2494
Development of HR-VWI Score to Explore the Characteristics Intracranial Artery Involvement in Relation to Intracranial Lesions in TA1Beijing AnZhen Hospital, Beijing, China
Synopsis
Keywords: Blood Vessels, Neuroinflammation
Motivation: Previous studies have not developed a high-resolution wall imaging scoring system for TA patients with intracranial vascular involvement to explore its relationship with intracranial lesions.
Goal(s): Develop a HR-VWI score to demonstrate the relationship between the score and incidence of intracranial lesions.
Approach: Integrated the degree of luminal stenosis, the pattern and degree of vessel wall enhancement and the number of affected vessels on HR-VWI into a HR-VWI score.
Results: TA patients with intracranial lesions had higher HR-VWI scores and HR-VWI scores performed well in distinguishing TA patients with intracranial lesions from those without intracranial lesions.
Impact: HR-VWI is a powerful tool for physicians to visualize the condition of vessels by showing the various changes in the vesseel walls and a more reliable method of diagnosing intracranial arterial stenosis than TOF-MRA.
Objective:
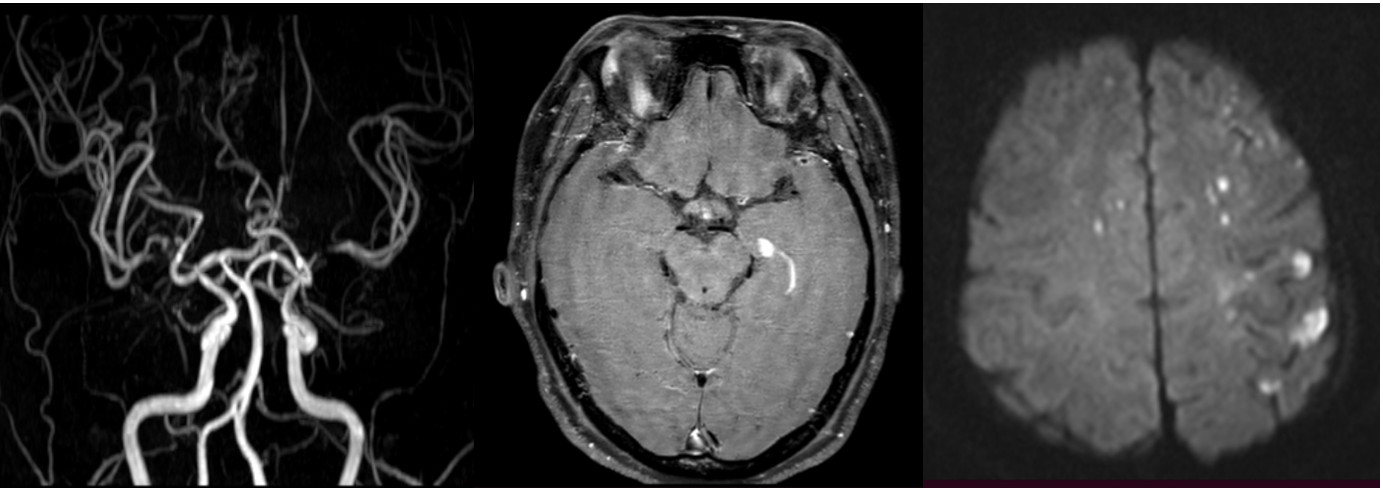
Takayasu arteritis (TA) can lead to inflammatory reactions in the intracranial vessel wall, thereby affecting the normal blood circulation of intracranial arteries, causing pathological changes in intracranial arteries, and consequently increasing the risk of cerebrovascular diseases. Early detection of intracranial artery involvement can control the progression of cerebrovascular disease and is significant in terms of clinical prognosis. Currently, high-resolution vessel wall imaging (HR-VWI) is increasingly being used for detecting different stages of inflammation and endothelial injury caused by TA often results in thickening of the vessel wall. However, it remains unclear whether HR-VWI characteristics are associated with intracranial lesions. The study aimed to describe the characteristics of intracranial artery (IA) involvement in patients with TA on HR-VWI and develop a HR-VWI score to demonstrate the relationship between IA involvement and incidence of intracranial lesions defined as acute cerebral infarction, encephalomalacia foci, cerebral hemorrhage, lacunar infarction, or white matter demyelination. The risk factors associated with the development of intracranial lesions in TA have also been explored.Methods
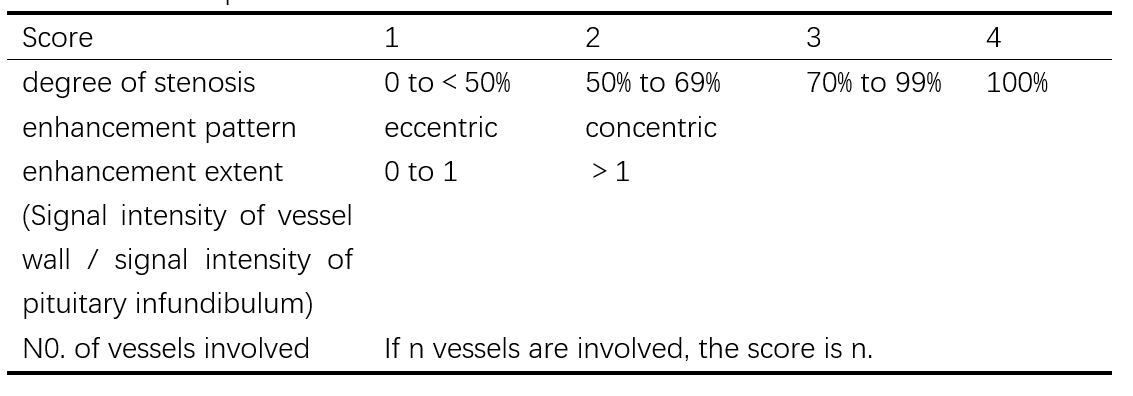
The study retrospectively reviewed the images of 60 patients identified TA who underwent HR-VWI from July 2019-July 2023. They were divided into two groups: with intracranial lesions group and without intracranial lesions group. Clinical characteristics were compared between two groups to identify possible causes of the intracranial lesions. Analyzed the degree of luminal stenosis, the pattern and degree of vessel wall enhancement and the number of affected vessels on HR-VWI. The HR-VWI detailed quantitative scores were as follows: firstly, score 1, 2, 3 and 4, respectively, for mild, moderate, severe luminal stenosis and occlusive; secondary, 1 point for eccentric enhancement and 2 points for concentric enhancement; thirdly, enhancement of vessel wall but less than that of the pituitary stalk is scored as one point, while more than that of the pituitary stalk is scored as two points; finally, the number of vessels involved is the number of points. Integrated the above scoring details into one HR-VWI score to explore the relationship with incidence of intracranial lesions.Results
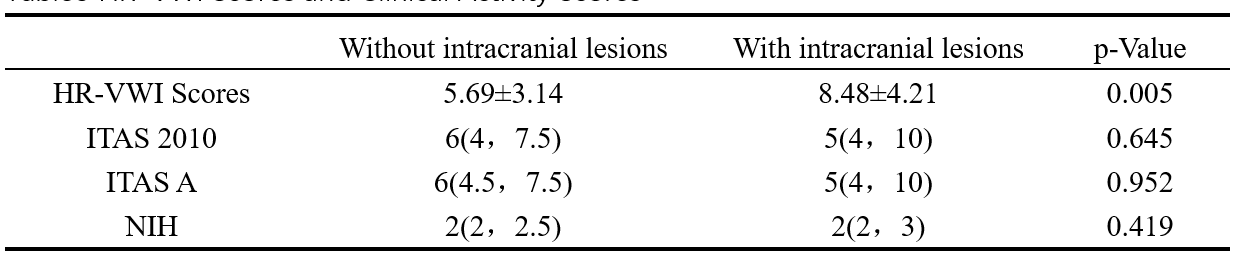
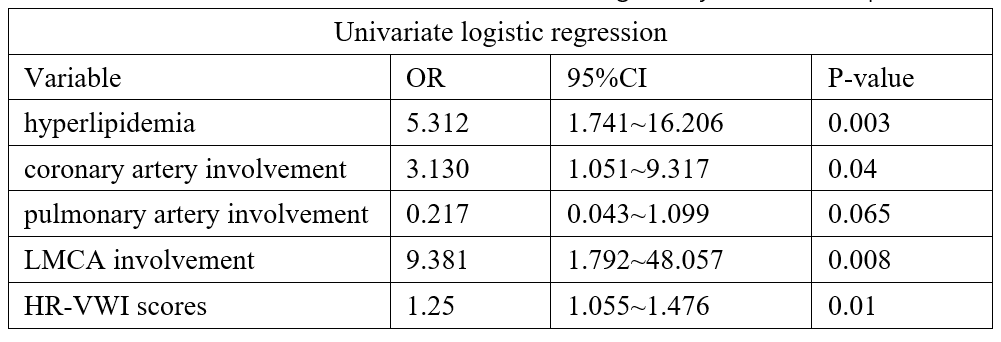
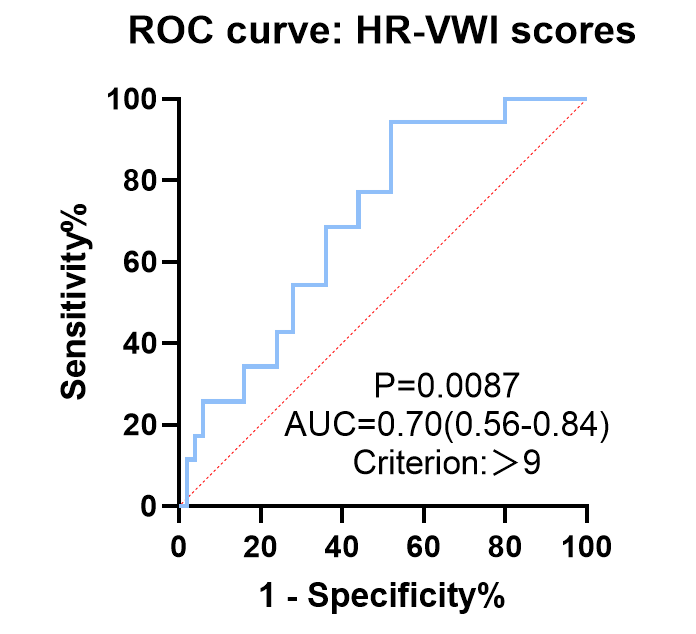
In the 60 TA patients (90%femal, median age was 39.75±10.38years), 25(41.7%) with intracranial lesions, while 35(58.3%) without intracranial lesions. Significant differences in left middle cerebral artery (LMCA) and left anterior cerebral artery (LACA) involvement between the group with and without intracranial lesions (MCA:36.0% vs 5.7%, p=0.008; ACA:20% vs 0, p=0.022). TA patients with intracranial lesions had higher HR-VWI scores compared to the group without intracranial lesions (8.48±4.21 vs 5.69±3.14,p=0.05). Taking>9 as the optimal cut-off for the HR-VWI score , we obtained the maximal Youden index with an area under the ROC curve (AUC) of 0.70. The results of logistic regression analysis indicated that TA patients who had hyperlipidemia [odds ratio (OR), 5.31; 95% confidence interval (CI): 1.74–16.21; P=0.003],coronary artery involvement (OR, 3.13; 95% CI: 1.05–9.32; P=0.04), LMCA involvement (OR, 9.38; 95% CI: 1.79–48.06; P=0.008), and a high HR-VWI score(OR, 1.25; 95% CI: 1.06–1.48; P=0.01) were more likely to develop intracranial lesions.Conclusion
Intracranial artery involvement was not uncommon in TA patients. The group of TA patients with intracranial lesions had higher HR-VWI scores and HR-VWI scores performed well in distinguishing TA patients with intracranial lesions from those without intracranial lesions. Hyperlipidemia, coronary artery involvement, LMCA involvement and high HR-VWI score may be the potential risk factors for presence of intracranial lesions in TA patients.Acknowledgements
First of all, I would like to give my heartfelt thanks to my tutor, whose suggestions and encouragement have given me much insight into these translation studies.I am also extremely grateful to all my friends and classmates who have kindly provided me assistance and companionship in the course of preparing this paper. Finally, I am really grateful to all those who devote much time to reading this thesis and give me much advice, which will benefit me in my later study.References
[1] Svensson C, Eriksson P, Zachrisson H. Vascular ultrasound for monitoring of inflammatory activity in Takayasu arteritis [J]. Clinical physiology and functional imaging, 2020, 40(1): 37-45.
[2]Bond K M, Nasr D, Lehman V, et al. Intracranial and Extracranial Neurovascular Manifestations of Takayasu Arteritis [J]. AJNR American journal of neuroradiology, 2017, 38(4): 766-72.
[3]Kong F, Huang X, Su L, et al. Risk factors for cerebral infarction in Takayasu arteritis: a single-centre case-control study [J]. Rheumatology (Oxford, England), 2021, 61(1): 281-90.
[4] Yang L, Zhang H, Jiang X, et al. Clinical Features and Outcomes of Takayasu Arteritis with Neurological Symptoms in China: A Retrospective Study [J]. The Journal of rheumatology, 2015, 42(10): 1846-52.
[5]Bolaman Z, Yavasoglu I, Kadikoylu G, et al. Takayasu arteritis with intracranial involvement mimicking epilepsy: case report and review of the literature [J]. Internal medicine (Tokyo, Japan), 2011, 50(12): 1345-8.
[6]Schäfer V S, Jin L, Schmidt W A. Imaging for Diagnosis, Monitoring, and Outcome Prediction of Large Vessel Vasculitides [J]. Current rheumatology reports, 2020, 22(11): 76.
[7]Kato Y, Terashima M, Ohigashi H, et al. Vessel Wall Inflammation of Takayasu Arteritis Detected by Contrast-Enhanced Magnetic Resonance Imaging: Association with Disease Distribution and Activity [J]. PloS one, 2015, 10(12): e0145855.
[8]Arend W P, Michel B A, Bloch D A, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis [J]. Arthritis and rheumatism, 1990, 33(8): 1129-34.
[9]Yuan C, Parker D L. Three-Dimensional Carotid Plaque MR Imaging [J]. Neuroimaging clinics of North America, 2016, 26(1): 1-12.
[10] Sundaram S, Kumar P N, Sharma D P, et al. High-Resolution Vessel Wall Imaging in Primary Angiitis of Central Nervous System [J]. Annals of Indian Academy of Neurology, 2021, 24(4): 524-30.
[11] Kathuveetil A, Sylaja P N, Senthilvelan S, et al. Vessel Wall Thickening and Enhancement in High-Resolution Intracranial Vessel Wall Imaging: A Predictor of Future Ischemic Events in Moyamoya Disease [J]. AJNR American journal of neuroradiology, 2020, 41(1): 100-5.
[12] Ryoo S, Cha J, Kim S J, et al. High-resolution magnetic resonance wall imaging findings of Moyamoya disease [J]. Stroke, 2014, 45(8): 2457-60.
[13]Lee G Y, Jang S Y, Ko S M, et al. Cardiovascular manifestations of Takayasu arteritis and their relationship to the disease activity: analysis of 204 Korean patients at a single center [J]. International journal of cardiology, 2012, 159(1): 14-20.
Figures