2488
Evaluation of Acceleration Methods for Clinical T1-weighted (T1w) Vessel Wall Imaging1Department of Radiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States, 2Siemens Medical Solutions USA Inc, Malvern, PA, United States, 3Department of Radiology, Keck School of Medicine of USC, Los Angeles, CA, United States, 4Department of Radiology, University Hospital of Würzburg, Würzburg, Germany, 5Hôpital Fondation Adolphe de Rothschild, Paris, France, Metropolitan, 6Department of Radiology, The University of Vermont Medical Center, Burlington, VT, Canada, 7Department of Radiology, University of Washington, Medical Center, Seattle, WA, United States
Synopsis
Keywords: Blood Vessels, Blood vessels, Vessel Wall Imaging, Accelerated Acquisition, Compressed Sensing
Motivation: Clinical VWI scans demand high spatial resolutions, which lead to extended acquisition times, potentially causing limited field-of-view (FOV), motion artifacts, and patient burden.
Goal(s): We evaluated FDA-approved acceleration methods for 3D T1w SPACE to develop optimized protocols for clinical VWI studies.
Approach: Compressed Sensing (CS) and CAIPI acceleration techniques optimized to reduce scan times and provide whole-head coverage were compared against our current GRAPPA accelerated limited-FOV clinical protocol.
Results: The whole-head FOV combined with CS yielded image quality comparable to our current clinical protocol but with almost half the scan time, promising significant reductions in lengthy clinical VWI protocols and patient burden.
Impact: Compressed Sensing enabled increased FOV imaging with substantially reduced scan times without significant loss of image quality compared to CAIPI and standard-of-care GRAPPA-accelerated techniques for a clinical T1-weighted vessel wall imaging protocol.
Introduction
Magnetic Resonance Imaging (MRI) for vessel wall assessment is crucial in diagnosing intracranial vasculopathies, differentiating among various conditions. Vessel wall MR imaging (VWI) demands high spatial resolutions with optimized tissue contrast, blood suppression, and motion robustness. Our health system employs a GRAPPA-accelerated 3D T1w-Sampling Perfection with Application optimized Contrasts using Different Flip Angle Evolution (SPACE) [1] sequence for clinical VWI. However, achieving the necessary submillimeter resolution necessitates extended acquisition times, leading to trade-offs in FOV coverage, motion artifacts, and patient burden. Previous studies using acceleration methods like CAIPI [2] and CS [3,4,5] demonstrated substantial scan time reductions. Nonetheless, these studies featured prototype sequences, limiting their clinical applicability. In this research, we assess FDA-approved acceleration methods for 3D T1w-SPACE, widely available in clinical scanners, including GRAPPA, CAIPI, and CS. Our goal is to identify suitable accelerated protocols for broader patient trials requiring clinical VWI exams.Method
We compared our standard clinical 3D T1w-SPACE protocol, using standard FOV GRAPPA R=2 (SFGRAPPA), with matched protocols that differed only in the use of CAIPI R=4 (SFCAIPI4, standard FOV CAIPI4), and CS R=7 (SFCS7, standard FOV CS7) accelerations. To shorten scan times, our standard clinical protocol incorporates a reduced FOV, truncating the left-right and anterior-posterior dimensions, as depicted in Figure 1a. This often leads to incomplete coverage of crucial cortical arteries for assessing embolic strokes, insufficient imaging of scalp arteries for temporal arteritis assessment, and the necessity of saturation pulses to reduce aliasing. To address these challenges, we also introduced "Large FOV" protocols with whole-head coverage and CS R=7 (LFCS7, large FOV CS7) and R=10 (LFCS10, large FOV CS10). Table 1 details the imaging parameters. Five healthy subjects underwent imaging with all five protocols using a 3.0 T MRI equipped with the vendor-supplied 20-channel head/neck coil (MAGNETOM PrismaFit, Siemens Healthineers). A 20-channel coil was chosen to replicate the hardware available across our health system's clinical scanners. Four neuroradiologists, experienced in VWI, independently reviewed 25 randomly presented scans. They employed a 4-point Likert scale to assess Perceived Signal-to-Noise Ratio (SNR) and Image Quality (1 = poor, 2 = fair, 3 = good, 4 = excellent). Vessel lumen and outer wall diameters of the basilar artery (BA) , bilateral internal carotid (ICA, supraclinoid segment), and middle cerebral arteries (MCA, M1 segment) were manually measured by one neuroradiologist in all studies. The study received approval from the local institutional review board.Results
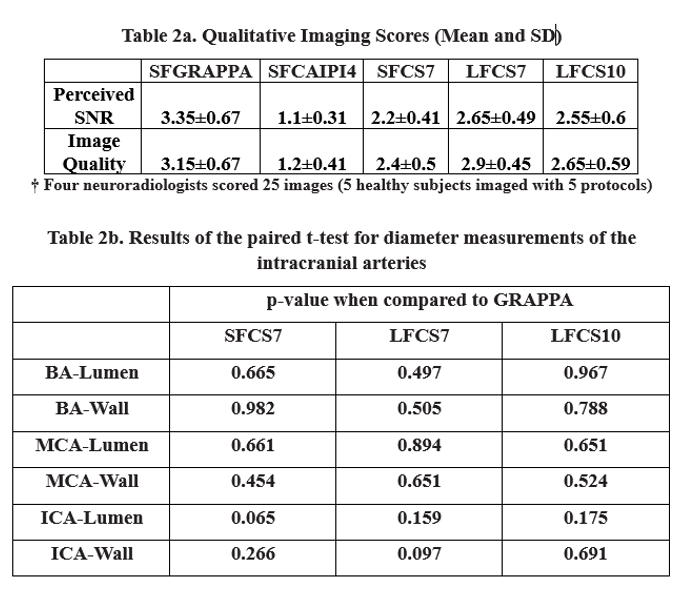
Figure 1b displays BA, ICA, and MCA images from healthy subjects. The SFCAIPI4 images exhibited low SNR towards the brain's center, as expected with the 20-channel coil. Differences in SNR between "standard" and "large" FOV CS-7 images were more pronounced in subjects with larger head circumferences, resulting in increased wrap artifacts in the "standard" FOV protocol. Perceived SNR and Image Quality by the four neuroradiologists are summarized in Table 2a and Figure 2. While none of the tested accelerated protocols surpassed the SFGRAPPA based on qualitative metrics, the LFCS7 protocol achieved the closest Perceived SNR and Image Quality scores (Perceived SNR mean difference: 0.7, t: -3.77, one-sided paired t-tests p=0.0006; Image Quality mean difference: 0.25, t: -1.39, one-sided p=0.174). This was followed by the LFCS10 (Perceived SNR mean difference: 0.8, t: -3.96, one-sided paired t-tests p=0.0003; Image Quality mean difference: 0.5, t: -2.5, one-sided p=0.017). Quantitative vessel lumen and outer wall diameter measurements are presented in Figure 3. Paired t-test analyses compared diameter measurements between SFGRAPPA and each of the other protocols (Table 2b). None of the compared protocols yielded statistically significant p-values, suggesting no systematic detectable quantitative differences in diameter measurements using these acceleration techniques.Discussion
All acceleration methods reduced scan time but displayed significant variations in image quality. Large-FOV CS scans received the highest Image Quality scores from neuroradiologists, closely matching our current clinical SFGRAPPA protocol. Additionally, Large-FOV protocols exhibited reduced wrap artifacts and provided extended coverage of brain/scalp tissue. This proves beneficial when imaging patients with larger head circumferences and when assessing intracranial cortical arteries in embolic stroke cases or scalp arteries in systemic vasculitis/temporal arteritis patients. Consequently, the Large-FOV CS protocol offers a 50% scan time reduction, enhancing clinical utility for comprehensive vasculopathy assessment.Conclusion
This study assessed FDA-approved acceleration methods for VWI using 3D T1w-SPACE. Qualitative and quantitative metrics from 5 healthy subjects' scans are evaluated from the acquired protocols. The findings indicate that CS-accelerated protocols closely match clinical standard image quality while significantly reducing scan time and enabling full-head coverage. Subsequent research will involve evaluating large-FOV CS protocols in a broader patient cohort to determine their efficacy in detecting vascular pathology.Acknowledgements
Sources of Funding: The work is supported by the American Heart Association Career Development Awards (938082 to JWS) and Institute of Translational Medicine and Therapeutics (JWS).References
1. Mugler III, J. P. (2014). Optimized three‐dimensional fast‐spin‐echo MRI. Journal of magnetic resonance imaging, 39(4), 745-767.
2. Qiu, Zhilang, et al. "Wave-CAIPI Highly Accelerated Whole-Brain Intracranial Vessel Wall Imaging." Proc. Intl. Soc. Mag. Reson. Med. 2020.
3. Zhu, Chengcheng, et al. "Accelerated whole brain intracranial vessel wall imaging using black blood fast spin echo with compressed sensing (CS-SPACE)." Magnetic Resonance Materials in Physics, Biology and Medicine 31 (2018): 457-467.
4. Fan, Zhaoyang, et al. "Whole-brain vessel wall imaging within 5 minutes using compressed sensing accelerated IR-SPACE." Proc. Intl. Soc. Mag. Reson. Med. Vol. 25. 2017.
5. Konstanze, Guggenberger, et al. "High-resolution Compressed-sensing T1 Black-blood MRI." Clinical Neuroradiology 31.1 (2021): 207-216.
Figures
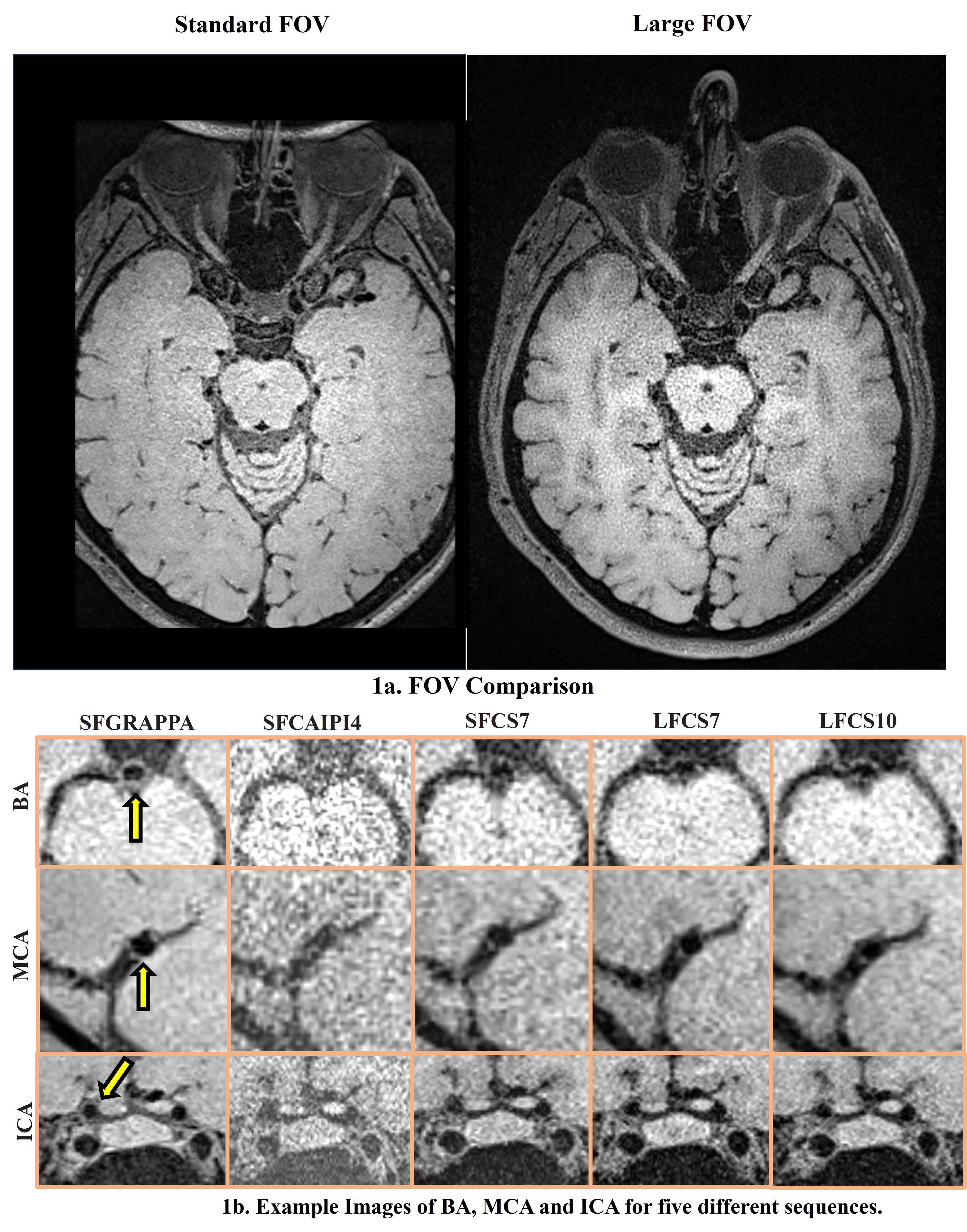
Figure 1a.(left) Standard Clinical Protocol uses a reduced field-of-view (FOV) which is truncated left-right and anterior-posterior when compared to larger FOV (right). 1b. Example images of the basilar artery (BA), middle cerebral artery (MCA), and internal carotid artery (ICA) at the level of the cavernous sinuses acquired from healthy subjects for the five protocols are shown. The yellow arrows indicate the vessel wall of the respective scored arteries.
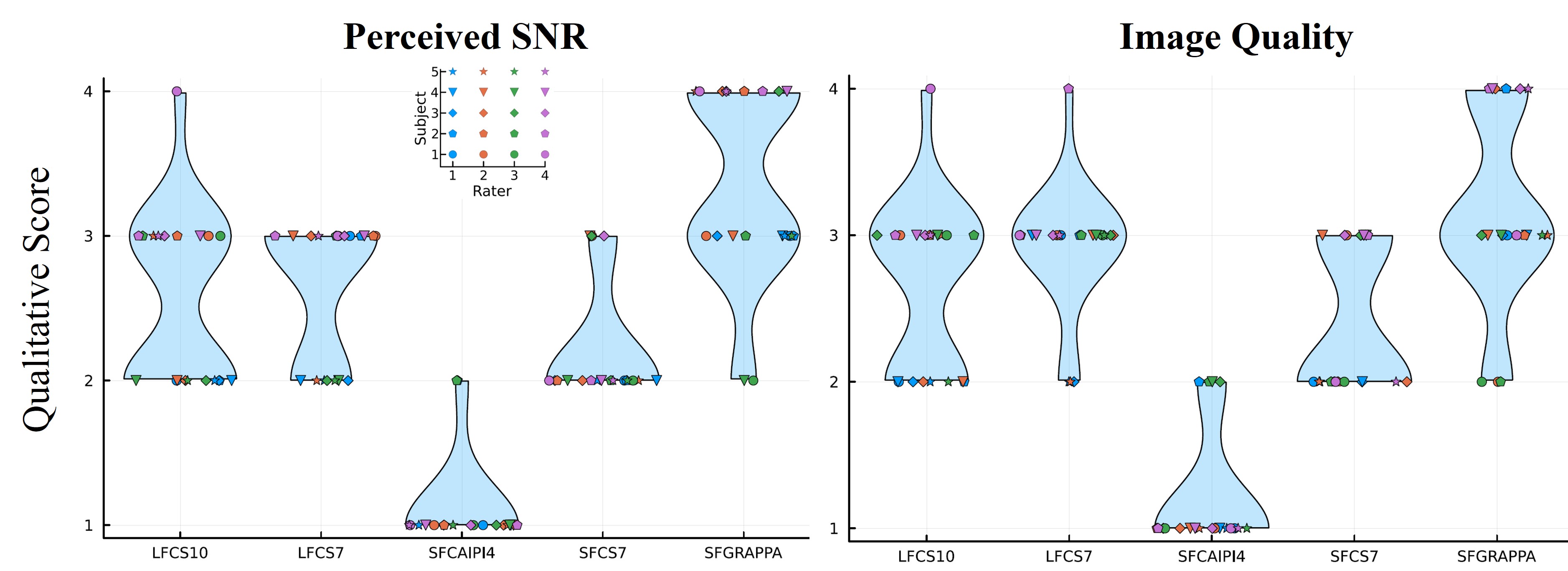
Qualitative Scores (Perceived signal to noise ratio, SNR and Image Quality) rated by 4 diagnostic neuroradiologists with vessel wall imaging (VWI) expertise. The x-axis shows the acquired five protocols, and the y-axis shows the qualitative score (1-4) from the four raters for five healthy subjects. Consensus in the ratings from all raters can be observed for all acquired sequences with very few outliers. Abbreviations : SFGRAPPA, Standard FOV GRAPPA, SFCAIPI4, Standard FOV CAIPI4, SFCS7, Standard FOV CS7, LFCS7, Large FOV CS7, LFCS10, Large FOV CS10
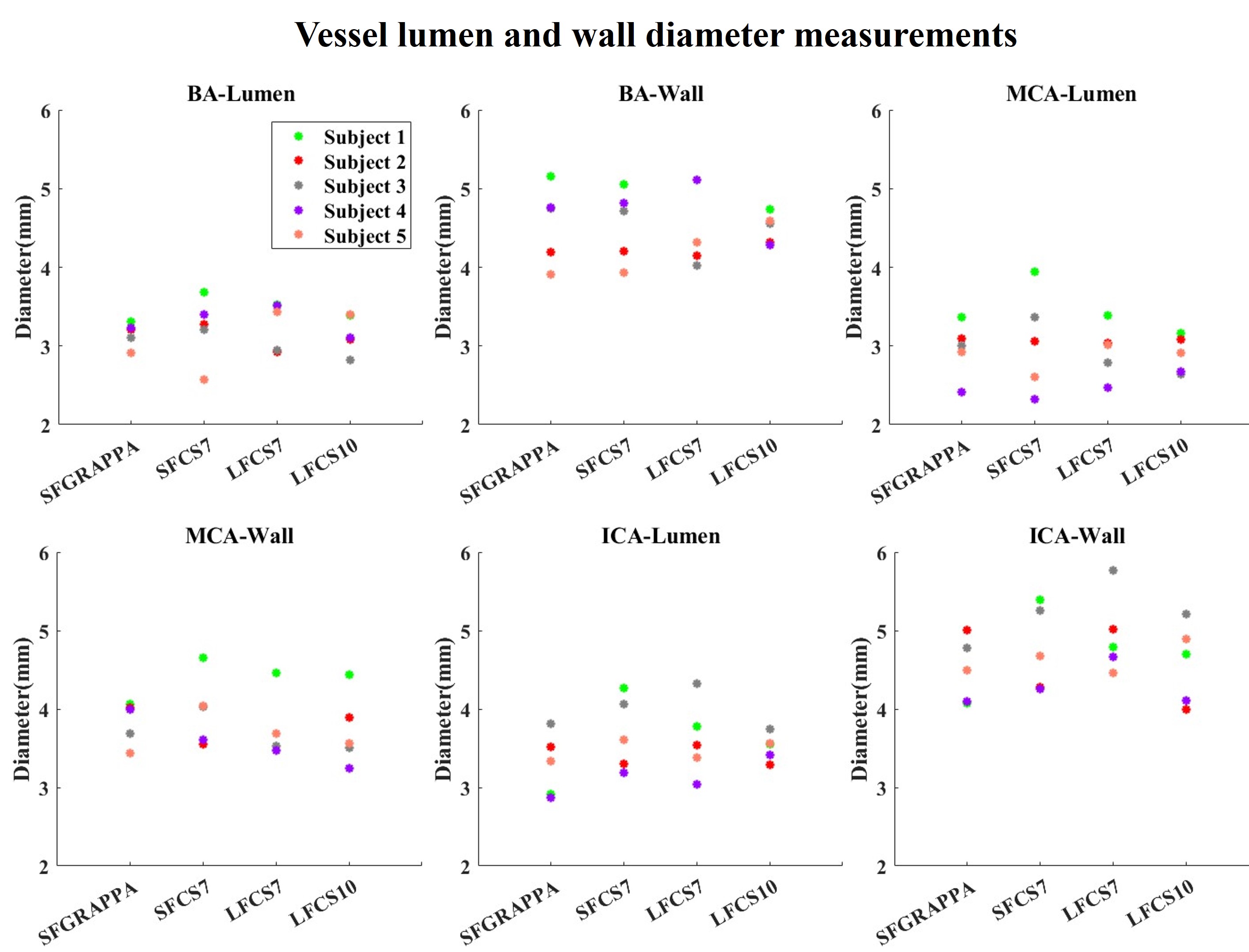
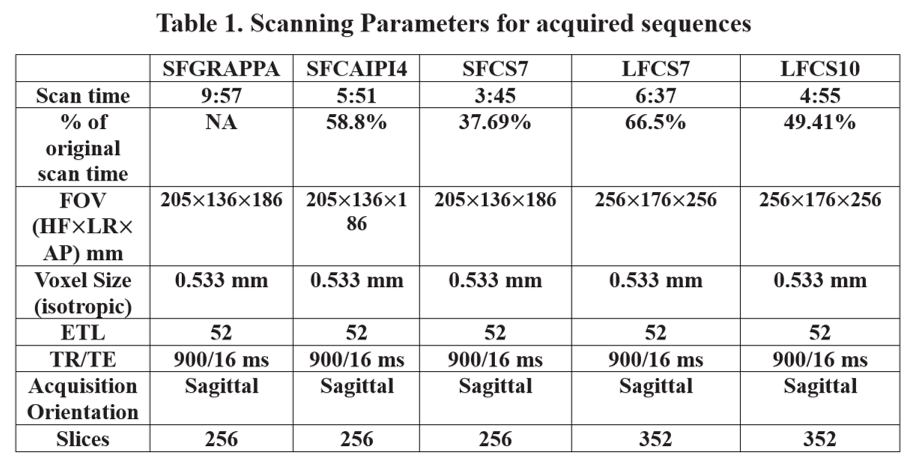
Table 1. Scanning Parameters. Abbreviations: ms, millisecond