2432
Diffusion tensor cardiovascular magnetic resonance with monopolar spin-echo at ultra-high gradient strength Connectom scanner1National Heart and Lung Institute, Imperial College London, London, United Kingdom, 2Cardiovascular Magnetic Resonance Unit, The Royal Brompton Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3Cardiff University Brain Research Imaging Centre (CUBRIC), Cardiff University, Cardiff, United Kingdom, 4Siemens Healthcare Ltd, Camberly, United Kingdom
Synopsis
Keywords: Diffusion Acquisition, Cardiovascular
Motivation: Spin-echo (SE) diffusion tensor cardiovascular magnetic resonance (DT-CMR) imaging with monopolar diffusion encoding scheme is limited by bulk motion induced signal loss.
Goal(s): Utilization of ultrahigh gradient-strengths to substantially reduce the echo-time (TE) in monopolar SE DT-CMR.
Approach: A monopolar SE DT-CMR pulse-sequence was developed. An in-vivo study at ultra-high gradient-strength (180mT/m, Connectom scanner) for diastolic cardiac phases was conducted.
Results: With ultra-high gradient strength, it was possible to obtain reasonable DT-CMR data with monopolar SE in 60% of subjects. To our knowledge this is the first report of SE DT-CMR with monopolar diffusion encoding utilizing the ultra-high gradient-strength of the Connectom scanner.
Impact: The ability to acquire monopolar SE using ultra-high diffusion gradient strengths and the associated drastic reductions in TE may provide substantial increase in imaging efficiency for DT-CMR acquired in diastolic cardiac phases, a key step towards clinical translation.
Introduction
DT-CMR uniquely provides in-vivo quantitative characterisation of the myocardial microstructure1. For currently clinically available gradient strengths (40-80 mT/m) motion-compensated spin-echo (MCSE) methods are widely used for DT-CMR because of their ability to reduce the sensitivity of DT-CMR to bulk cardiac motion2. While some cardiac studies with non-motion compensated SE have been reported3, the lack of motion compensation typically leads to severe motion related signal loss and therefore incorrect DT-CMR results4,5. However, with ultra-high gradient strength, sufficient diffusion weighting with much shorter diffusion encoding gradients is possible reducing the sensitivity of non-motion compensated spin-echo sequences to bulk cardiac motion. Such techniques would provide substantial increases in SNR due to a reduction in TE relative to MCSE techniques.Here we present the first results obtained with monopolar SE DT-CMR, acquired with the ultra-high gradient strength available on the Siemens 3T Connectom (Gmax= 300mT/m).
Methods
A monopolar SE DT-CMR EPI sequence (Figure 1) with zonal excitation (via in-plane slice selection) was developed to utilize the ultrahigh gradient strength of the 3T Connectom scanner (Siemens Healthcare, Germany) accounting for patient safety (peripheral nerve and cardiac stimulation). A maximum gradient strength of 180mT/m was used for consistency with other ongoing DT-CMR studies at the Connectom. Six encoding directions at b=0, b=150 (2 averages) and b=500 s/mm2 (8 averages) were acquired at 2.8×2.8×8 mm3 (1.4x1.4x8 mm3 reconstructed). For efficient fat suppression a four-pulse binomial water excitation was used (1:3:3:1). A field of view = 360x135 mm2, TE = 31 ms, repetition-time= 2RR intervals, GRAPPAx2 was used. ECG triggered single short-axis DT-CMR acquisitions were conducted in the diastolic rest period.5 healthy volunteers (2 Female, 21-42 years) were recruited in accordance with ethical approval. All DT-CMR data was processed using an in-house MATLAB (Mathworks, MA) software tool.
An analysis (in MATLAB) based on the primary-eigenvalue (e1) in the left-ventricle (LV) myocardium was conducted for all five healthy volunteers to detect regions of motion induced signal loss in the images. This analysis was based on a maximum diffusivity = 3x10-3 mm2/s which is the diffusivity of free water at 37˚C, and e1 exceeding this value were assumed to correspond to pixels with motion-induced signal loss. Region-of-interests were drawn in the LV myocardium, excluding sub-epicardial and sub-endocardial pixels where blood contaminates the signal.
Results
Example monopolar SE diffusion-weighted images for b=0, 150 and 500 s/mm2 and six diffusion directions are displayed in Figure 2. The short TE results in visually apparent high SNR. The ultra-high gradient strength resulted in TE= 31ms compared to TE~74ms for similar MCSE protocols at 40mT/m maximum gradient strength6 (resulting in 2.5x less T2-weighted signal-loss).Acquisitions were deemed successful in 3/5 subjects. In the remaining 2 subjects DT-CMR results didn’t show the expected helix-angle (HA) pattern and the mean-diffusivity (MD) was higher than expected, indicating bulk motion artefacts. DT-CMR parameter maps calculated for all healthy human subjects in diastolic cardiac phases are shown in figure 3.
Figure 4 presents the analysis of e1 in the mid-LV myocardium. Acquisitions were deemed successful for the first three subjects. In these datasets 87–94% of pixels have e1 ≤ 3x10-3 mm2/s. Table 1 displays the results of motion-induced signal loss analysis, fractional anisotropy (FA), MD and second eigenvector (E2A). For subjects 4 and 5, more than 36% of pixels in LV myocardium presented an e1 > 3x10-3 mm2/s, further justifying their exclusion from the analysis.
Discussion and Conclusion
SE DT-CMR with monopolar diffusion encoding and without any motion-compensation has previously been challenging to obtain2,4,7. However, here we demonstrate that with ultra-high gradient strength, it is possible to obtain reasonable DT-CMR data with monopolar SE in 3/5 healthy subjects. To the best of our knowledge this is the first report of SE DT-CMR with monopolar diffusion scheme at the ultra-high gradient strengths of the Connectom scanner.In contrast to most MCSE studies, we acquired data in diastasis where amplitude of cardiac motion is minimum. While 2/5 acquisitions failed in this study, a similar proportion of MCSE studies fail in diastole using more standard gradient hardware5,7 and improvements in robustness might be obtained via trigger delay scouts9. While larger studies are required to validate these results, the improved robustness of monopolar SE with ultra-high diffusion gradient strengths and the associated drastic reductions in TE may provide substantial increases in imaging efficiency for DT-CMR acquired in diastolic cardiac phases, which is a key step towards clinical translation.
Acknowledgements
This work was funded by British Heart Foundation grant RG/19/1/34160.
References
1. Nielles-Vallespin et al., Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance, JACC 2017, 69(6).
2. Stoeck et al., Second-Order Motion-Compensated Spin Echo Diffusion Tensor Imaging of the Human Heart, MRM 2016, 75:1669–1676.
3. Xiang et al. Microvascular dysfunction associates with outcomes in hypertrophic cardiomyopathy: Insights from the Intravoxel incoherent motion MRI. JMRI 2022;28450.
4. Stoeck et al., Motion-Induced Signal Loss in In Vivo Cardiac Diffusion-Weighted Imaging. J MRI. 2020, 51(1):319-320.
5. Moulin et al., In Vivo Cardiac Diffusion Imaging Without Motion-Compensation Leads to Unreasonably High Diffusivity. J Magn Reson Imaging 2023, 58: 1990-1991.
6. Scott et al., An in-vivo comparison of stimulated-echo and motion compensated spin-echo sequences for 3 T diffusion tensor cardiovascular magnetic resonance at multiple cardiac phases. JCMR 2018, 20(1).
7. Welsh et al., Higher-Order Motion-Compensation for In Vivo Cardiac Diffusion Tensor Imaging in Rats, IEEE Trans Med Imaging 2015, 34(9):1843-53.
8. Khaliqueet al. Diffusion tensor cardiovascular magnetic resonance in hypertrophic cardiomyopathy: a comparison of motion-compensated spin echo and stimulated echo techniques. MAGMA 2020, 33(3):331-342.
9. Moulin et al., Probing cardiomyocyte mobility with multiphase cardiac diffusion tensor MRI, PLOS ONE 2020, 15(11): e0241996.
Figures
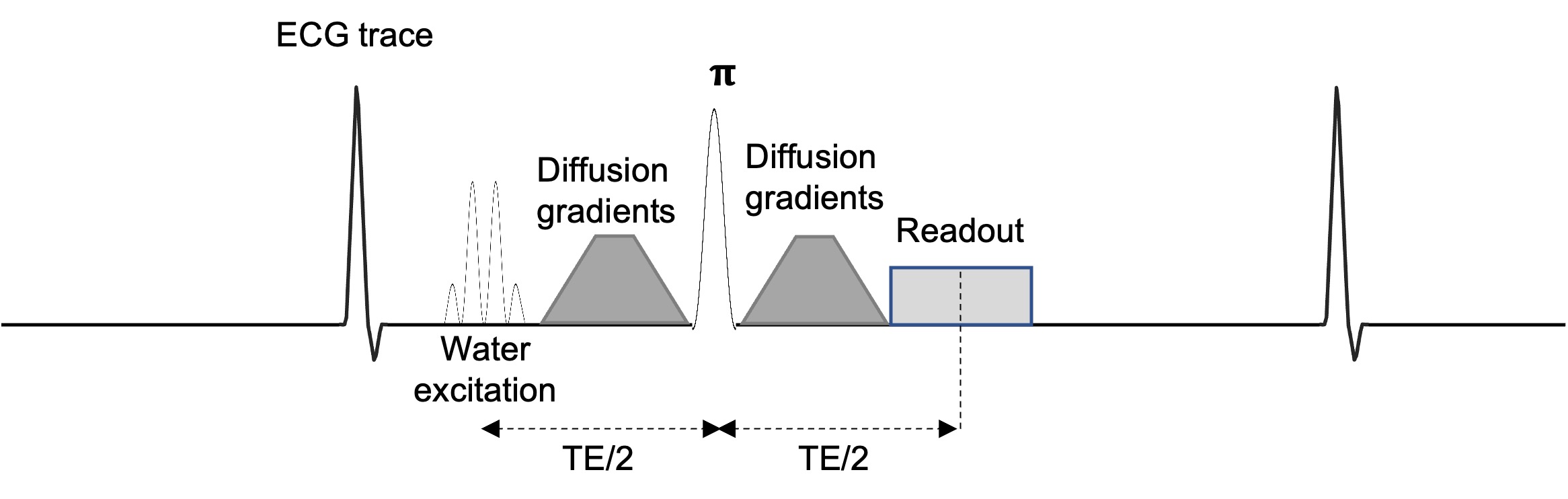
Figure1: Monopolar SE EPI DT-CMR pulse sequence at the Connectom scanner utilizing water excitation technique implemented with modified four binomial pulses (1:3:3:1) for efficient fat suppression. It was implemented for the maximum gradient strength of 180 mT/m.
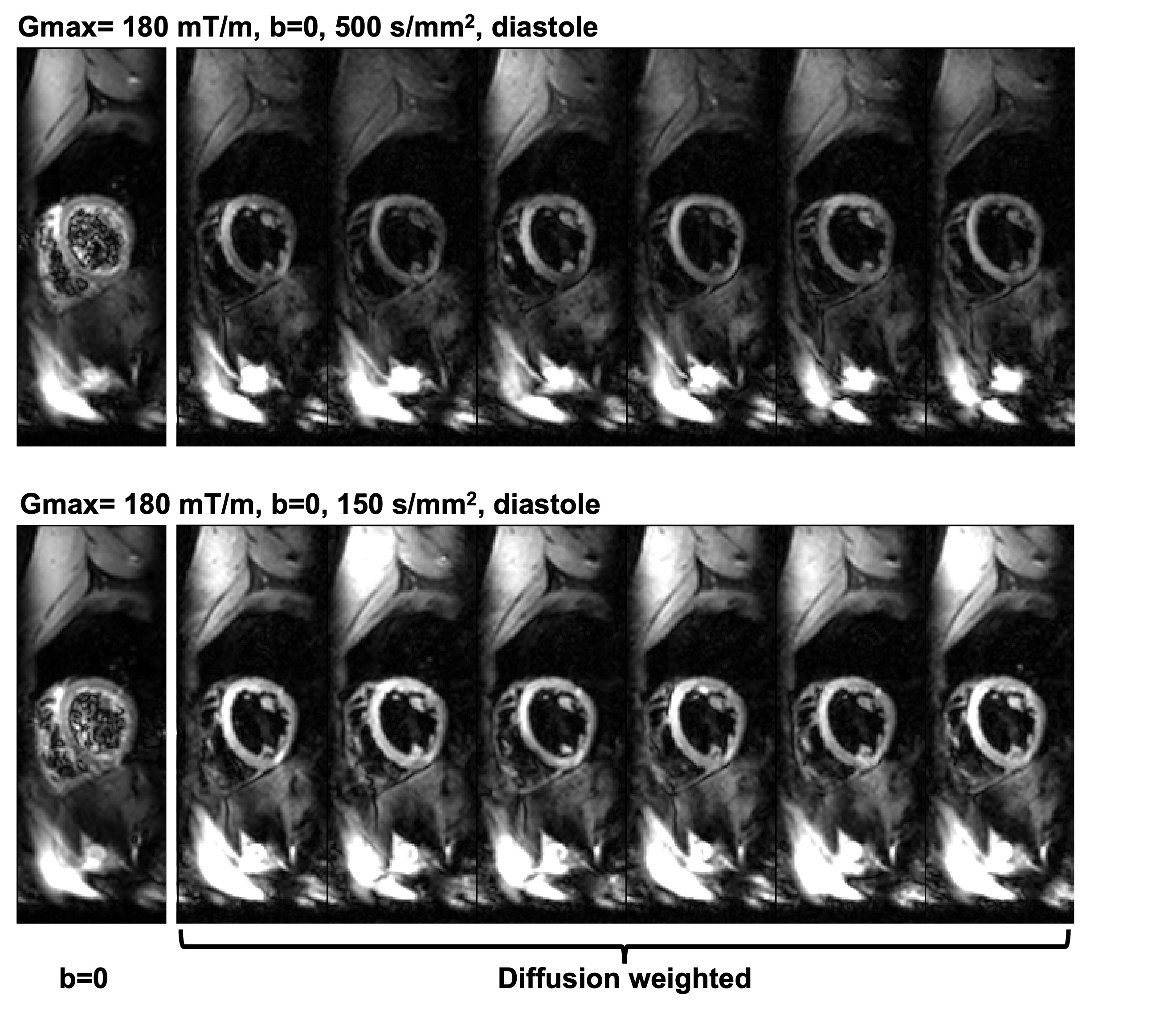
Figure 2: Monopolar SE EPI DT-CMR images for b=0, 150 and 500 s/mm2 for a healthy volunteer during diastolic cardiac phase. The images are windowed separately to highlight the image quality for different b-values.
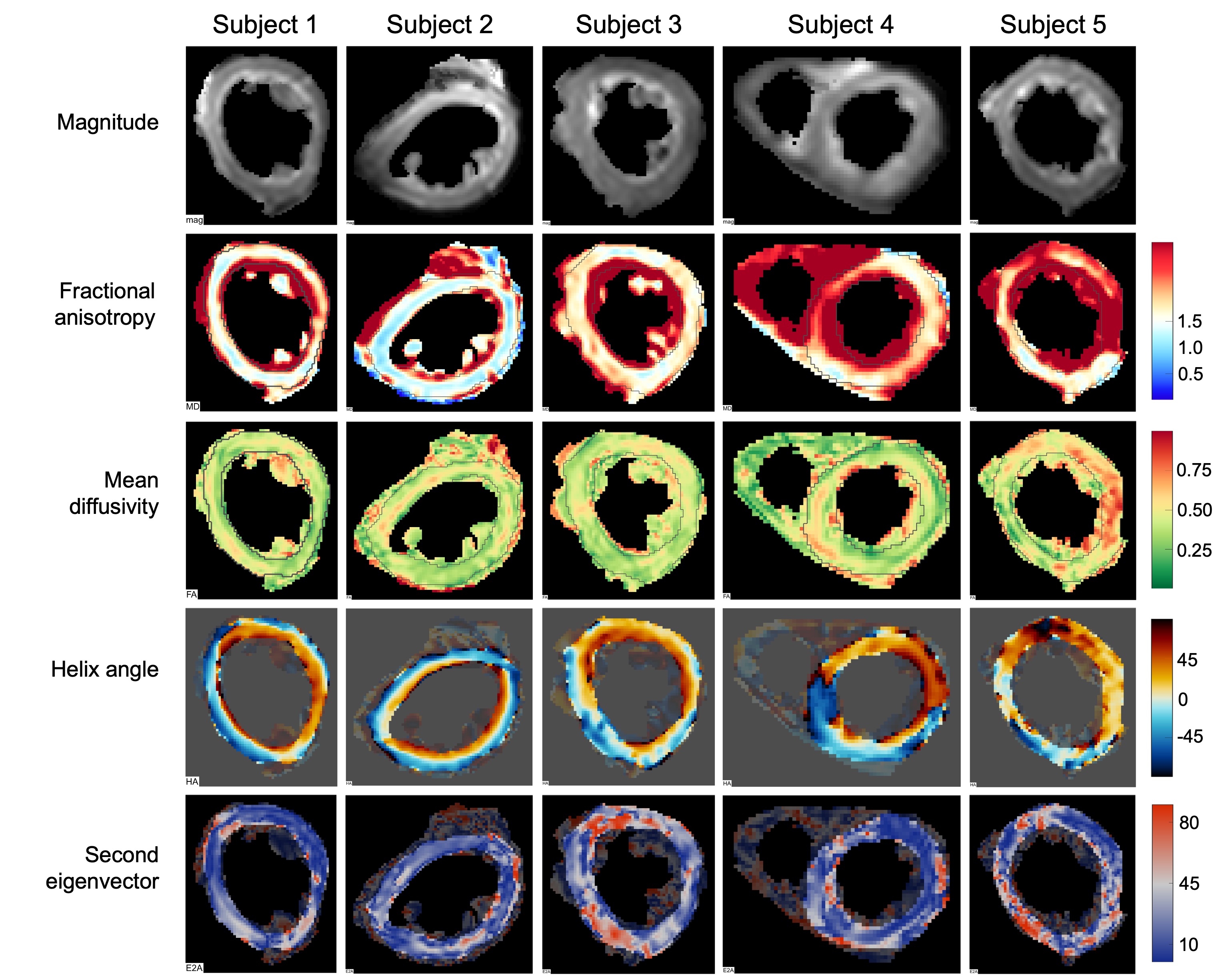
Figure 3: DT-CMR parameter maps calculated for five subjects. Subjects 4 and 5 were discarded because of motion induced signal loss.
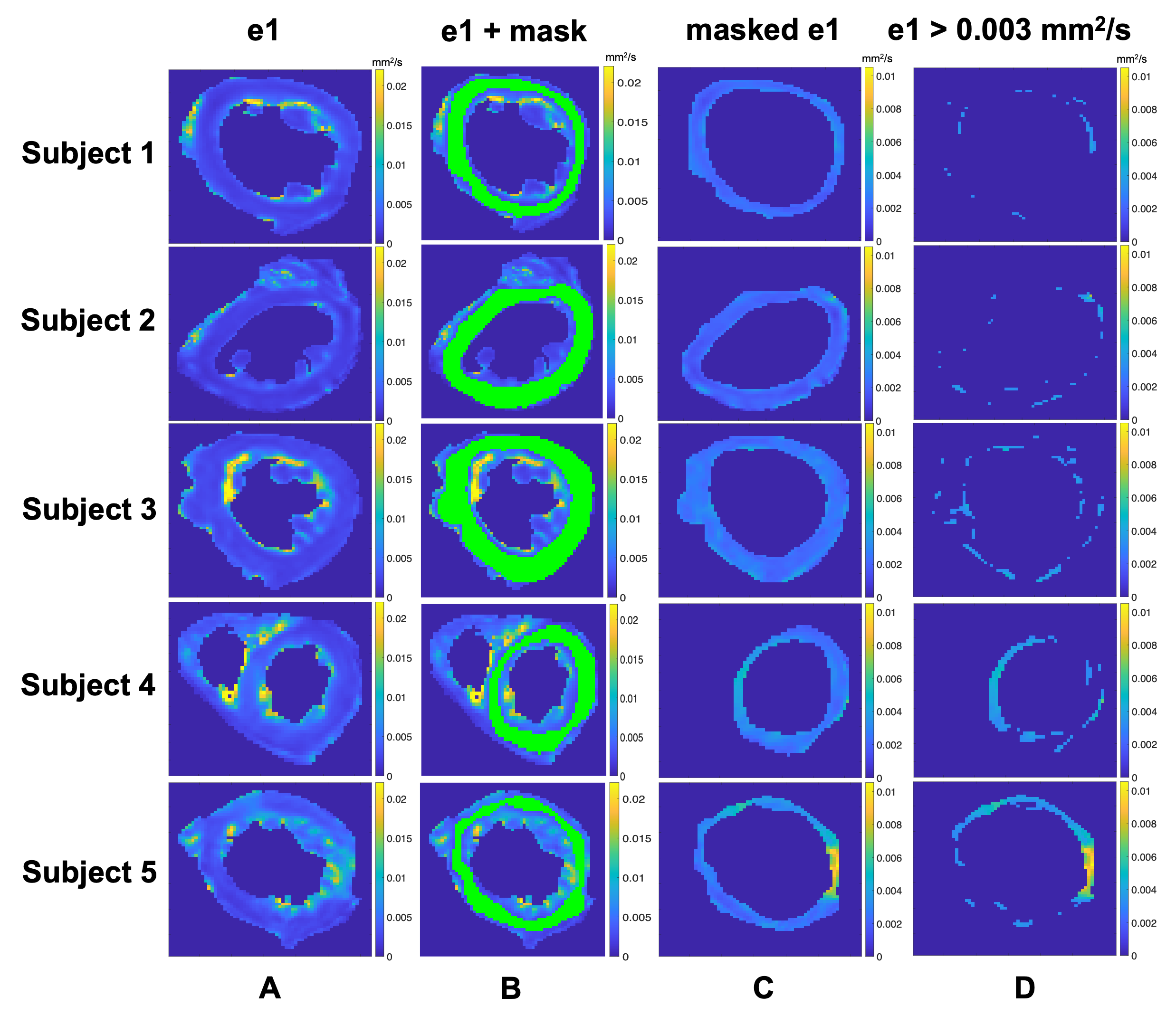
Figure 4: Analysis for the primary eigenvalue (e1) in LV myocardium. Column A represents the primary eigenvalues in LV myocardium. For the analysis of primary eigenvalue exclusively at myocardium a mask was created (Column B). The masked LV with e1 from all pixels is presented at Column C. Column D represents the pixels with e1 higher than diffusivity of free water at 37º C i.e., 3x10-3 mm2/s. Subjects 4 and 5 were discarded because of motion induced phase.
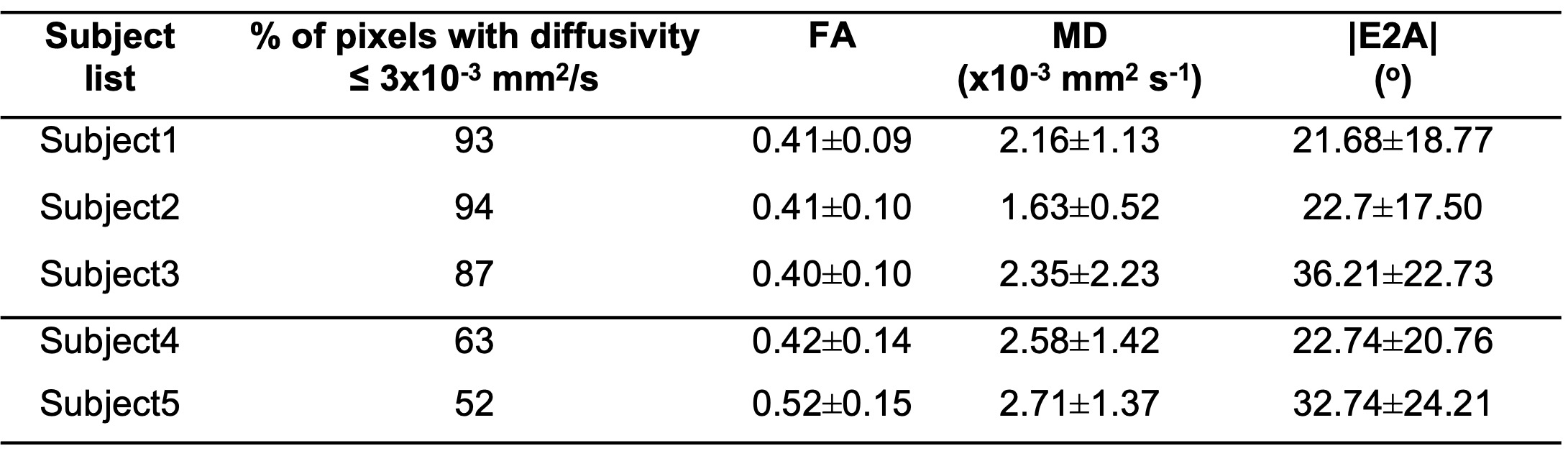
Table 1: Analysis of primary eigenvalue (e1) in LV myocardium for motion indued phase, FA, MD and |E2A| for all subjects.