2427
Achievable Flow-Compensation Parameters on a Clinical 33 mT/m Wide-Bore Scanner for Intravoxel Incoherent Motion Imaging1Medical Radiation Physics, Department of Translational Medicine, Lund University, Malmö, Sweden, 2Radiation Physics, Department of Hematology, Oncology, and Radiation Physics, Skåne University Hospital, Lund, Sweden, 3Department of Medical Radiation Physics, Lund University, Lund, Sweden, 4Department of Neuroimaging, King's College London, London, United Kingdom, 5Radiology, Department of Clinical Sciences, Lund University, Lund, Sweden, 6Oncology, Department of Hematology, Oncology, and Radiation Physics, Skåne University Hospital, Lund, Sweden, 7Systemic Radiation Therapy, Department of Clinical Sciences, Lund University, Lund, Sweden
Synopsis
Keywords: IVIM, Diffusion/other diffusion imaging techniques, Intravoxel incoherent motion, IVIM
Motivation: Can flow-compensated intravoxel incoherent motion be performed on a wide-bore scanner with a 33 mT/m gradient system?
Goal(s): To find the shortest feasible diffusion encoding time for double diffusion encoding waveforms.
Approach: Phantom measurements with various diffusion encoding times, with application of the optimal encoding times on in-vivo brain and prostate scans.
Results: The shortest achievable encoding time was found to be 80 ms, with artefacts being the limiting factor. This encoding time was found to not be sufficiently short for brain imaging. For prostate imaging, it was found to be sufficient for imaging the transitional zone, but not the peripheral zone.
Impact: Due to ghosting artefacts associated with higher gradient amplitudes, we found a diffusion encoding time of 80 ms to be the shortest practically feasible. This encoding time was shown to be insufficient for brain IVIM, and partially so for prostate.
Introduction
Flow-compensated (FC) measurements of intravoxel incoherent motion (IVIM) offers the opportunity to disentangle microvascular diffusion signal from tissue diffusion by compensating for straight flows in the diffusion encoding. For flow-compensation to be a valid measurement of microvasculature, the crucial assumption of ballistic flow has to be fulfilled, i.e. straight blood-flow with no directional changes during the encoding time. Current literature1,2 suggests that this can be achieved at b-values as low as 50 s/mm2 with sufficiently short encoding times. However, very short encoding times with high load on the gradient system may cause other problems. The purpose of this work was to explore the technical and practical limitations of flow-compensated measurements on a wide-bore clinical scanner with a 33 mT/m and 120 T/m/s gradient system.Methods
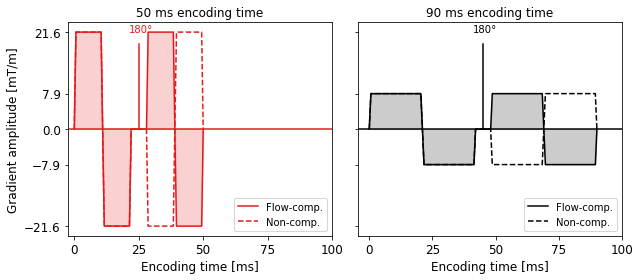
Double diffusion encoded (DDE) MRI was performed on a GE Signa Architect 3T (Milwaukee, WI, USA) with restrictions on max gradient amplitude 33 mT/m and max slew rate 50 T/m/s (per physical amplifier). These restrictions were set to limit mechanical vibrations and PNS-related problems.FC DDE waveforms were produced using the fwf_sequence_tools repository (https://github.com/filip-szczepankiewicz/fwf_sequence_tools) for the GE implementation of the free waveform pulse sequence. Non-compensated (NC) waveforms were created by inverting the encoding after the 180-pulse (Figure 1). Waveforms were generated for a b-value shell of 50 s/mm2, 40 directions for each flow encoding (total 80 waveforms), with waveform sets generated for encoding times 50/60/70/80/90 ms.
A prostate phantom consisting of a kiwi fruit fixated in a water tank was imaged using the aforementioned encoding times with two protocols; brain and prostate. For brain, ASSET was used with complete field-of-view. For prostate, FOCUS was used with field-of-view 12 x 6 cm2. For both protocols, voxel size 1.5 x 1.5 mm2 and slice thickness 3 mm. TE varied with the different DDE waveform encoding times with minimum TE 79 ms for 50 ms encoding time and maximum TE 119 ms for 90 ms encoding time. TR was constant at 2000 ms. Scan time 2 minutes and 44 seconds per waveform set.
Visual analysis was performed on DWI and difference of the averaged images post-registration (FCavg – NCavg) to find the encoding times free of artefacts.
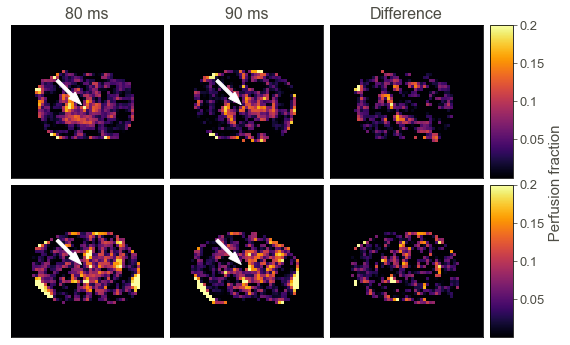
In-vivo imaging was performed on a healthy brain and prostate using the two shortest encoding times. Maps of IVIM perfusion fraction were produced according to3 (FCavg – NCavg)/FCavg.
Results
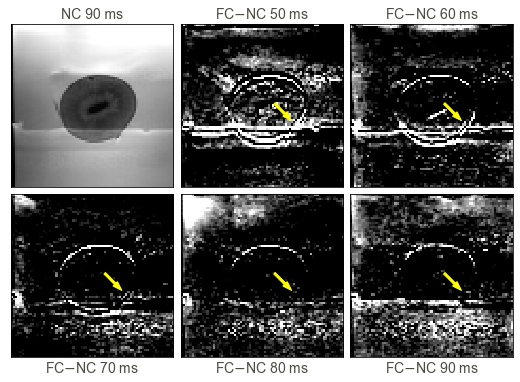
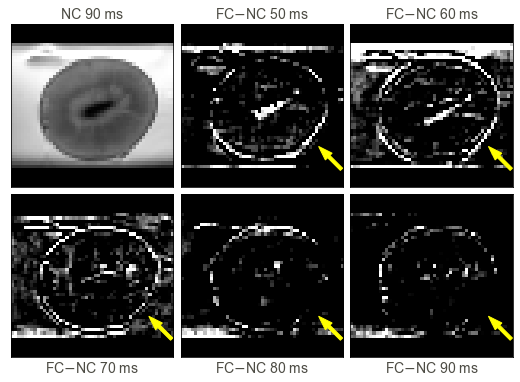
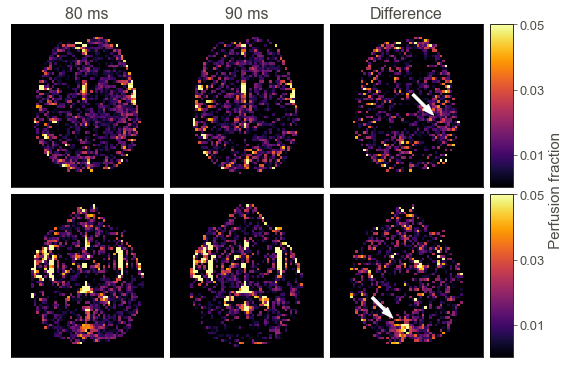
The shortest encoding time free of artefacts was found to be 80 ms for both protocols (Figures 2 and 3). The artefacts can be seen as displacements/ghosting of the phantom in the phase encoding direction, which correlated with strong vibrations during the scans.The brain perfusion maps in Figure 4 are profoundly affected by noise, indicating unsuccessful flow-compensation due to the long encoding time. Apart from CSF, it is difficult to distinguish anatomical features and/or effects related to brain perfusion. The difference map suggests that certain anatomical features may appear with a slightly shorter encoding time.
The perfusion of the prostate shows successful flow-compensation in the transitional zone due to the higher signal values (> 0 in Figure 5), while the peripheral zone does not.
Discussion
As current literature suggests that b-value 50 s/mm2 is sufficient to see a difference between FC and NC signal curves1,2, the use of a single low b-value allowed the investigation of shorter encoding times without exceeding the safety restrictions on gradient amplitude and slew rate.The artefacts seen for the shorter encoding times can be correlated with shakings and vibrations during the scan. Therefore, although even shorter encoding times are technically possible by the system, practical limitations diminish their usefulness. A thorough investigation into the causes of these issues is warranted to further optimize the encoding time. It should also be noted that a visual inspection of each of the 80 DWI showed ghosting artefacts in the phase direction that were reduced with increased encoding time.
The achieved encoding time turned out to be insufficient for brain FC-IVIM estimation of perfusion fraction, where even shorter encoding times are required. Currently published results have used approximately 40 ms1, half of the achieved encoding time in this work.
For the prostate, the consistent positive voxel values of the transitional zone in the perfusion fraction indicate successful compensation of straight flows. This was however not seen in the peripheral zone which may also require shorter encoding times.
Conclusion
Total diffusion encoding times shorter than 80 ms are required for prostate and brain FC-IVIM. Shorter encoding times are technically possible, but presently practically infeasible due to artefacts related to higher gradient amplitudes.Acknowledgements
This work was supported by GE Healthcare.
References
- Ahlgren A, Knutsson L, Wirestam R, Nilsson M, Ståhlberg F, Topgaard D, et al. Quantification of microcirculatory parameters by joint analysis of flow-compensated and non-flow-compensated intravoxel incoherent motion (IVIM) data. NMR in Biomedicine. 2016;29(5):640–9.
- Wetscherek A, Stieltjes B, Laun FB. Flow-compensated intravoxel incoherent motion diffusion imaging. Magnetic Resonance in Medicine. 2015;74(2):410–9.
- Maki JH, Macfall JR, Johnson GA. The use of gradient flow compensation to separate diffusion and microcirculatory flow in MRI. Magnetic Resonance in Medicine. 1991;17(1):95–107.
Figures