2484
A COMPARATIVE STUDY BETWEEN 3D -SUSCEPTIBILITY-WEIGHTED IMAGING SEQUENCE &2D-T2WI GRADIENT ECHO SEQUENCE IN MRI BRAIN1RADIOLOGY, psims, near vijayawada, India, 2psims, near vijayawada, India
Synopsis
Keywords: Blood Vessels, Stroke, swI, T2 GRE
Motivation: Our study's aim is to aid radiologists in selecting the most appropriate MRI brain sequence, enhancing diagnostic accuracy.
Goal(s): We aimed to compare the effectiveness of SWI and GRE MRI sequences in detecting brain conditions like hemorrhages, calcifications, and vascular malformations
Approach: We conducted an observational study, analyzing patient data using SWI and GRE sequences on the same patient. Our approach focused on data analysis and assessing image quality.
Results: SWI is our preference for its sensitivity and reliability, but we recognize GRE's value when CT is already available. GRE efficiently distinguishes brain features, particularly beneficial for uncooperative patients.
Impact: Our study's results hold far-reaching implications. Healthcare professionals can benefit by using more accurate MRI-sequence, enabling better patient care. Researchers may explore novel avenues, enhancing scientific understanding, which is invaluable for medical progress.
INTRODUCTION:
SWI is a technique that leverages variations in magnetic susceptibility between different tissues to create image contrast. This approach is instrumental in revealing subtle differences in tissue properties, making it a valuable tool in medical imaging.On the other hand, GRE, or Gradient-echo, involves a clever manipulation of the free induction decay signal. It starts by applying an external dephasing gradient field across the specimen or tissue.Both SWI and GRE-sequences amplify local field variations due to calcification, iron deposition, and hemorrhage, resulting in signal loss1.The phase images of SWI play a crucial role in distinguishing calcifications, hemorrhage, and iron deposition. While gradient sequences that were available previously aided in identification by displaying a blooming effect, they fell short in differentiating these elements from each other.In this study, we will compare the time-consuming SWI-sequence, known for its superior quality, to the faster GRE-sequence in the detection of micro/macro-hemorrhages, calcifications, and vascular malformations.MATERIALS AND METHODS:
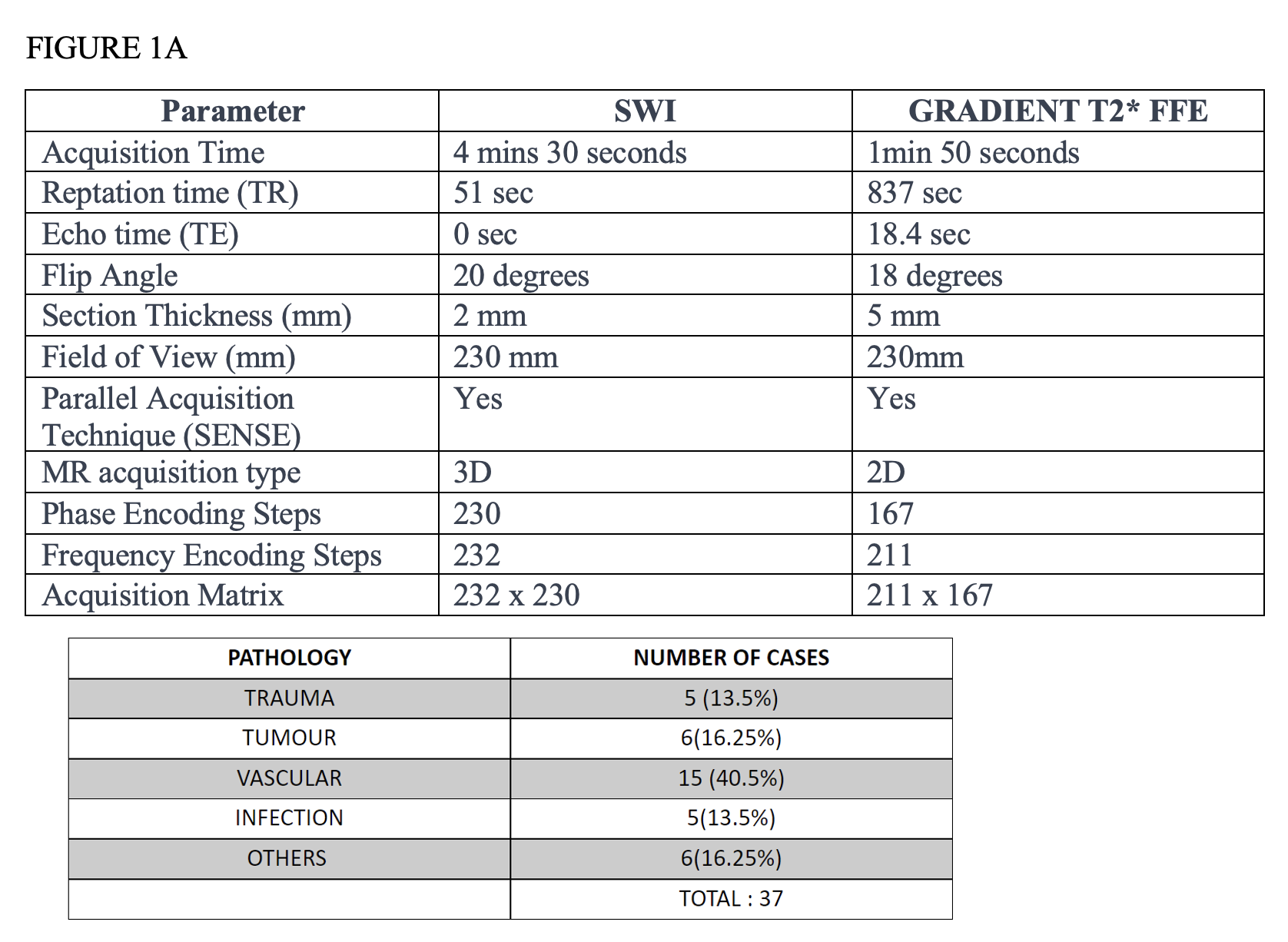
This observational study involved patients undergoing MRI-Brain using a Philips-1.5-Tesla-MRI scanner at Dr. PSIMS & RF Hospital. To address potential ambiguities in distinguishing calcifications from hemorrhage within phase images, we utilized a Siemens-16-slice-CT- scanner. The image acquisition technique employed is presented in Figure1RESULTS
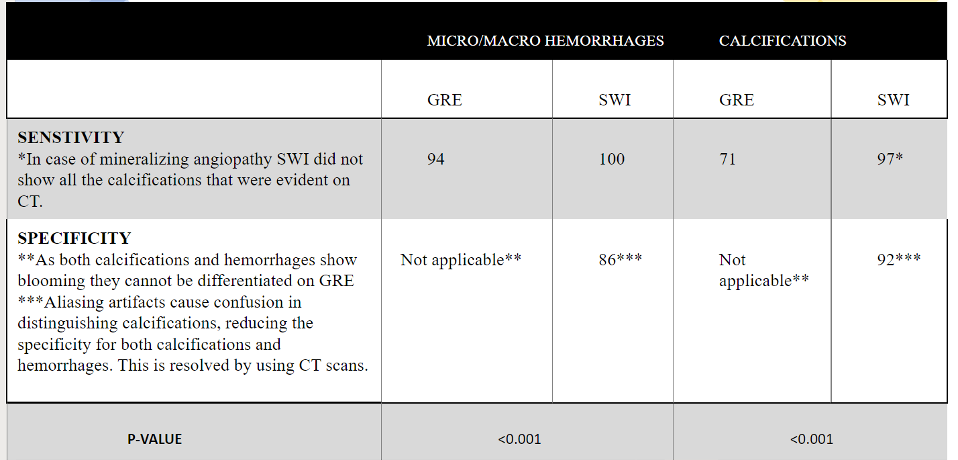
In this study, a total of 37 subjects were included. To ensure a smooth transition for radiologist readings during the digitization of the machine, we conducted both SWI and GRE-sequences for a two-month period.Results are depicted in the table figure 2
DISCUSSION
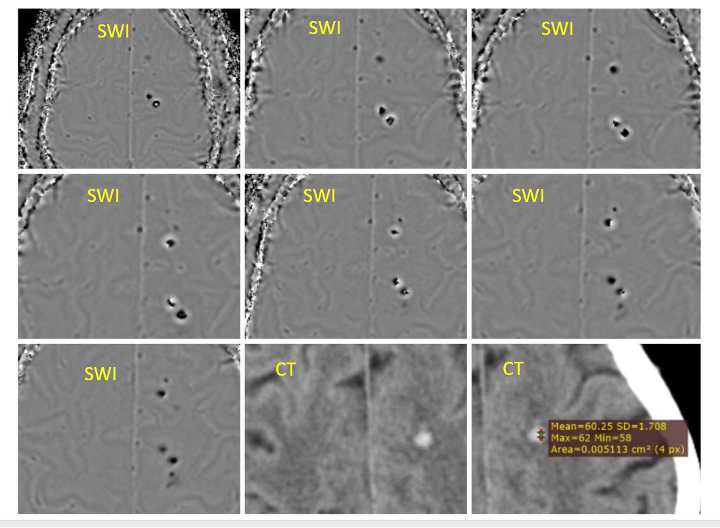
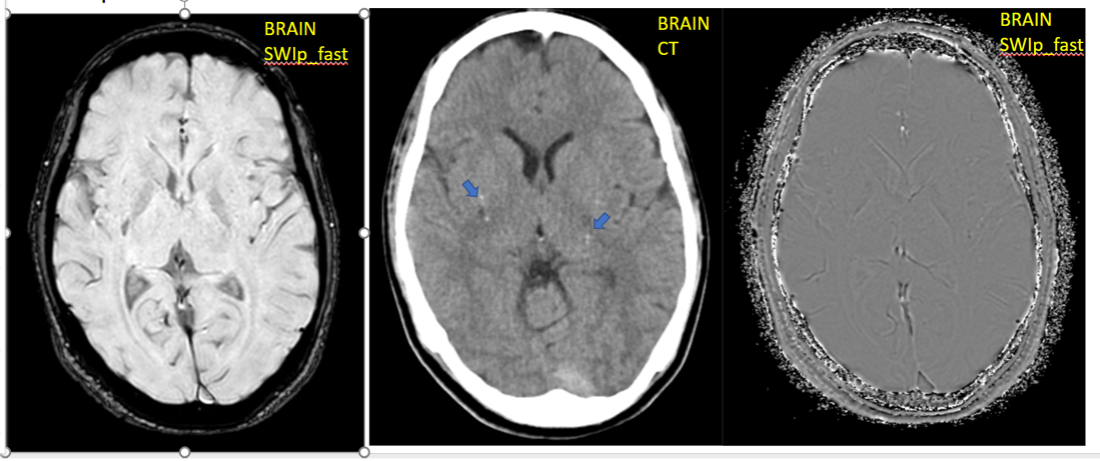
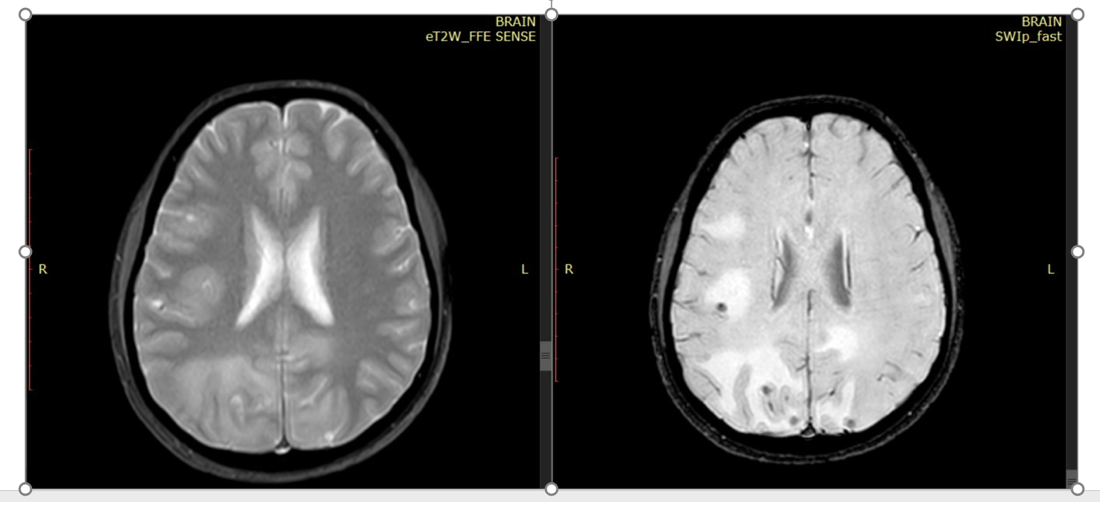
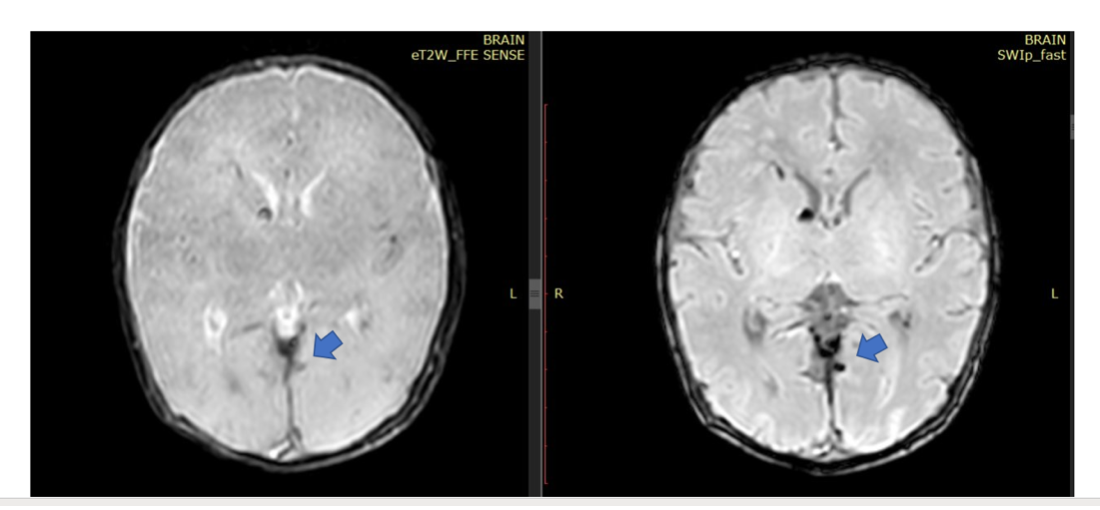
Clinicians should always be aware of the handedness used, as it affects the interpretation of phase shifts from blood (hemorrhage) vs. Calcium, A popular approach among radiologists is to compare vessels and or choroid plexus to determine the MRI's handedness. In our study, we employed a right-handed machine. Interpreting phase images can occasionally pose challenges, as macro-hemorrhages may be mistakenly perceived as calcifications. This necessitates correlation with CT-scans to address aliasing artifacts. Techniques like coronal reformatting and meticulous signal analysis at the edges can enhance accuracy and reliability. Our data indicates that SWI sequences outperform GRE-sequences in terms of sensitivity for detecting both hemorrhage and calcifications. Notably, hemorrhage is better visualized on SWI compared to GRE, and SWI detects a higher number of microhemorrhages as seen in fig 3&6. SWI imaging plays a pivotal role in detecting hemorrhage in traumatic brain injury. While moderate and severe injuries exhibit evident lesions on CT, mild cases are challenging to depict. Detecting microbleeds is vital for prognosis and legal perspectives, as SWI-like imaging reveals more lesions than CT or standard T2* with long-lasting visibility2,3. Our study findings demonstrate that SWI is highly sensitive for detecting and distinguishing hemorrhage and calcifications, especially when using Phase reconstructed images. These results align with the studies by Berberat et al4.When conducting an MRI brain protocol, if an SWI sequence is being performed, additional time spent on a GRE sequence may not be necessary, as SWI often provides more comprehensive information. However, the gradient sequence may suffice if a CT scan has already been conducted, reducing time constraints. It's important to note that in uncooperative patient scenarios, high-demand hospitals, or when CT is readily available, GRE may offer a quicker alternative. A significant finding in this article is the recognition that the SWI-sequence, while valuable in many respects, occasionally fails to identify calcifications in cases of mineralizing angiopathy. This limitation becomes apparent when comparing SWI results to the clear depiction of these calcifications on CT scans, as exemplified in fig 4. This underscores the importance of considering alternative imaging methods, such as CT, when evaluating mineralizing angiopathy-related calcifications, as SWI may not always provide the comprehensive information required for accurate diagnosis and assessment.. And Zafar et al. emphasized that the inclusion of SWI imaging alongside conventional MRI enhances lesion detection and scolex demonstration, particularly during the calcified stage of neurocysticercosis (NCC), without incurring additional costs. This underscores the importance of integrating SWI into conventional MRI protocols for improved NCC detection and diagnosis, as illustrated in fig 5. Another potential application of susceptibility imaging is in the context of vascular malformations. On SWI-images, the angioarchitecture of vascular malformations associated with bleeding is often obscured by blooming. While angioarchitecture is more clearly seen on gradient or conventional-sequences, SWI excels in visualizing supplying arteries and draining veins, as implied by Jagadeesan et al5.Conclusion
While we favor SWI for its sensitivity and reliability. We recognize the value of GRE sequences, especially in cases where CT is readily available. This aids in differentiating calcifications and allows for faster scanning, which is particularly beneficial in situations involving uncooperative patientsAcknowledgements
Sincere thanks to our head of the department Prof. chandrasekhar and our beloved professor Dr.Santha kumar and Dr.Bala Murali the NeuroradiologstReferences
1. Haller S, Haacke EM, Thurnher MM, Barkhof F. Susceptibility-weighted imaging: technical essentials and clinical neurologic applications. Radiology. 2021 Apr;299(1):3-26.
2. Beauchamp MH, Ditchfield M, Babl FE, Kean M, Catroppa C, Yeates KO, Anderson V. Detecting traumatic brain lesions in children: CT versus MRI versus susceptibility weighted imaging (SWI). Journal of neurotrauma. 2011 Jun 1;28(6):915-27.
3. Haller S. The Concept of “Number Needed to Image”. AJNR: American Journal of Neuroradiology. 2017 Oct;38(10): E79.
4. Berberat J, Grobholz R, Boxheimer L, Rogers S, Remonda L, Roelcke U. Differentiation between calcification and hemorrhage in brain tumors using susceptibility-weighted imaging: a pilot study. American Journal of Roentgenology. 2014 Apr;202(4):847-50.
5. Jagadeesan BD, Delgado Almandoz JE, Moran CJ, Benzinger TL. Accuracy of susceptibility-weighted imaging for the detection of arteriovenous shunting in vascular malformations of the brain. Stroke. 2011 Jan;42(1):87-92.
6. Wycliffe ND, Choe J, Holshouser B, Oyoyo UE, Haacke EM, Kido DK. Reliability in detection of hemorrhage in acute stroke by a new three‐dimensional gradient recalled echo susceptibility‐weighted imaging technique compared to computed tomography: a retrospective study. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2004 Sep;20(3):372-7.
7. MRI Questions & Answers; MR imaging physics & technology [Internet]. Questions and Answers in MRI. Available from: https://mriquestions.com/
8. Verma A, Awasthi R, Prasad KN, Soni N, Singh K, Paliwal VK, Lal H, Pandey CM, Gupta RK. Improved detection of parenchymal cysticercal lesions in neurocysticercosis with T2*-weighted angiography magnetic resonance imaging. Academic radiology. 2012 Aug 1;19(8):958-64.
9. Neyaz Z, Patwari SS, Paliwal VK. Role of FIESTA and SWAN sequences in diagnosis of intraventricular neurocysticercosis. Neurology India. 2012 Nov 1;60(6):646.
Figures