2400
UTE Imaging for Rapid Whole-Body Central Vascular Access Assessment in Children and Young Adults Undergoing Cardiac Surgery1Cardiology, Pediatrics, Children's Medical Center Dallas, Dallas, TX, United States, 2Cardiology, Pediatrics, UT Southwesten Medical Center, Dallas, TX, United States
Synopsis
Keywords: Visualization, Cardiovascular, UTE, Access, Vasculature, Quality, CHD, Contrast, Chest, Abdomen, Diagnostic
Motivation: The motivation for this study is to propose an alternative and more efficient imaging protocol for vascular access assessment for complex congenital heart disease (CHD) cases
Goal(s): To determine if UTE imaging can provide a supplemental tool to conventional MR imaging for evaluating vascular access in the context of CHD.
Approach: Selection of 15 patients undergoing pre-operative assessment for complex CHD, including ferumoxytol administration, implement a 3D UTE sequence and a quality scoring scale.
Results: The study concludes that UTE imaging is a time-efficient method to visualize vascular anomalies, patency, occlusion, and access, and it can complement MRI planning for cardiovascular procedures.
Impact: Our study demonstrates that UTE imaging with ferumoxytol can provide high-quality vascular access imaging for patients with complex CHD. This offers an improved diagnostic tool for assessing vascular access as an important addition to the tools available for CHD evaluation.
Introduction
With the increasing use of blood pool contrast agents for complex congenital heart disease, the ability to perform first-pass angiography is limited. High quality 3D whole heart bSSFP-based sequences are time consuming and lack adequate field homogeneity to allow large volume vascular access imaging. Conversely, as patients require more careful operative planning, including transplantation and mechanical ventricular support, the requirement for vascular access planning is paramount. We propose a rapid free-breathing and ungated vascular access imaging protocol for all patients undergoing complex pre-operative congenital heart disease (CHD) MRI using the Ultrashort Echo Time (UTE) sequence. In this study we assess the image quality and diagnostic performance of UTE imaging for central vascular access assessment.Methods
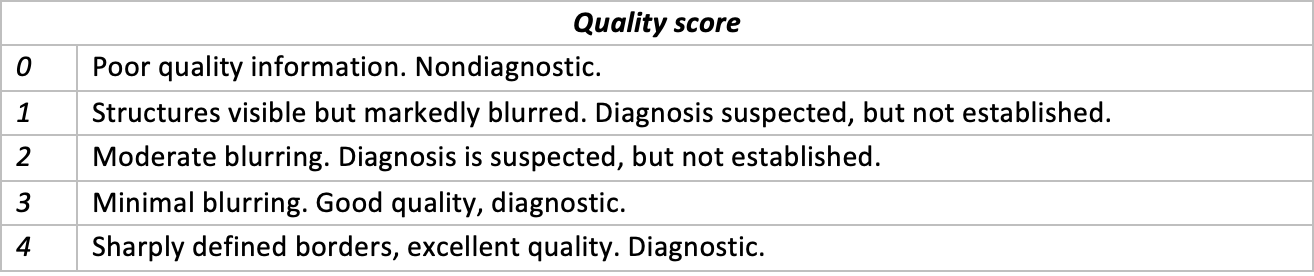
Fifteen patients undergoing pre-operative assessment for complex CHD with cardiac MRI that included ferumoxytol administration were included in the study. The patients’ age, gender, body surface area, and diagnosis were recorded (Table 1). Prospective informed consent was obtained with IRB approval(STU032016-009 ). The study was performed using a Phillips Ingenia 1.5 T system (PhilipsHealthcare, Best, Netherlands) and a 32 channel Flex coil with 60 cm coverage.The 3D UTE sequence was implemented using center-out spiral readouts. The sequence was run in a free-breathing and ungated fashion without using any prepulse. For the chest region, parameters of the sequence include: TE/TR = 0.1/5.1, flip angle = 18, isotropic acquired resolution 1.74 mm3, isotropic reconstructed resolution 1.34 mm3, Field of View=300x300x300 mm^3. The acquisition time was 54 seconds. The Abdomen and Pelvis was done as a separate acquisition with the same sequence parameters. Qualitative imaging quality was assessed by a five-point scoring scale (Table 2). Assessment of central vessels focused on vascular patency and anatomy definition. In addition to image quality, the ability to define all central vessels with diagnostic certainty was recorded by two independent observers, each with over 5 years’ experience.
Results
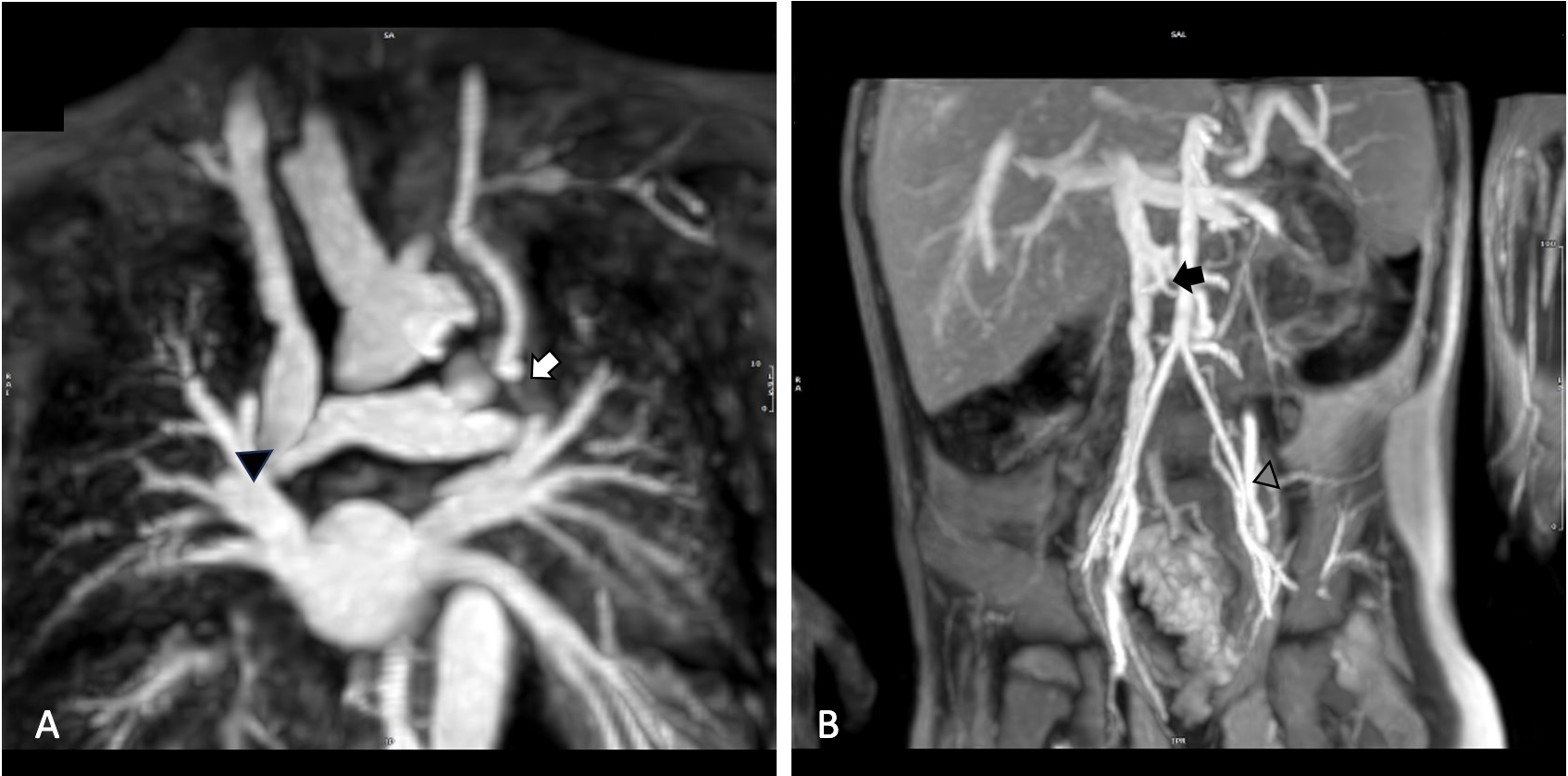
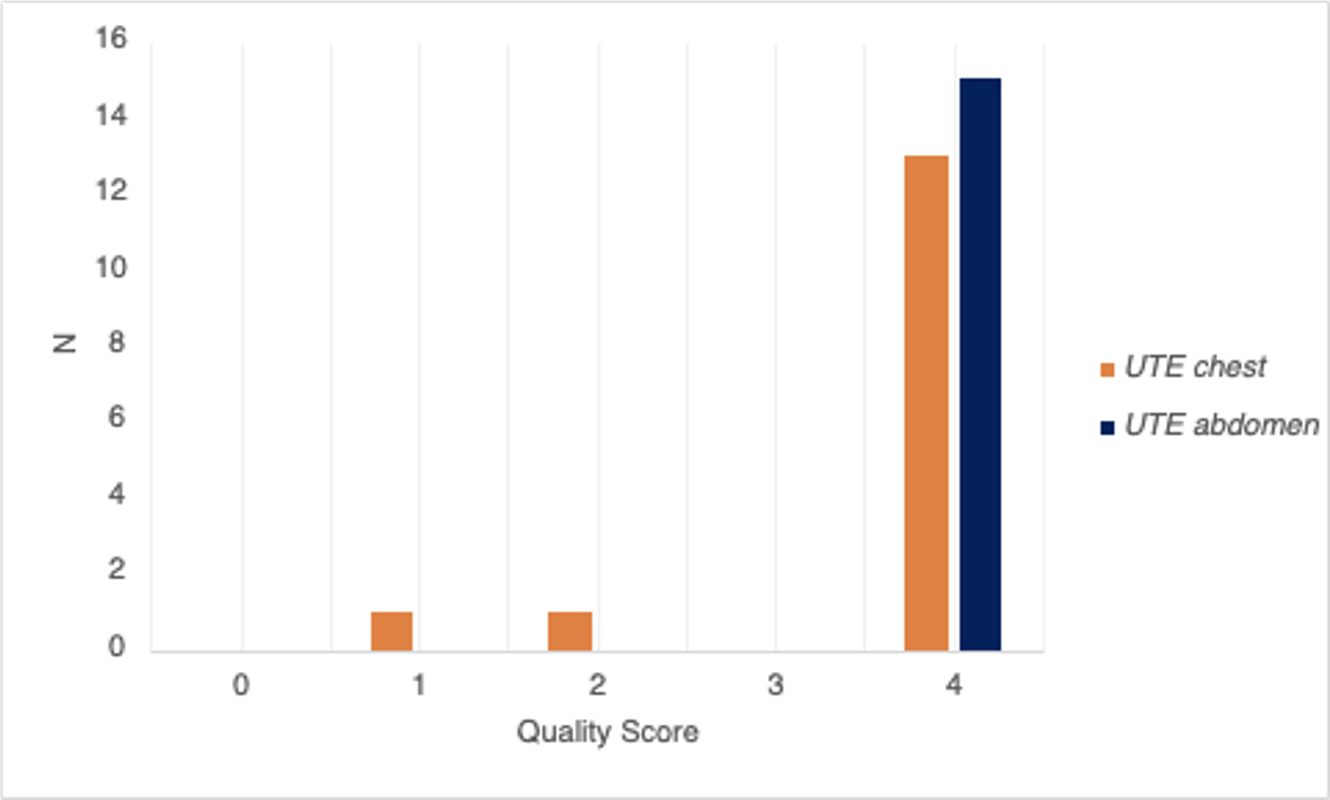
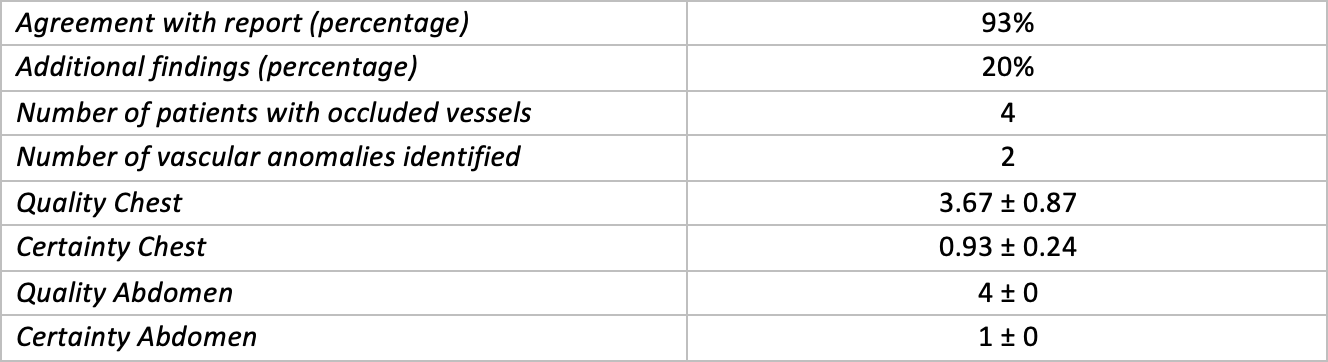
The UTE imaging with ferumoxytol contrast provided high quality images with diagnostic certainty index scoring in both the chest and the abdomen (Figure 2). Additional diagnostic findings were determined in 20% of cases. Four cases were identified with obstructed vasculature, and three patients had structural vascular anomalies, including right aortic arch and bilateral superior vena cava. Susceptibility artifacts were considerably reduced in comparison to bSSFP imaging but for two of the cases, the susceptibility artefact on chest imaging due to stainless steel vascular embolization coils precluded full diagnostic evaluation . Otherwise, vascular access in both chest and abdomen were clearly discernible in all other chest and abdominal sequences. Assessment of vessel patency and complete diagnosis was identical to those reported by previous diagnostic studies and showed a good argument for improved diagnostic analysis on additional findings (Table 3).Discussion
Our study showed that UTE MR imaging produced vascular imaging with high quality and diagnostic certainty indexing and relatively few susceptibility, motion, and flow artifacts. The demographic characteristics of each case were not correlated to imaging quality, though diagnostic and procedural status correlated with significant coil artifacts consequent to device placement at the level of the chest. Structural anomalies, such as bilateral superior vena cavae and right-sided aortic arch, and vascular occlusions could be assessed with high diagnostic certainty. The use of UTE as outlined in this study is a highly time-efficient method in which to optimize the visualization of vascular anomalies, patency, occlusion, and access as an adjunct to MRI planning for cardiovascular procedures.Conclusion
The use of vascular UTE imaging may provide a good supplemental tool to conventional MR imaging in the assessment of vascular access.Acknowledgements
No acknowledgement found.References
Hoerr, V., Nagelmann, N., Nauerth, A. et al. Cardiac-respiratory self-gated cine ultra-short echo time (UTE) cardiovascular magnetic resonance for assessment of functional cardiac parameters at high magnetic fields. J Cardiovasc Magn Reson 15, 59 (2013). https://doi.org/10.1186/1532-429X-15-59
Schuijf JD, Ambale-Venkatesh B, Kassai Y, Kato Y, Kasuboski L, Ota H, Caruthers SD, Lima JA. Cardiovascular ultrashort echo time to map fibrosis-promises and challenges. Br J Radiol. 2019 Nov;92(1103):20190465. doi: 10.1259/bjr.20190465. Epub 2019 Aug 8. PMID: 31356106; PMCID: PMC6849674.
Figures