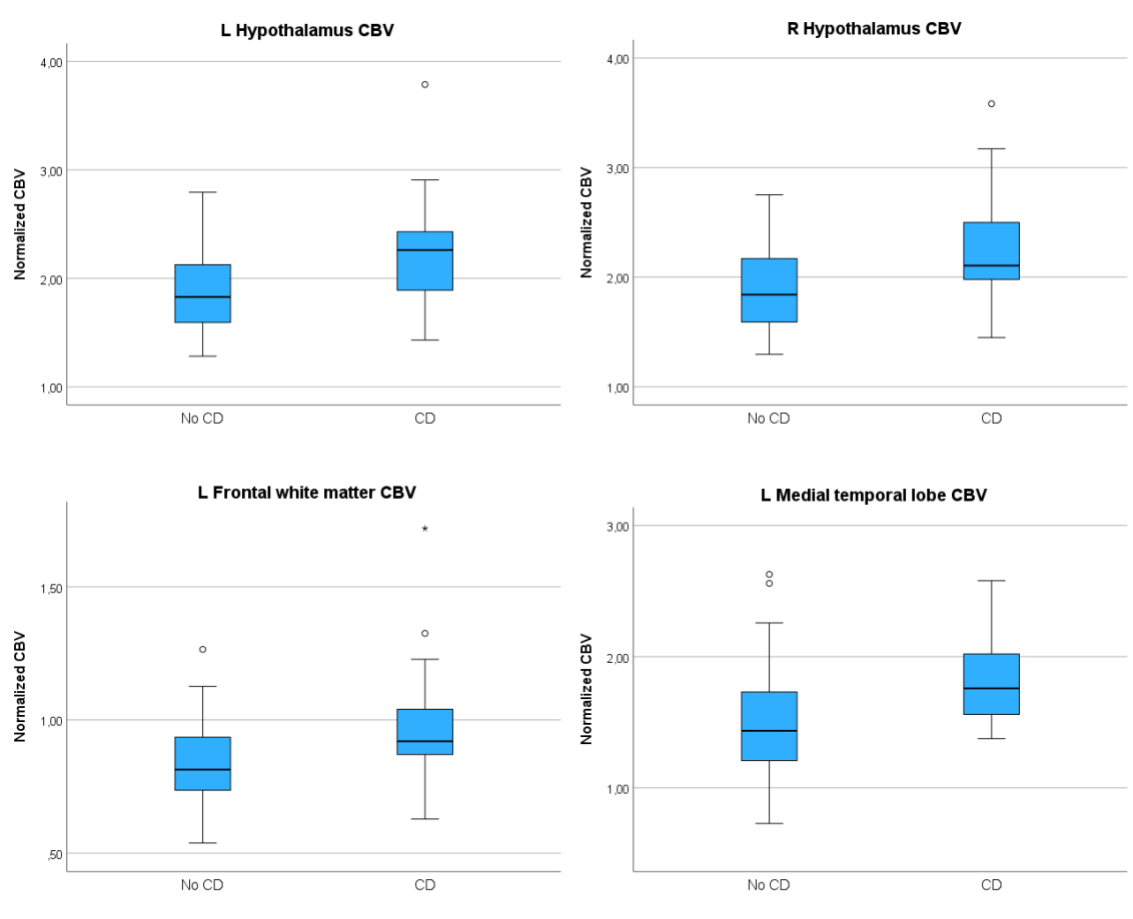
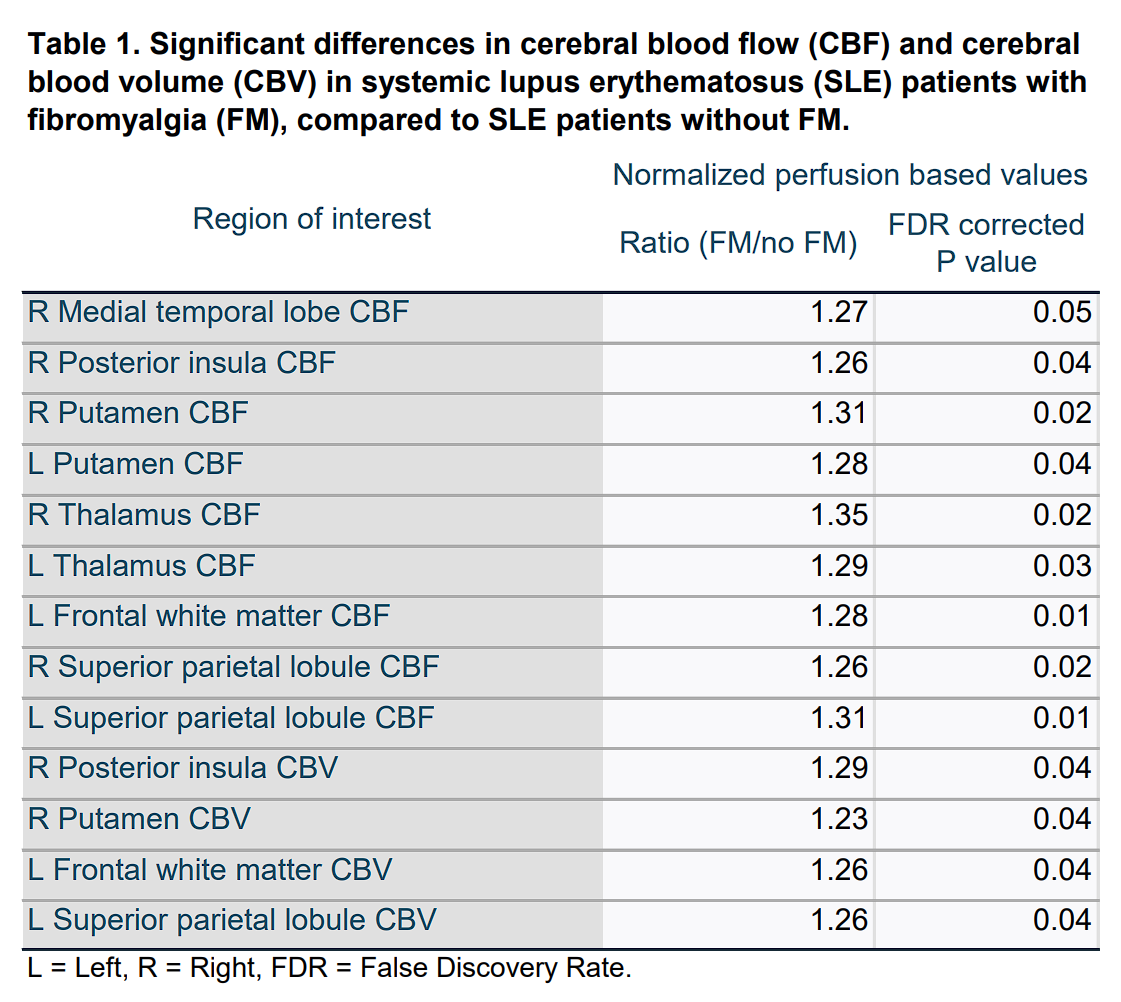
Table 1. Significant differences in cerebral blood flow (CBF) and cerebral blood volume (CBV) in systemic lupus erythematosus (SLE) patients with fibromyalgia (FM), compared to SLE patients without FM. L = Left, R = Right, FDR = False Discovery Rate.