2399
Differentiating Low- and High-Grade Pediatric Brain Tumor Using Integrated DWI1Center for Magnetic Resonance Research, University of Illinois Chicago, Chicago, IL, United States, 2Medical Scientist Training Program, University of Illinois Chicago, Chicago, IL, United States, 3Department of Biomedical Engineering, University of Illinois Chicago, Chicago, IL, United States, 4Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 5Department of Radiology, Xin Hua Hospital, Shanghai, China, 6Department of Radiology and Neurosurgery, University of Illinois Chicago, Chicago, IL, United States
Synopsis
Keywords: Cancer, Brain, pediatric brain tumor
Motivation: Pediatric brain tumors is the most common cancer among the pediatric population, and DWI-imaging offers a non-invasive method to assess tumor grade to guide appropriate treatments.
Goal(s): The study investigates the feasibility of DISMANTLE, an integrated DWI approach for simultaneous assessment of tissue cellularity, vascularity, and heterogeneity, in differentiating high-grade and low-grade pediatric brain tumors.
Approach: Seventy pediatric patients with brain tumors, categorized into high-grade and low-grade, were scanned with DWI sequence. Images were analyzed using DISMANTLE and 3 comparison models.
Results: Removing the perfusion-related signal in DISMANTLE improved the accuracy and sensitivity of diffusion-related parameters in assessing pediatric brain tumor grades.
Impact: The study emphasizes the importance of appropriate signal characterization and fitting strategies for high b-value DWI in robust assessment of brain tumors. Future DWI modeling should consider segmentally fitting the diffusion and perfusion-related signals.
Introduction
Pediatric brain tumors are the most common cancer in children under 15 years of age, accounting for more than 20% of all neoplasms1. Accurate assessment of pediatric brain tumor grade is imperative for treatment decisions. Diffusion-weighted imaging (DWI) with conventional apparent diffusion coefficient (ADC) has emerged as a tool for brain tumor grading because of its sensitivity to tissue cellularity2. While ADC is informative3, it lacks the flexibility to characterize complex diffusion processes as it relies on the assumption of Gaussian diffusion. Consequently, several advanced DWI models, such as intravoxel incoherent motion (IVIM) model4 and continuous-time random-walk (CTRW) model5 have been developed to probe additional tissue structural properties beyond cellularity. Here we employ an integrated DWI approach for simultaneous assessment of tissue cellularity, vascularity, and heterogeneity (DISMANTLE) that is based on the combination of the IVIM and CTRW models6. Built upon previous success of using DISMANTLE for breast cancer diagnosis and treatment monitoring6, the present study aims at assessing the performance of DISMANTLE in differentiating between low-grade and high-grade pediatric brain tumors.Methods
Patients: The patient group consisted of 70 children (4 months to 13 years old; 20 females) who underwent surgical biopsy or surgery with histopathology confirmation under an IRB-approved protocol. Thirty patients were classified as low-grade grades (I or II) and 40 as high-grade (grades III or IV) tumors.MR Imaging: All patients underwent MR examination on a 3T GE Signa scanner with an 8-channel head coil. The imaging protocol included FLAIR, T2, pre-/post-contrast T1, and multi-b-value DWI series. DWI was performed with single-shot spin-echo EPI using 12 b-values (0-4000sec/mm2).
DWI Analysis: Diffusion-weighted images were analyzed by four DWI models: 1) IVIM, 2) CTRW, 3) DISMANTLE, and 4) mono-exponential models. DWI signal were characterized as follows:
$$ S/S_0 = fe^{-bD_{perf}} + (1-f)e^{-bD_{diff}} \tag 1 $$
$$ S/S_0 = E_\alpha(-(bD_m))^{\beta} \tag 2 $$
$$ S/S_0 = fe^{-bD_{perf}} + (1-f)E_{\alpha^*}(-(b{D^{}_{m}}^*))^{\beta^*} \tag 3$$
$$ S/S_0 = e^{-b(ADC)} \tag 4$$
IVIM parameters in Eq. (1), Ddiff, Dperf, and f, represent diffusion coefficient, pseudo-diffusion coefficient, and perfusion fraction, respectively. In Eq. (2), E⍺ is a Mittag-Leffler function5 while Dm is CTRW model’s diffusion coefficient. ⍺ and β represent temporal and spatial diffusion heterogeneities. In Eq. (3), DISMANTLE provides two parameters identical to IVIM (f, Dperf) and three parameters analogous to CTRW (Dm*, ⍺*, and β*). DISMANTLE was implemented through a multi-step approach as illustrated in Fig. 1.
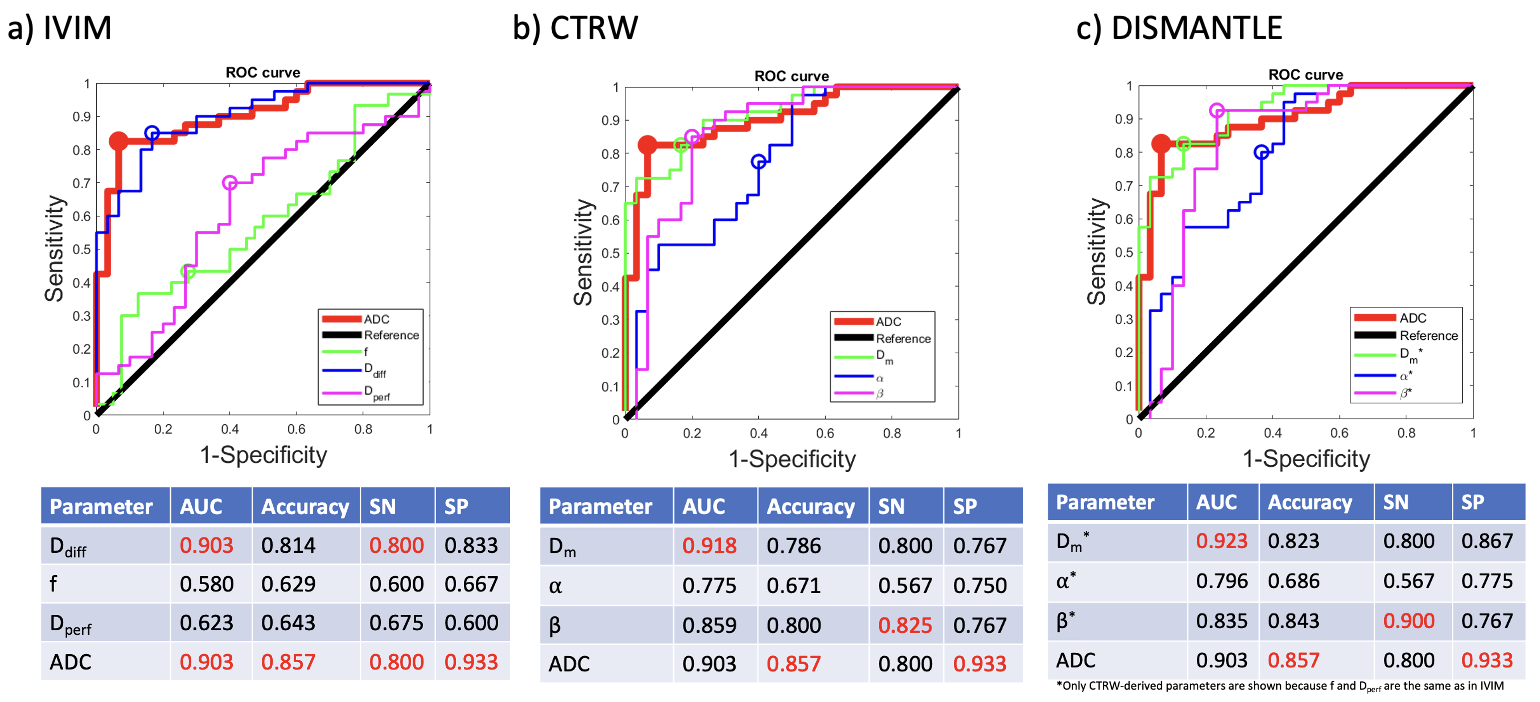
Statistical Analysis: Mean values for all parameters were calculated over tumor regions of interest. Mann-Whitney U-test was conducted between low-grade and high-grade tumors for each parameter (threshold: p < 0.05). Receiver operating characteristic (ROC) analysis was performed using each parameter for differentiation between low-grade and high-grade tumors. Performance of models was assessed by AUC, sensitivity, specificity, and accuracy using a leave-one-out approach with logistic regression.
Results
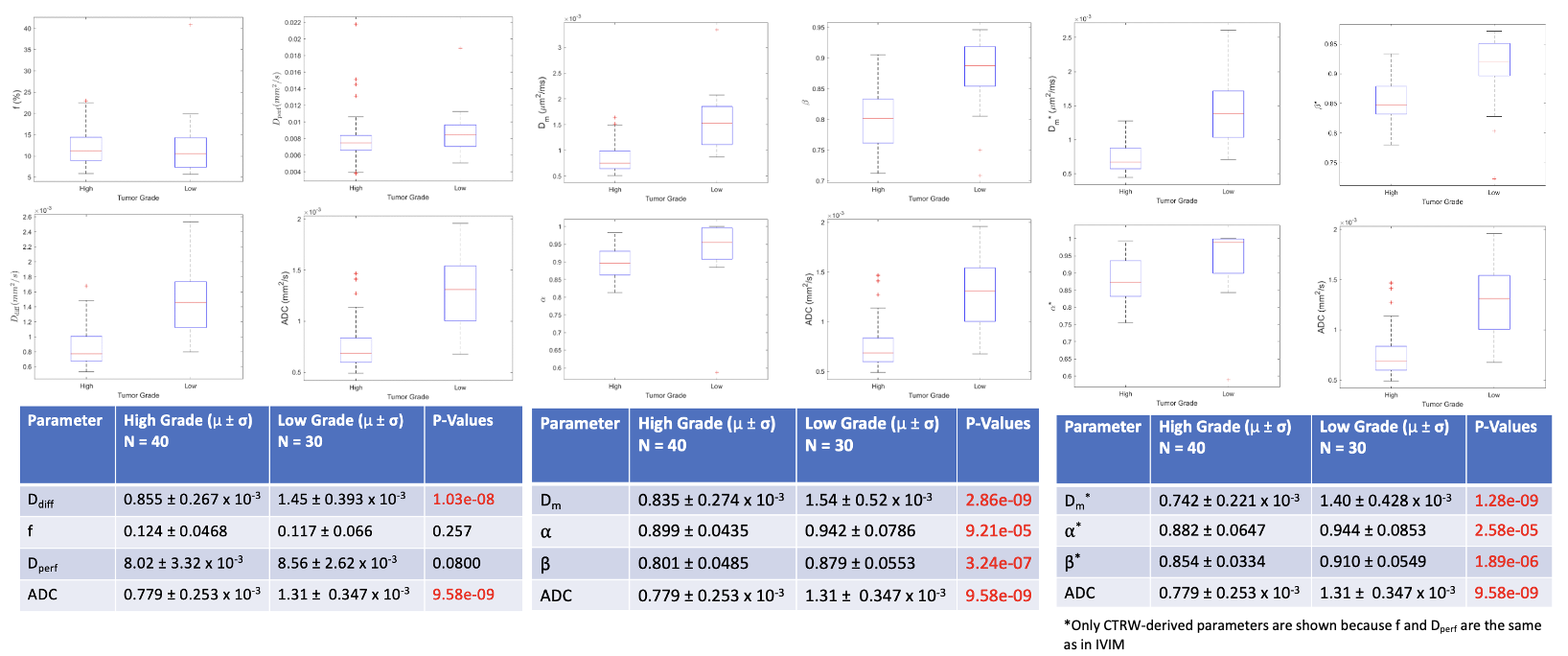
Figure 2 shows representative parameter maps from one representative patient in each group. ADC, Dm, Dm*, Ddiff , ⍺, ⍺*, β, and β* values are appreciably lower in high-grade tumors. These observations were substantiated in the group analysis. As summarized in Figure 3, all parameters except the perfusion-related f and Dperf yielded statistically significantly lower mean values in the high-grade tumors. As shown in Figure 4, the DISMANTLE CTRW-based parameters, Dm* and β*, exhibited the highest AUC of 0.927 and a sensitivity of 0.900, surpassing their classical CTRW-based counterparts. Notably, β* demonstrated strong accuracy (0.843), coming very close to the performance of ADC, which was the top performer in accuracy (0.857). ADC achieved the highest specificity at 0.933, although at the expense of a lower sensitivity.Discussion
We have investigated the performance of DISMANTLE in grading pediatric brain tumors and showed that diffusion-related DISMANTLE parameters produced statistically significantly lower values in high-grade tumors. This is consistent with previous studies5 and can be attributed to the inherent complexity and heterogeneity of high-grade tumors. Notably, the spatial heterogeneity parameter β* achieved a considerably higher sensitivity than ADC (90% vs. 80%) with only a marginally lower overall accuracy (84.3% vs. 85.7%), showing promise as a superior parameter than ADC. Importantly, while perfusion-related DISMANTLE parameters showed no significant differences between tumor grades, removal of perfusion-related signal using DISMANTLE enhanced accuracy for all three CTRW-based diffusion-related parameters, Dm*, ⍺*, and β*, when compared to the standard CTRW model.Conclusion
Our results suggest that DISMANTLE not only offers a unified framework for characterizing perfusion and diffusion-related DWI signals but also improves the performance of a high b-value non-Gaussian model – the CTRW model.Acknowledgements
No acknowledgement found.References
Ostrom QT, Cioffi G, Gittleman H, et al. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012-2016. Neuro Oncol. 2019 Nov 1;21(Suppl 5):v1-v100.
Chen L, Liu M, Bao J, et al. The correlation between apparent diffusion coefficient and tumor cellularity in patients: A meta-analysis. PLoS One. 2013;8(11).
Moffat BA, Chenevert TL, Lawrence TS, et al. Functional diffusion map: A noninvasive MRI biomarker for early stratification of clinical brain tumor response. Proc Natl Acad Sci U S A. 2005;102(15):5524-5529.
Iima M, Le Bihan D. Clinical intravoxel incoherent motion and diffusion MR imaging: past, present, and future. Radiology. 2016;278:13–32.
Karaman MM, Sui Y, Wang H, et al. Differentiating low- and high-grade pediatric brain tumors using a continuous-time random-walk diffusion model at high b-values. Magn Reson Med. 2016;76(4):1149-1157.
Karaman M, Bu Y, Dan G, et al. A Hybrid DWI Approach for Simultaneous Assessment of Cellularity, Vascularity, and Heterogeneity of Breast Lesions. Proc ISMRM Meeting; 2021; S0139
Figures
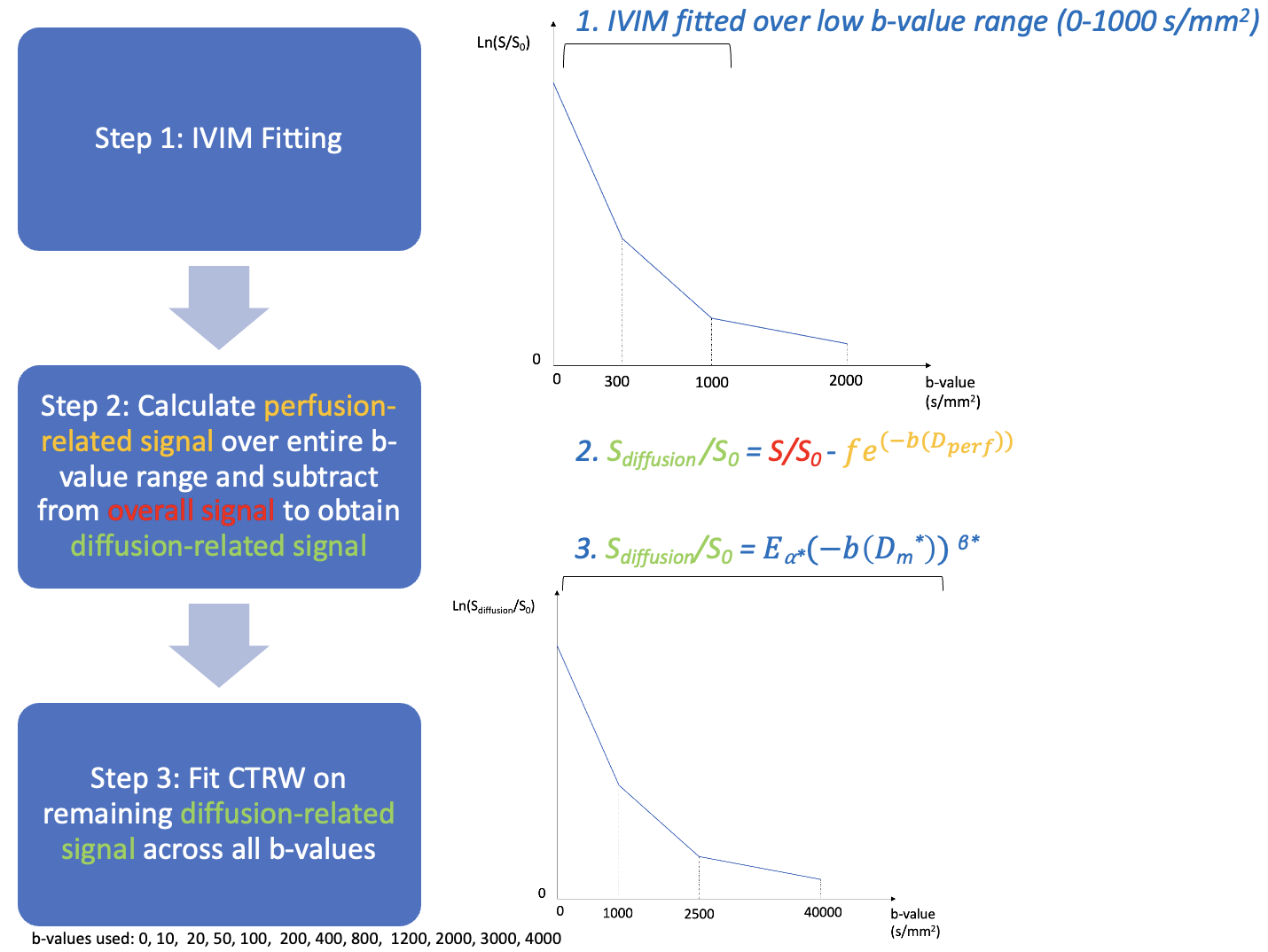
Figure 1: DISMANTLE uses a segmented fitting approach that combines both the IVIM and CTRW models. After fitting the IVIM model to the trace-weighted DWI data in the lower b-value range (0-1000 s/mm2), the perfusion component was subtracted from overall signal, followed by fitting the CTRW parameters to the remaining signals across all b-values.
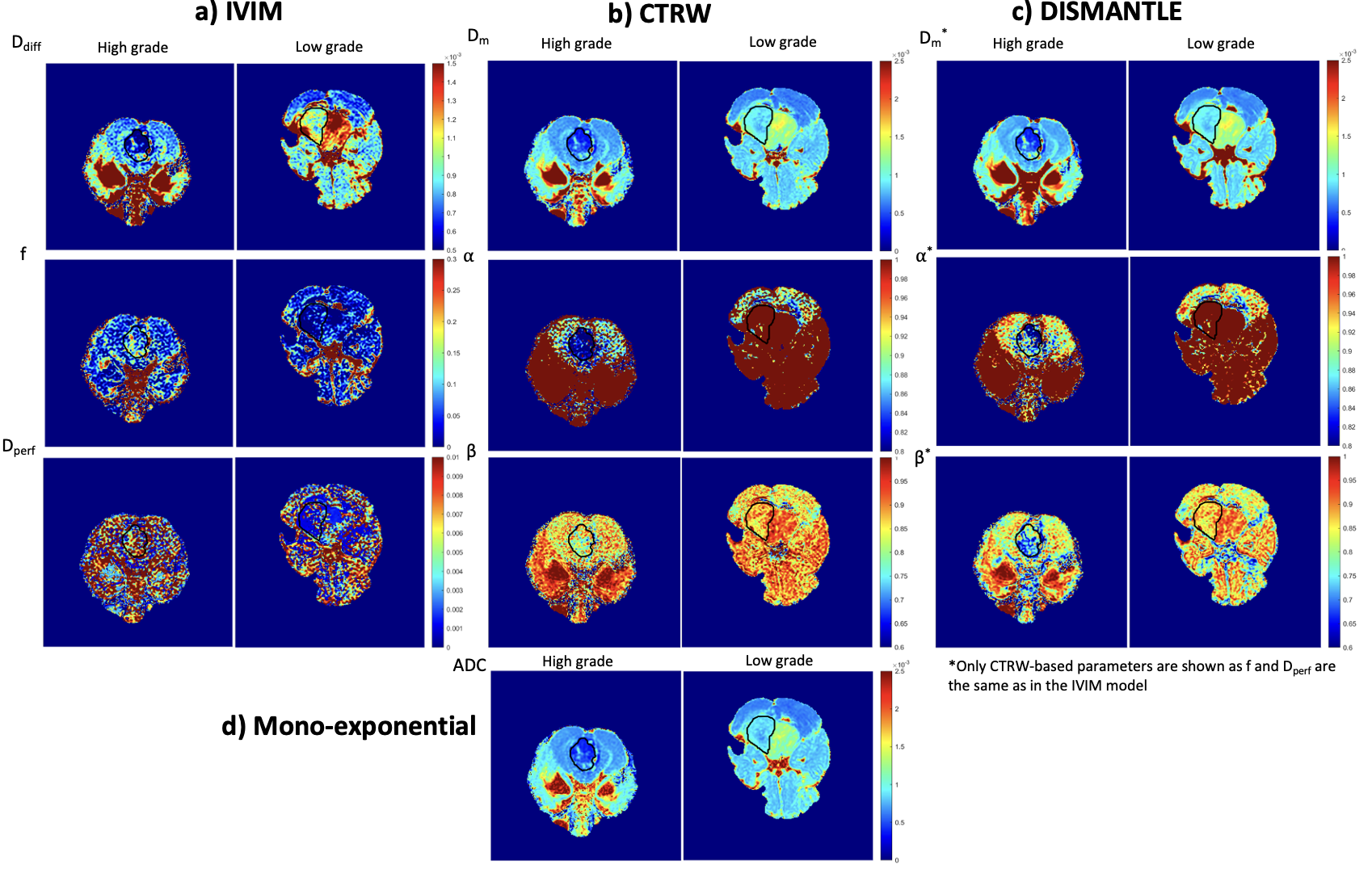
Figure 2: The Parameter maps from a) IVIM, b) CTRW, c) DISMANTLE , and d) mono-exponential model (ADC) from representative patients in the high-grade (left column) and low-grade (right column) patient groups. Notable differences between high- and low-grade tumors can be observed in ADC, Ddiff, ⍺, ⍺*, β, β*, Dm, and Dm*. Other acquisition parameters were: TR/TE=4700/100ms, slice thickness=5mm, Δ=38.6 ms, δ=32.2ms, FOV=22cm×22cm, matrix size=128×128.