2496
Improved Vessel-Encoded Dynamic Arterial Spin Labeling (VE-DASL) for Vascular Territory Mapping1Institute of Science and Technology for Brain-inspired Intelligence, Fudan University, Shanghai, China, 2Philips Healthcare, Shanghai, China, 3Key Laboratory of Computational Neuroscience and Brain-Inspired Intelligence (Fudan University), Ministry of Education, Shanghai, China
Synopsis
Keywords: Data Processing, Perfusion, ASL
Motivation: VE-DASL is promising in achieving fast vascular territory mapping by using short labeling duration and post-labeling delay, but the accuracy is limited, especially in the border zones.
Goal(s): To achieve a robust vascular territories separation using VE-DASL.
Approach: We adopted optimal encoding scheme and simulated the signal for each territory. The voxels that best matched the simulated signal were identified and their signal was used as the reference. The vascular territories were obtained using matrix inversion or correlation analysis.
Results: The proposed method achieved results comparable to VEASL and demonstrated the capability to differentiate the four vascular territories.
Impact: We improved VE-DASL by using OES and the proposed vessel-decoding method. This approach enabled us to achieve results comparable to VEASL while offering the potential for extension to more complex vascular scenarios.
Introduction
Distinguishing arterial blood supply to specific brain regions is crucial in the assessment of collateral flow in steno-occlusive cerebrovascular diseases. Super-selective ASL and vessel-encoded arterial spin labeling (VEASL) are currently the two primary non-invasive techniques for vascular territory mapping1,2. However, they both suffer from long scan time. The previously proposed vessel-encoded dynamic ASL (VE-DASL) is promising in achieving very fast cerebral territory mapping due to the use of short labeling duration (LD) and post-labeling delay (PLD)3. However, the accuracy of VE-DASL is limited, especially in the border zones. This study proposed to improve VE-DASL by using optimal encoding scheme (OES)4 and a novel vessel-decoding method. This approach enabled us to achieve results comparable to VEASL while offering the potential for extension to more complex vascular scenarios.Materials and methods
Sequence designThe IRB-approved experiment was performed on a 3T Philips Ingenia CX scanner. As shown in Figure 1, leveraging Philips' Pride tool, we developed an interaction interface to select the 4 vessels of interest (i.e. two ICAs and two VAs) on a 2D image at the labeling plane on the console. The OES algorithm was implemented for automated encoding pattern calculation, which included the angles of the in-plane gradient, encoding spacing, and encoding offset to determine the label conditions. Several non-selective cycles were added to the beginning and end of the sequence in order to enhance the robustness of vessel-decoding.
Image acquisition
Traditional VEASL, 2D VE-DASL and 3D VE-DASL with OES labeling patterns were scanned on one healthy volunteer. The imaging parameters were as follows. Traditional VEASL: 2D EPI readout, 20 slices, LD 1650 ms, PLD 1575 ms, voxel size 2.75×2.75×5 mm3. VE-DASL: LD 800 ms, flip angle 25°, PLD 70 ms for 3D TFEPI readout, 10 ms for 2D multislice EPI readout, OES labeling pattern, each pattern repeated ten times, and the whole labeling scheme was repeated twice (see Figure 1), resulting in a total of 160 volumes.
Vessel-decoding methods
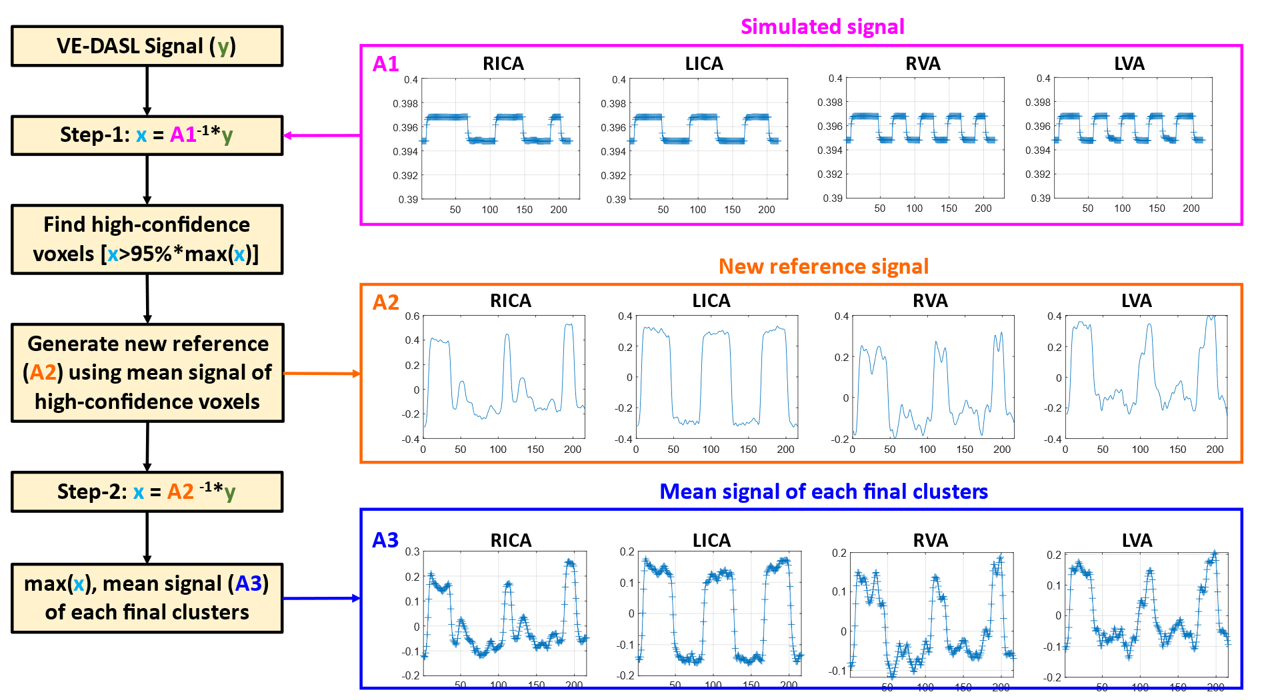
A two-compartment model was used to simulate the signal evolution in a particular territory as the initial reference3, where the labeling efficiency was directly obtained through the OES. As shown in Figure 2, the signal preprocessing steps included spatial denoising, temporal smoothing, and detrending. Then, we first identified the high-confidence voxels that best matched the simulated signal using matrix inversion. In the second step, we replaced the simulated signal with the mean signal of these high-confidence voxels, which served as the new reference, and further classified the signal for each voxel. In the preprocessing, the impact of detrending was assessed on the final vessel-decoding. In the second step of processing, we compared the matrix inversion approach and maximum-correlation approach for vessel-decoding. The proposed novel vessel-decoding approach was also compared to the direct k-means clustering algorithm and simple matrix inversion, while using identical preprocessing procedures.
Results
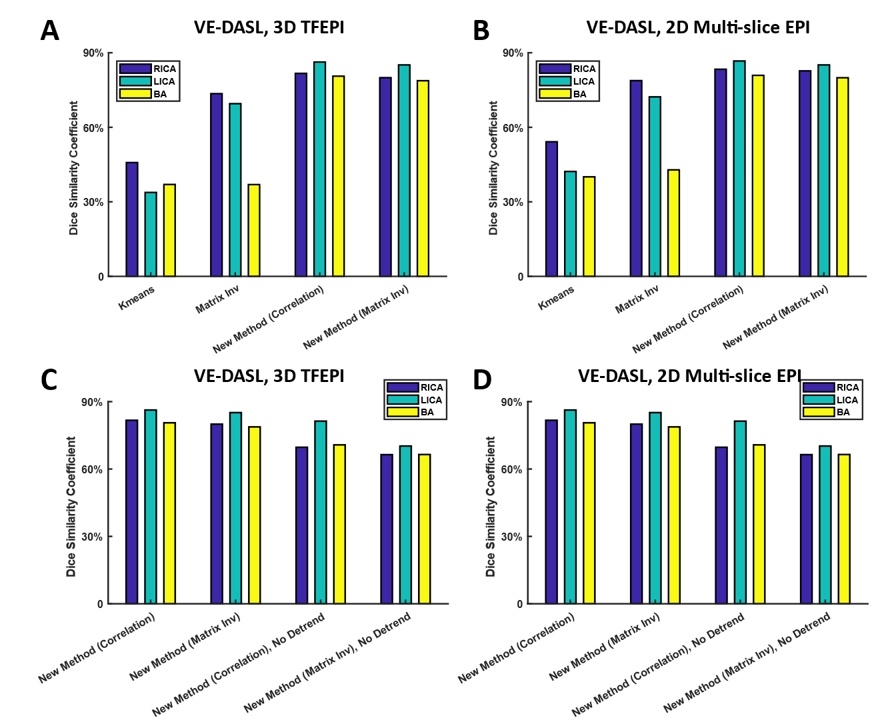
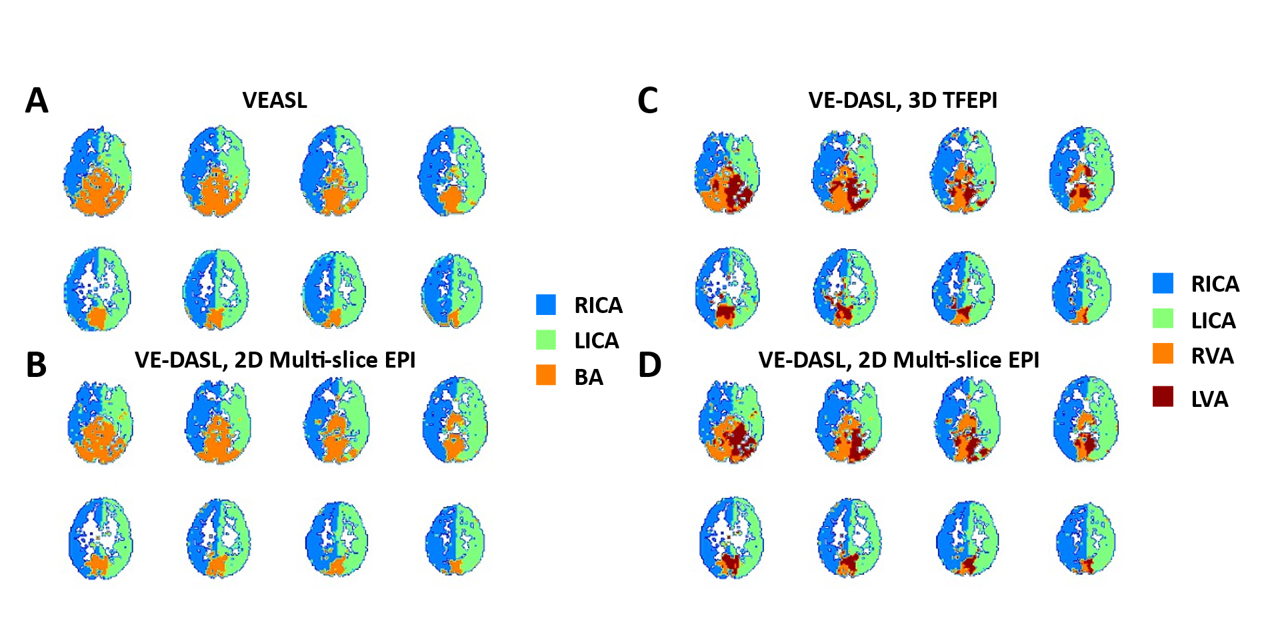
The proposed approach showed a significant improvement compared to traditional clustering or matrix inversion methods, particularly in the posterior circulation territory, achieving a Dice coefficient of approximately 80% with the VEASL used as gold standard, as shown in Figure 3A and 3B. As shown in Figure 3C and 3D, detrending could improve the Dice coefficient by about 10%. Additionally, the maximum-correlation approach was slightly better than the matrix inversion approach in all vascular territories. The resulting territory maps are shown in Figure 4. The proposed method achieves results comparable to VEASL and demonstrates the capability to differentiate between the four vascular territories.Discussion and conclusions
Among the evaluated approaches, the use of detrending in preprocessing, followed by maximum-correlation analysis using the high-confidence voxels’ signals as reference, seems to result in the best vessel-decoding for VE-DASL. The large discrepancy between the high-confidence voxels’ signals and the simulated signals is likely due to the presence of partial labeling in the OES design. In real scan, factors such as B1 inhomogeneity and head motion may contribute to this discrepancy. In future work, efforts will be made to optimize the OES design and ASL scan parameters, aiming to bring each labeling arteries as close as possible to the label and control states. On the flip side, our proposed method to some extent can mitigate the impact of partial labeling, resulting in a more robust territory mapping, although further validation is needed.Acknowledgements
This work was supported by Natural Science Foundation of Shanghai (22ZR1403900).References
1. Wong, E.C. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magnetic Resonance in Medicine 58, 1086-1091 (2007).
2. Helle, M., et al. Superselective pseudocontinuous arterial spin labeling. Magnetic Resonance in Medicine 64, 777-786 (2010).
3. Zhang, X., Ghariq, E., Hartkamp, N.S., Webb, A.G. & van Osch, M.J.P. Fast cerebral flow territory mapping using vessel encoded dynamic arterial spin labeling (VE-DASL). Magnetic Resonance in Medicine 75, 2041-2049 (2016).
4. Berry, E.S.K., Jezzard, P. & Okell, T.W. An Optimized Encoding Scheme for Planning Vessel-Encoded Pseudocontinuous Arterial Spin Labeling. Magnetic Resonance in Medicine 74, 1248-1256 (2015).
Figures