2401
Diagnostic Value of Pulmonary MR Ultra-Short Echo Time (UTE) Imaging in Potential Pulmonary Metastasis in Pediatric Hepatoblastoma1Radiology, Renji Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, China, 2MR Scientific Marketing, Siemens Healthineers Co Ltd, Shanghai, China, Shanghai, China, 3Liver Surgery, Renji Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, China
Synopsis
Keywords: Cancer, Tumor, Hepatoblastoma; Metastasis; UTE
Motivation: UTE MR has demonstrated its potential for evaluating pulmonary lesions, which could be employed for assessing pulmonary metastasis from hepatoblastoma.
Goal(s): To investigate the diagnostic performance of UTE MR for detecting pulmonary nodules and thus diagnosing pulmonary metastasis in pediatric hepatoblastoma patients.
Approach: Lung UTE was assessed for its capability to detect nodules and for its diagnostic performance for pulmonary metastasis.
Results: UTE has a moderate diagnostic sensitivity for metastasis, while its specificity is high. When it comes to single pulmonary nodules, UTE has a moderate detection rate with a relatively high false positive detection rate.
Impact: UTE has a moderate diagnostic sensitivity for pulmonary metastasis, while its specificity is high. To make MR imaging a reliable one-stop assessment tool, higher resolution UTE imaging technology will be needed in the future.
Introduction
Hepatoblastoma is the most common malignant liver tumor in children, often presenting with pulmonary metastasis. Accurate preoperative assessment and postoperative surveillance of pulmonary lesions are crucial for optimal management and treatment planning(1,2). Traditionally, CT has been the modality of choice for diagnosing pulmonary metastasis due to its high spatial resolution. Recent advances have enabled ultrashort echo time (UTE) sequence detection of signals from tissues with ultrashort relaxation times, which may be useful for diagnosing metastatic lung diseases(3–5).Our aim is to assess UTE MR's diagnostic performance in pediatric hepatoblastoma patients undergoing preoperative assessment or postoperative surveillance for detecting pulmonary nodules and diagnosing pulmonary metastasis, using routine chest CT as the reference standard.
.
Methods
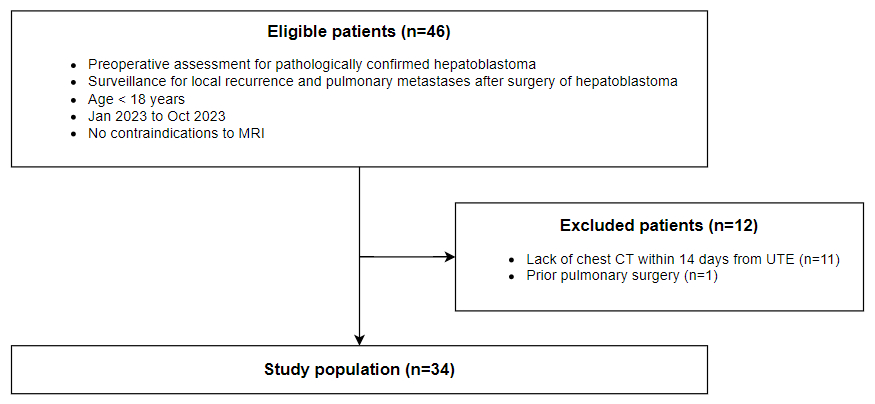
This study was approved by the institutional review board. Informed consent was obtained from the patients’ guardians. Inclusion and exclusion criteria were illustrated in Fig 1.Sedation was performed by the anesthesiology team following the institutional protocol. MRI was performed on a 3T scanner (MAGNETOM Skyra,Siemens Healthcare, Erlangen, Germany). A lung UTE (working in process #992, slice thickness of 1.25mm. Specific parameters: TR=4.23ms, TE=0.05 ms, FA=5°, FOV=319mm, acquisition matrix=2.5, spatial resolution=1.25×1.25×1.25 mm3, scan direction=coronal, respiratory gating=free breathing, base resolution=256, Spiral interleaves=504, slice resolution=50%, trajectory=spiral) was performed following the routine 20-minute free-breathing contrast-enhanced liver MR imaging(6). 0.1 mmol of gadopentetate gadobutrol (Gadovist, Bayer Schering Pharma AG., Leverkusen, Germany) per kilogram of body weight with a maximum dose not exceeding 7.5 mmol was administered manually followed by a saline flush for liver MR imaging. At the time of the UTE, no additional contrast was administrated.
Image review sessions were divided into lesion level and patient level assessments. During the lesion level assessment session, two radiologists (R1, R2) identified and labeled up to five nodules at UTE without knowing their clinical details. A second team of radiologists (R3, R4) determined whether these lesions were nodules on CT, and if so, recorded their diameter. A maximum of five additional non-calcified solid nodules were selected on CT by R3 and R4 if additional nodules were detected on UTE. R1, R2 judged whether the lesions were readily visible as nodules on UTE, and recorded their diameters. R3 and R4 were instructed to select lesions of different diameters whenever possible. A pulmonary nodule is defined as an approximately rounded opacity on CT or a well-defined area of high signal intensity on UTE measuring up to 3 cm in diameter(7). Consequently, each case with up to ten lesions detected by UTE and/or CT will be observed.
In patient level assessment session, both groups of radiologists decide on whether lung metastasis can be diagnosed at CT and UTE, respectively. A solid non-calcified pulmonary nodule >= 5 mm or greater than two non-calcified nodules >= 3 mm is considered metastatic by the 2017 PRE/POSTTEXT system(8).
A paired samples t-test was used to compare the diameters of nodules detected by CT and UTE. A t-test was used to compare the diameters of UTE detectable and undetectable nodules. In addition, the nodule detection rate as well as the false positive detection rate (the number of false-positives divided by the total number of UTE detections) were calculated(9). The performance of UTE in diagnosing patient-level metastasis was evaluated.
Results
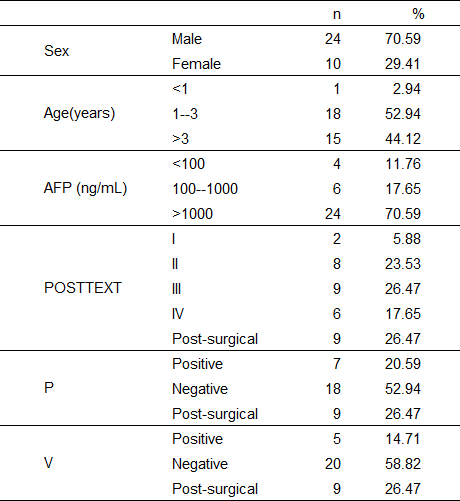
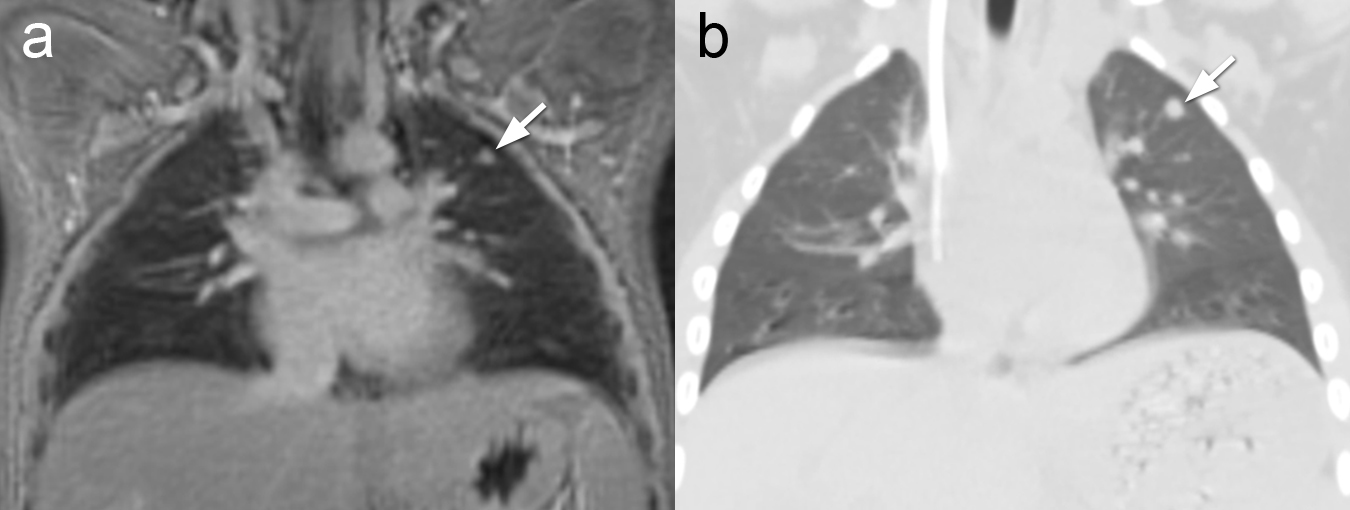
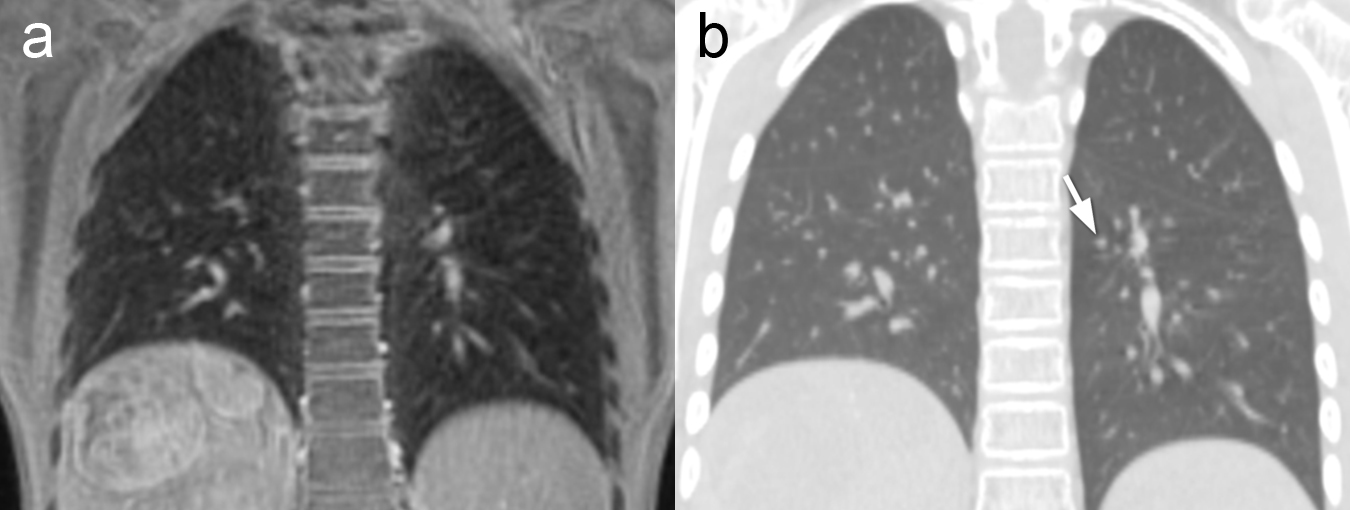
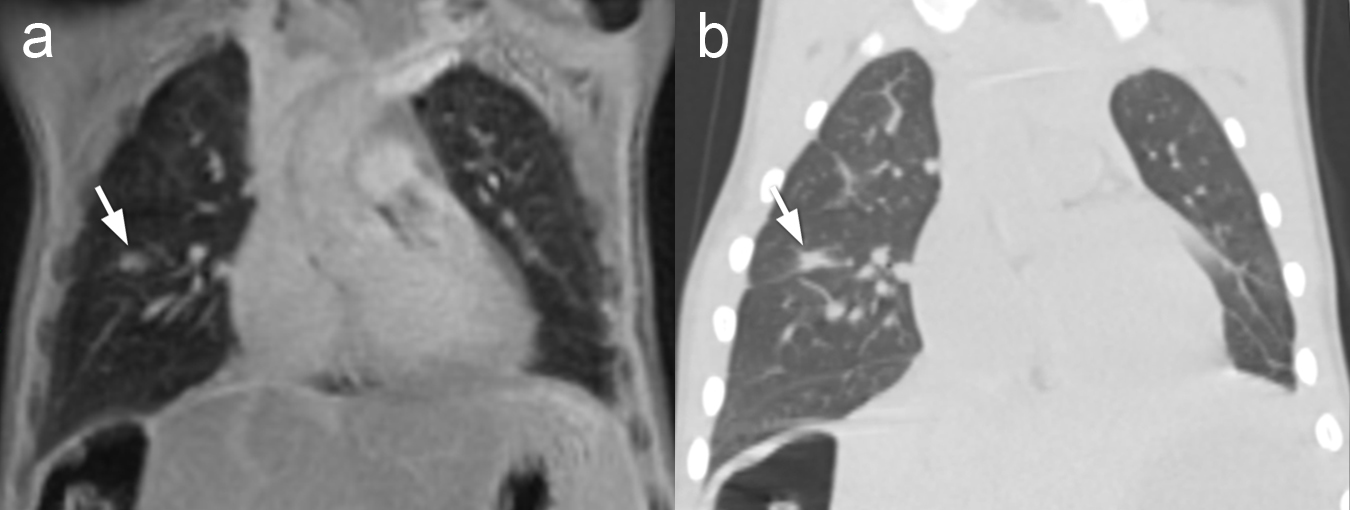
There were 34 patients enrolled in the study. Fig. 2 shows the patient demographics.There were a total of 30 UTE or CT-detected lesions, including 18 nodules on both (Fig 3). There was no statistically significant difference in diameter between UTE (7.98 ± 4.26 mm) and CT (8.03 ± 3.48 mm) measurements (paired samples t-test, P = 0.884). Seven nodules were not detected by UTE (Fig 4). The diameter of the UTE detectable nodules (8.03 ± 3.48 mm) and undetectable nodules (3.74±1.09 mm) significantly differed. On UTE, five lesions were mistaken for nodules (Fig 5). The detection rate and false positive detection rate for UTE were 72.0% and 21.7%, respectively.
Five patients had lung metastasis on CT, but three met the criteria for metastasis on UTE. UTE diagnosis of metastasis had two false-positives and two false-negatives. The sensitivity and specificity for UTE were 60.0% and 93.1%, respectively.
Conclusion
UTE has moderate sensitivity and high specificity for pulmonary metastasis. UTE has a moderate detection rate with a relatively high false positive rate for single pulmonary nodules. Nodule detection on UTE is affected by their diameter.Acknowledgements
No acknowledgement found.References
- Fuchs J, Cavdar S, Blumenstock G, Ebinger M, Schäfer JF, Sipos B, et al. POST-TEXT III and IV Hepatoblastoma: Extended Hepatic Resection Avoids Liver Transplantation in Selected Cases. Annals of Surgery. 2017 Aug;266(2):318–23.
- King SJ, Babyn PS, Greenberg ML, Phillips MJ, Filler RM. Value of CT in determining the resectability of hepatoblastoma before and after chemotherapy. American Journal of Roentgenology. 1993 Apr;160(4):793–8.
- Hirsch W, Sorge I, Krohmer S, Weber D, Meier K, Till H. MRI of the lungs in children. European Journal of Radiology. 2008 Nov;68(2):278–88.
- Cha MJ, Park HJ, Paek MY, Stemmer A, Lee ES, Park SB, et al. Free-breathing ultrashort echo time lung magnetic resonance imaging using stack-of-spirals acquisition: A feasibility study in oncology patients. Magnetic Resonance Imaging. 2018 Sep;51:137–43.
- Renz DM, Herrmann KH, Kraemer M, Boettcher J, Waginger M, Krueger PC, et al. Ultrashort echo time MRI of the lung in children and adolescents: comparison with non-enhanced computed tomography and standard post-contrast T1w MRI sequences. Eur Radiol. 2022 Mar;32(3):1833–42.
- Gong XH, Feng MX, Zhuang ZG, Yan YQ, Wang L, Ren HN, et al. Pediatric Hepatoblastoma After Neoadjuvant Chemotherapy: Diagnostic Performance of MR in Staging POSTTEXT and Vascular Involvement. Magnetic Resonance Imaging. 2023 Jun 5;jmri.28848.
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology. 2008 Mar;246(3):697–722.
- Towbin AJ, Meyers RL, Woodley H, Miyazaki O, Weldon CB, Morland B, et al. 2017 PRETEXT: radiologic staging system for primary hepatic malignancies of childhood revised for the Paediatric Hepatic International Tumour Trial (PHITT). Pediatr Radiol. 2018 Apr;48(4):536–54.
- Liu K, Li Q, Ma J, Zhou Z, Sun M, Deng Y, et al. Evaluating a Fully Automated Pulmonary Nodule Detection Approach and Its Impact on Radiologist Performance. Radiology: Artificial Intelligence. 2019 May;1(3):e180084.
Figures