2403
Cardiac Magnetic Resonance Imaging in Pediatric Noonan Syndrome: Comparison with Non-syndromic Hypertrophic Cardiomyopathy1Fuwai Hospital, State Key Laboratory of Cardiovascular Disease, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Siemens Healthineers SHS AM NAM USA DI MR COLLAB 737 N. Robertson Blvd., Suite 1600 Los Angeles, CA, 90048 USA, Los Angeles, CA, United States, 3Siemens Shenzhen Magnetic Resonance Ltd. SHS DI MR R&D SZN DL Gao Xin Zhong Er Dao 518057 Shenzhen, China, Shenzhen, China
Synopsis
Keywords: Cardiovascular, Cardiovascular, Noonan syndrome; non-syndromic hypertrophic cardiomyopathy; cardaic MRI; young children
Motivation: The high prevalence of cardiac involvement necessitates comprehensive cardiac exploration at diagnosis and during follow-up in NS, especially when NS was found to be a risk factor in children with HCM
Goal(s): Our study aimed to identify and assess the cardiac MRI features of NS in comparison with non-syndromic HCM in a cohort of young children
Approach: 10 young children genetically confirmed with NS and 10 children genetically confirmed with HCM were evaluated by cardiac MRI
Results: ROC curves documented the diagnostic performance of MRI features(LGE quantification, T1 mapping and strain analysis) in differentiating NS patients from HCM patients
Impact: We performed comprehensive evaluation of pediatric NS by comparison with non-syndromic HCM, and defined a vital role of cardiac MRI in NS. Comprehensive cardiac MRI findings will provide more insights into the rare hereditary cardiomyopathy for researchers and clinicians
Introduction
Noonan syndrome (NS) is a rare hereditary cardiomyopathy with autosomal dominant disorder characterized by distinctive facial dysmorphology, growth failure and a wide spectrum of cardiac abnormalities. Our study aimed to evaluate cardiac magnetic resonance imaging (MRI) features of pediatric NS as well as compare MRI features to cohort of patient with non-syndromic hypertrophic cardiomyopathy (HCM).Methods
From October 2018 to September 2022, 10 young children genetically confirmed with NS were enrolled. For comparison, 10 children genetically confirmed with HCM were also enrolled. All patients were comprehensively evaluated by cardiac MRI including late gadolinium enhancement (LGE), T1 mapping and myocardial strain.Results
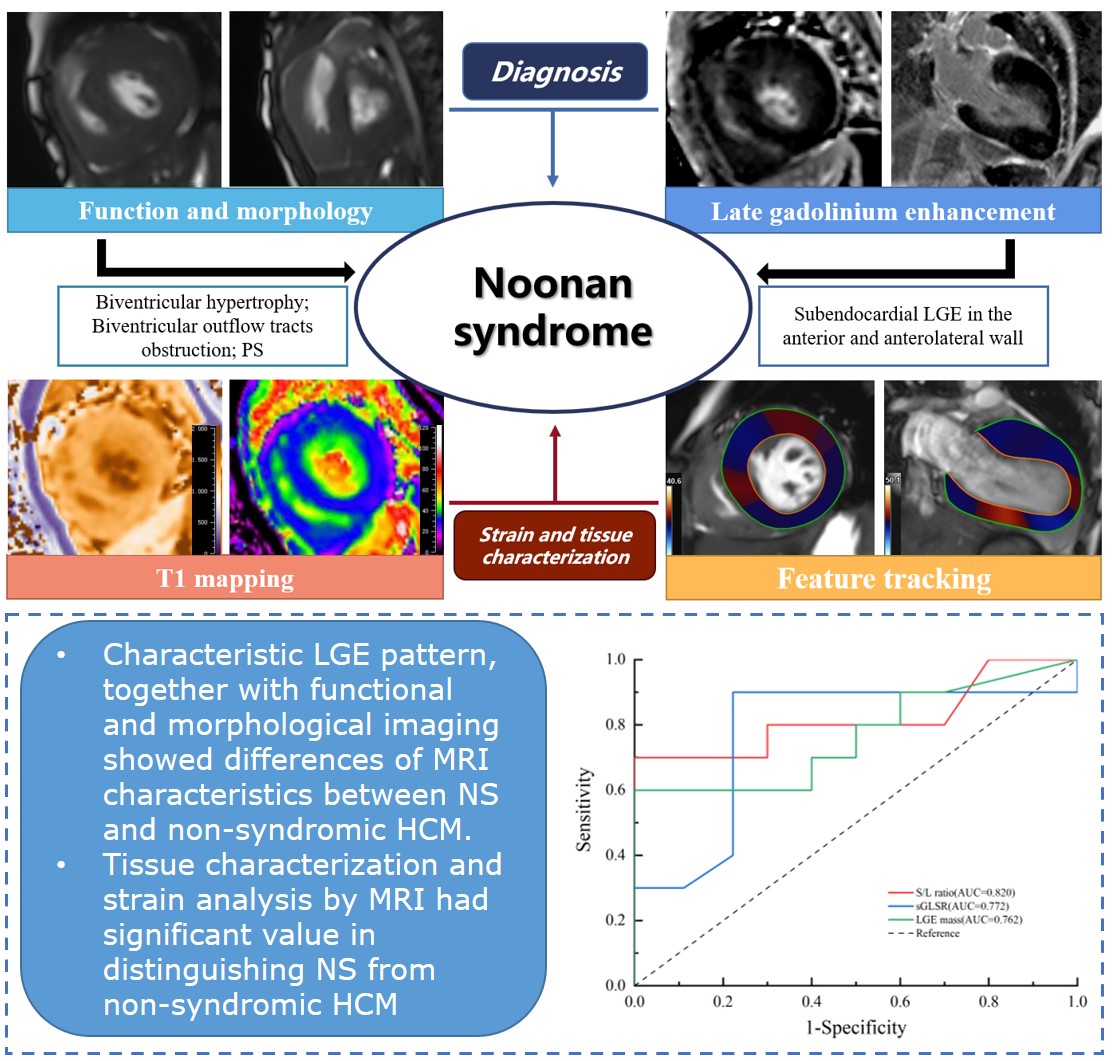
Of the 10 NS children, 7 were females and the median age is 3.1 years (IQR, 0.46-4.30). Pulmonary stenosis was present in 5 NS patients. In comparison with non-syndromic HCM, NS had a higher prevalence of biventricular hypertrophy and biventricular outflow tracts obstruction, while asymmetric hypertrophy was more prevalent in non-syndromic HCM. Characteristic LGE pattern of subendocardial LGE in the anterior and anterolateral wall was detected in NS. NS patients had lower extent of LGE (LGE mass:10.62g vs 2.06g, P=0.043; LGE percentage:11.49% vs 6.13%, P=0.052) and extracellular volume (ECV) (29.3% vs 37.1%, P=0.065) than non-syndromic HCM. Significant lower global systolic global longitudinal strain rate (sGLSR) was also found in NS (P<0.05). Using ROC analysis, age, ratio of LV septum to lateral wall thickness, LGE mass, LGE percentage, ECV and sGLSR were good discriminators for NS patients and HCM patients (all P<0.05). The LGE mass cutoff value was 0.57 for distinguishing NS from non-syndromic HCM (AUC: 0.765; sensitivity: 90.00%, specificity: 80.00%), and the ECV cutoff value was 35.4 (AUC: 0.761; sensitivity: 88.89%, specificity: 60.00%). An sGLSR cutoff value of -0.67 had a sensitivity of 77.78%, a specificity of 90.00%, and an AUC of 0.772.Discussion
To our knowledge, the current study was the first to conduct systematic cardiac MRI evaluation of pediatric NS including T1 mapping and feature-tracking strain analysis. In the guideline, biventricular hypertrophy and biventricular outflow tracts obstruction suggested specific etiologies of HCM, such as NS. In our study, compared with non-syndromic HCM, RVH and RVOT were more frequent in NS. In addition, compared with the non-syndromic HCM patients in our study, lower extent of LGE and ECV and lower strain values were documented in NS. Heterogeneous mutations in the Ras/MAPK signaling pathway have been found to account for the cardiac developmental disorders in NS, while the definite pathophysiology of myocardial tissue characterization and myocardial deformation is unclear and needs to be further investigated.Conclusion
Characteristic LGE pattern, together with functional and morphological imaging showed differences of MRI characteristics between NS and non-syndromic HCM. And tissue characterization (LGE quantification and T1 mapping) and strain analysis had significant value in distinguishing NS from non-syndromic HCM.Acknowledgements
NAReferences
1. Mendez HM, Opitz JM. Noonan syndrome: a review. Am J Med Genet. 1985;21:493-506.
2. Romano AA, Allanson JE, Dahlgren J et al. Noonan syndrome: clinical features, diagnosis, and management guidelines. Pediatrics. 2010;126:746-759.
3. Alexander PMA, Nugent AW, Daubeney PEF et al. Long-Term Outcomes of Hypertrophic Cardiomyopathy Diagnosed During Childhood: Results From a National Population-Based Study. Circulation. 2018;138:29-36.
Figures