2492
Development of automated vessel labeling for multiple cerebrovascular conditions based on magnetic resonance angiography1Department of Biomedical Imaging and Radiological Sciences, National Yang Ming Chiao Tung University, Taipei, Taiwan, 2School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan, 3Department of Neurology, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwan, 4Brain Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan, 5Institute of Clinical Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan, 6Division of Translational Research, Department of Medical Research, Taipei Veterans General Hospital, Taipei, Taiwan, 7Department of Radiology, Taipei Veterans General Hospital, Taipei, Taiwan
Synopsis
Keywords: Blood Vessels, Blood vessels
Motivation: Intracranial vessels exhibit significant variations stemming from anatomical distinctions and pathological conditions; therefore, automated vessel labeling is challenging.
Goal(s): We aimed to investigate the performance of automated intracranial vessel labeling for multiple cerebrovascular conditions, including normal structure, severe stenosis, occlusion, aging, and calcification.
Approach: We developed an automated vessel labeling model solely based on the dataset with normal structures (202 real cases) and evaluated its labeling performance in different cerebrovascular conditions (50 real and 200 simulated cases).
Results: The proposed model showed high generalization across cerebrovascular conditions with an average labeling accuracy of 0.82, which could facilitate future quantitative analysis of vessel anomalies.
Impact: This study contributes to the application of automated intracranial vessel labeling in different cerebrovascular conditions and offers insights into the model applications in future quantitative analysis for the diagnosis and treatment of vessel anomalies.
Background and Purpose
The automated labeling of intracranial vessels with their corresponding anatomic nomenclature is pivotal for the quantitative analysis of cerebrovascular diseases. Intracranial vessels exhibit considerable variations owing to both natural anatomical differences and pathological conditions. Accordingly, automated labeling of intracranial arteries is a formidable challenge 1, 2. While previous works have shown feasibility in vessel labeling based on healthy populations, the applications for cerebrovascular diseases with variations of artery structures have not been fully explored 3, 4. In addition, the available dataset for the evaluation of anatomical labeling in cerebrovascular diseases is very limited. In this study, we collected 252 MR angiography (MRA) scans and constructed a simulated dataset of various cerebrovascular conditions, including severe stenosis, occlusion, aging, and calcification. We aimed to develop an automated vessel labeling model solely based on the dataset with normal structures and evaluated its labeling performance in different cerebrovascular conditions.Materials and Methods
This study retrospectively collected a dataset comprising 252 MRA scans with normal vessel structures obtained from Taipei Veterans General Hospital. The 3D Time-of-Flight MRAs (3D-TOF MRAs) were acquired utilizing a 3.0-T GE Discovery MR750 scanner, with imaging parameters set at a repetition time (TR) of 25 ms, echo time (TE) of 2.9 ms, and a voxel dimension of 0.39 x 0.39 x 0.50 mm³. Ethical approval for the study was obtained from the local Institutional Review Board. The representation of intracranial arterial structures was achieved through the depiction of arterial centerlines.We extracted centerlines of cerebral vessels using our previously proposed Vessel Analysis Platform and manually labeled them by experienced neuroscientists as ground truth and approved by neuroradiologists. Based on the vessel centerlines extracted from real cases, we constructed a simulated dataset composed of various cerebrovascular conditions (Figure 1). To simulate severe stenosis (50 cases), five consecutive points were removed within randomly selected arterial segments. To simulate vessel occlusion (50 cases), all points of vessel centerlines beyond a randomly defined location were removed. To simulate the tortuosity in aging vessels (50 cases), the centerlines were subject to random shifts within a range of 0.1 mm. To simulate vessel calcification (50 cases), a randomly selected portion of certain centerlines was subject to random shifts within a range of 0.1 mm.
We developed an automated vessel labeling model solely based on the training dataset with normal structures (202 of 252 real cases) and evaluated its labeling performance in the test dataset (the remaining 50 real cases with normal structures and 200 simulated cases for four vessel conditions). To perform vessel labeling, we used PointNet++ as the vessel centerline classification model on the MATLAB interface of the R2023a version. PointNet++ hierarchically processes individual points in a point cloud to extract local features from point clusters and groups those features to capture global and local features from the entire point cloud 5. The labeling accuracy of six artery segments, including bilateral anterior cerebral artery (ACA), middle cerebral artery (MCA), and posterior cerebral artery (PCA), was evaluated in different cerebrovascular conditions. The detailed study workflow is shown in Figure 2.
Results and Discussion
Table 1 presents the performance of automated vessel labeling for each artery segment with different vessel conditions (mean accuracy = 0.82), and the model inference time was around 2.4 to 2.6 seconds for each case. Figure 3 demonstrates satisfactory labeling accuracy for the conditions of normal structure (0.88), severe stenosis (0.85), aging (0.83), and calcification (0.84). Inferior performance in the condition of occlusion (0.69) was observed, indicating the proposed model was less adaptable to drastic vascular alterations. Accordingly, continuous collection of vascular occlusion datasets may benefit the development of automated vessel labeling for ischemic stroke studies. Figure 4 shows representative cases of four different cerebrovascular conditions. Overall, the proposed model could effectively identify the bilateral ACA, MCA, and PCA within 3 seconds for each case. Our results indicated that the proposed automated vessel labeling model has high generalization across cerebrovascular conditions which could facilitate future quantitative analysis of vessel anomalies.Conclusions
This study developed an automated vessel labeling model with satisfactory accuracy in five cerebrovascular conditions, including normal structure, severe stenosis, occlusion, aging, and calcification. Our finding contributes to the quantitative cerebrovascular analysis and offers insights into future applications in the diagnosis and treatment of cerebrovascular diseases.Acknowledgements
This study was supported by Ministry of Science and Technology of Taiwan (MOST110-2634-FA49-005 and MOST 109-2314-B-010-022-MY3) and Veterans General Hospitals and University System of Taiwan Joint Research Program (VGHUST112-G1-3-3).References
- Kayembe, K.N., M. Sasahara, and F. Hazama, Cerebral aneurysms and variations in the circle of Willis. Stroke, 1984. 15(5): p. 846-50.
- Alpers, B.J., R.G. Berry, and R.M. Paddison, Anatomical studies of the circle of Willis in normal brain. AMA Arch Neurol Psychiatry, 1959. 81(4): p. 409-18.
- Chen, L., et al., Quantification of morphometry and intensity features of intracranial arteries from 3D TOF MRA using the intracranial artery feature extraction (iCafe): A reproducibility study. Magn Reson Imaging, 2019. 57: p. 293-302.
- Robben, D., et al., Simultaneous segmentation and anatomical labeling of the cerebral vasculature. Med Image Anal, 2016. 32: p. 201-15.
- Qi, C.R., et al., Pointnet++: Deep hierarchical feature learning on point sets in a metric space. 2017. 30.
Figures
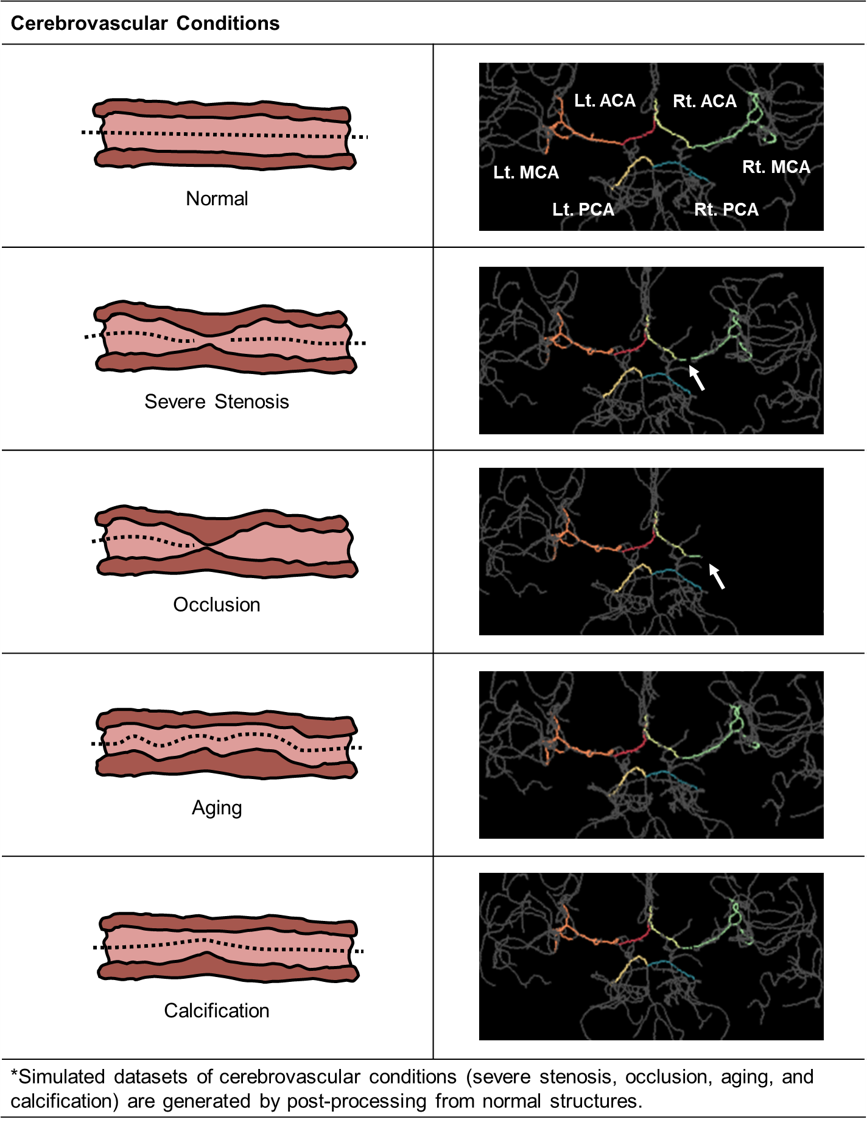
Figure 1. Schematic diagram of cerebrovascular condition simulation.
(A) To simulate severe stenosis (50 cases), five consecutive points were removed within randomly selected arterial segments. (B) To simulate vessel occlusion (50 cases), all points of vessel centerlines beyond a randomly defined location were removed. (C) To simulate the tortuosity in aging vessels (50 cases), the centerlines were subject to random shifts within 0.1 mm. (D) To simulate vessel calcification (50 cases), a randomly selected portion of certain centerlines was subject to random shifts within 0.1 mm.
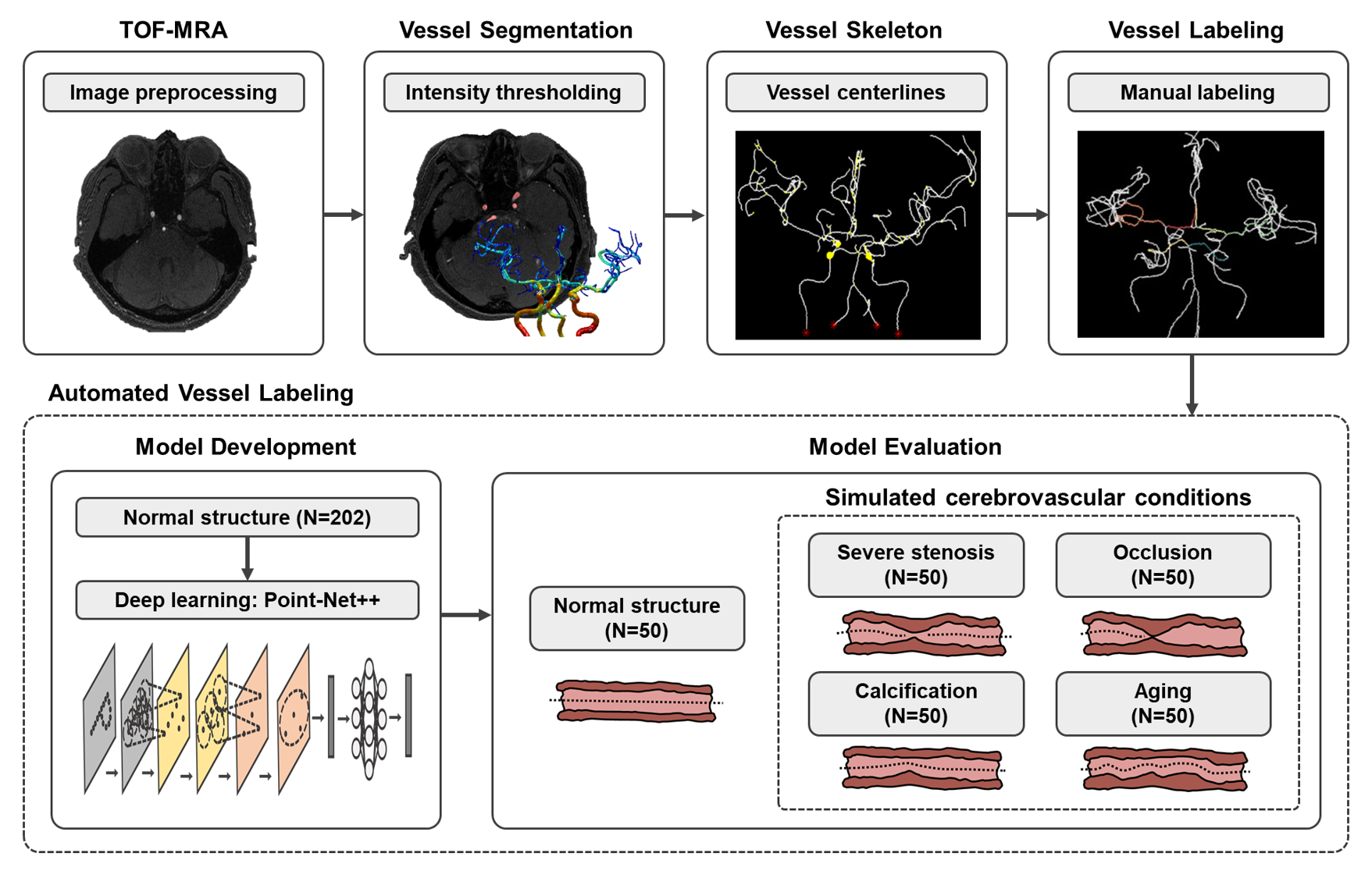
Figure 2. Flowchart of image processing and model development.
The vessel segmentation was based on intensity thresholding. The representation of intracranial arterial structures was achieved through the depiction of artery centerlines. Labeling of bilateral ACA, MCA, and PCA was used as ground truth. The vessel labeling was performed by PointNet++ for vessel centerline classification. The development of automated vessel labeling model was solely based on the dataset with normal structures and evaluated its labeling performance in different cerebrovascular conditions.
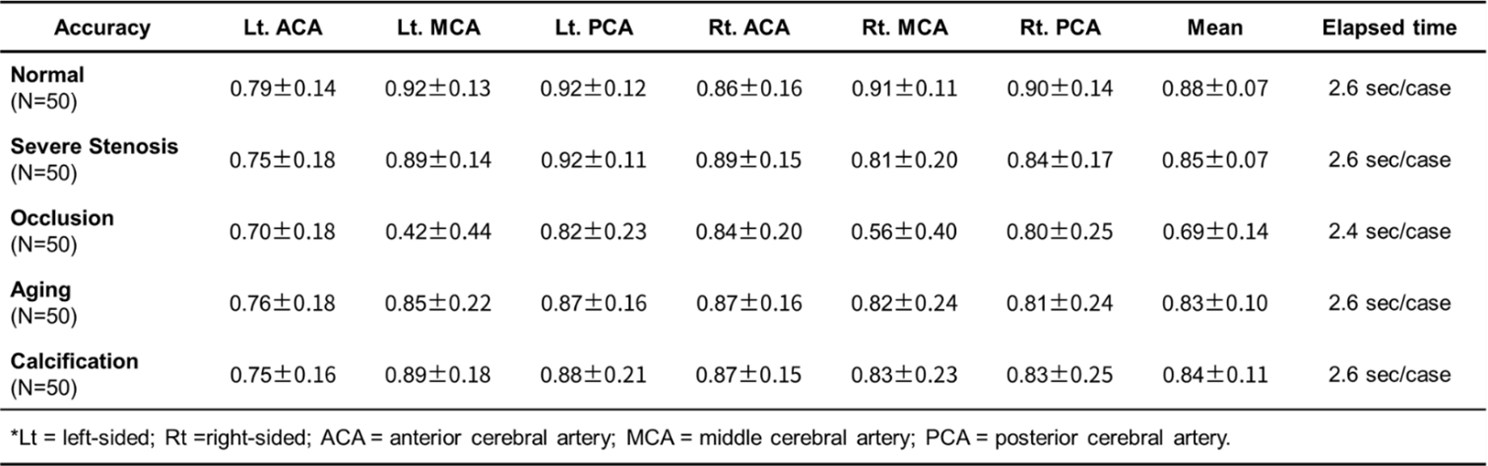
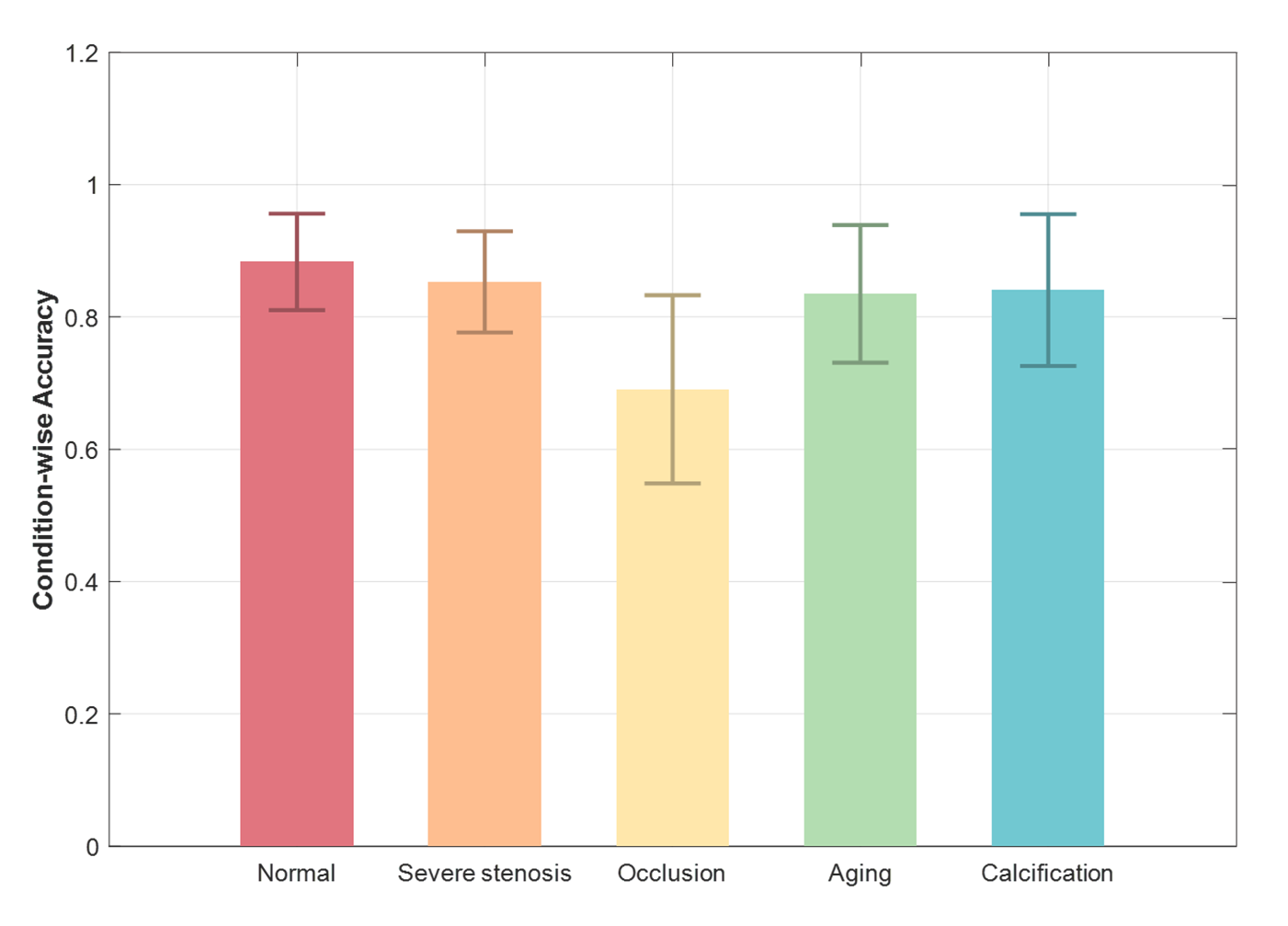
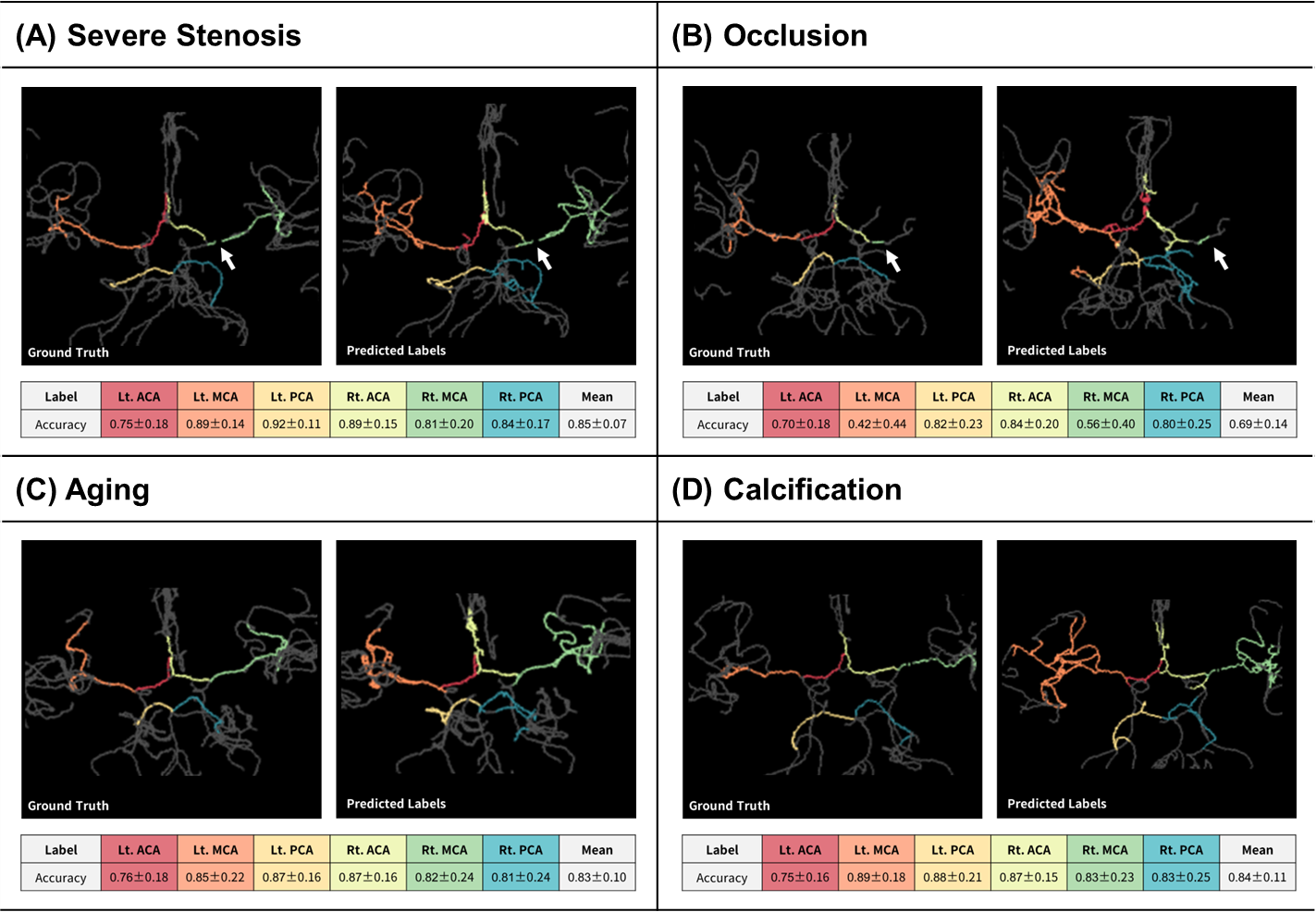
Figure 4. Representative cases of automated vessel labeling.
(A) The simulated dataset with severe stenosis achieved accuracy with a mean of 0.85. (B) The simulated dataset with vessel occlusion achieved accuracy with a mean of 0.69. (C) The simulated dataset with aging vessels achieved accuracy with a mean of 0.83. (D) The simulated dataset with vascular calcification achieved accuracy with a mean of 0.84. Lt = left-sided; Rt =right-sided; ACA = anterior cerebral artery; MCA = middle cerebral artery; PCA = posterior cerebral artery.