2398
Changes in Working Memory Structural Connectomes During Reduced Intensity Therapy for WNT-subtype Medulloblastoma1Diagnostic Imaging, St Jude Children's Research Hospital, Memphis, TN, United States, 2Biostatistics, St Jude Children's Research Hospital, Memphis, TN, United States, 3Psychology and Biobehavioral Sciences, St Jude Children's Research Hospital, Memphis, TN, United States, 4Radiation Oncology, St Jude Children's Research Hospital, Memphis, TN, United States, 5Oncology, St Jude Children's Research Hospital, Memphis, TN, United States
Synopsis
Keywords: Structural Connectivity, Cancer
Motivation: Cognitive impairment following treatment of medulloblastoma has been associated with white matter structural changes and altered structural brain connectivity.
Goal(s): We hypothesized that decreased intensity therapy would reduce acute change in the working memory structural connectome.
Approach: Working memory structural connectomes were assessed relative to baseline after 15 Gy craniospinal irradiation (RT), after subsequent reduced-intensity chemotherapy, and during follow-up for 24 children treated for WNT-subtype (WNT) medulloblastoma.
Results: Changes after RT or chemotherapy showed small increases in connectivity strength in frontal striatal edges indicating little acute change. Follow-up revealed significant decreases in connectivity of the bilateral connections between caudate/thalamus.
Impact: Increased connectivity of frontal striatal edges after therapy and decreased connectivity of caudate/thalamus edges in follow-up for patients receiving reduced intensity therapy for WNT medulloblastoma may indicate a low incidence of acute changes.
INTRODUCTION
Cognitive impairment following treatment of medulloblastoma (MB), the most common malignant brain tumor in children, includes processing speed, attention, working memory, and executive functions being the most affected domains.1,2 These changes in cognition have been associated with white matter structural changes and altered structural brain connectivity.3,4 We hypothesized that decreased intensity of therapy would reduce acute change in the working memory structural connectome.METHODS
MB participants were assigned to treatment strata based first on molecular subgroup and then by clinical risk stratification. All patients were treated with risk-adapted radiation therapy (RT) and adjuvant chemotherapy. WNT-subtype comprises 10% of all medulloblastomas5,6 and have an excellent prognosis with overall survival exceeding 90% using standard therapy.7,8 To reduce the intensity of therapy for this cohort, patients received reduced dose craniospinal irradiation (15 Gy) and primary site boost (51Gy, cumulative total).A total of 31 WNT patients were treated at a single institution. One participant either missed or had metal artifacts in all time points and six had no baseline imaging. A cohort of 24 subjects (median age at baseline 10.6 years [5.3-22.0 years]; 14 female) was available for the analysis. Imaging protocols were approved by the local Institutional Review Board, and written informed consent was obtained from the patient, parent, or guardian, as appropriate.
Imaging was conducted on a Siemens 3T magnet at four time points: baseline (after resection of the tumor and prior to adjuvant therapy), post-RT, post-chemotherapy (12-months), and 18-months after baseline. A 3D sagittal T1 MPRAGE image was acquired: TR=1980 ms; TE=2.26 ms; TI=1100 ms; Flip angle =15 degrees; 1 mm3 isotropic. Diffusion imaging was acquired using bipolar diffusion-encoding gradients with a double-spin echo, simultaneous multi-slice, multi-echo planar imaging pulse sequence: TR= 4000 ms; TE= 78.6 ms, b = 0 , and b = 700 or 1500 s/mm2 at 30 or 64 directions, respectively; 1.8 mm isotropic resolution; Multi-band-factor: 4. The acquisition was performed twice with reverse blips.
The raw diffusion MR images were initially preprocessed to remove noise, motion and eddy current distortions using FSL and MRtrix3 tool.9,10 The preprocessed images were reconstructed using single-shell multi-tissue constrained spherical deconvolution models to obtain fiber orientation distribution images which were used to generate whole brain tractogram using the probabilistic iFOD2 algorithm.11 The whole brain streamlines were filtered using the SIFT2 method to extract realistic streamlines.12 Connectomes were computed for each subject based on weighted streamline density from the whole brain tractograms.10
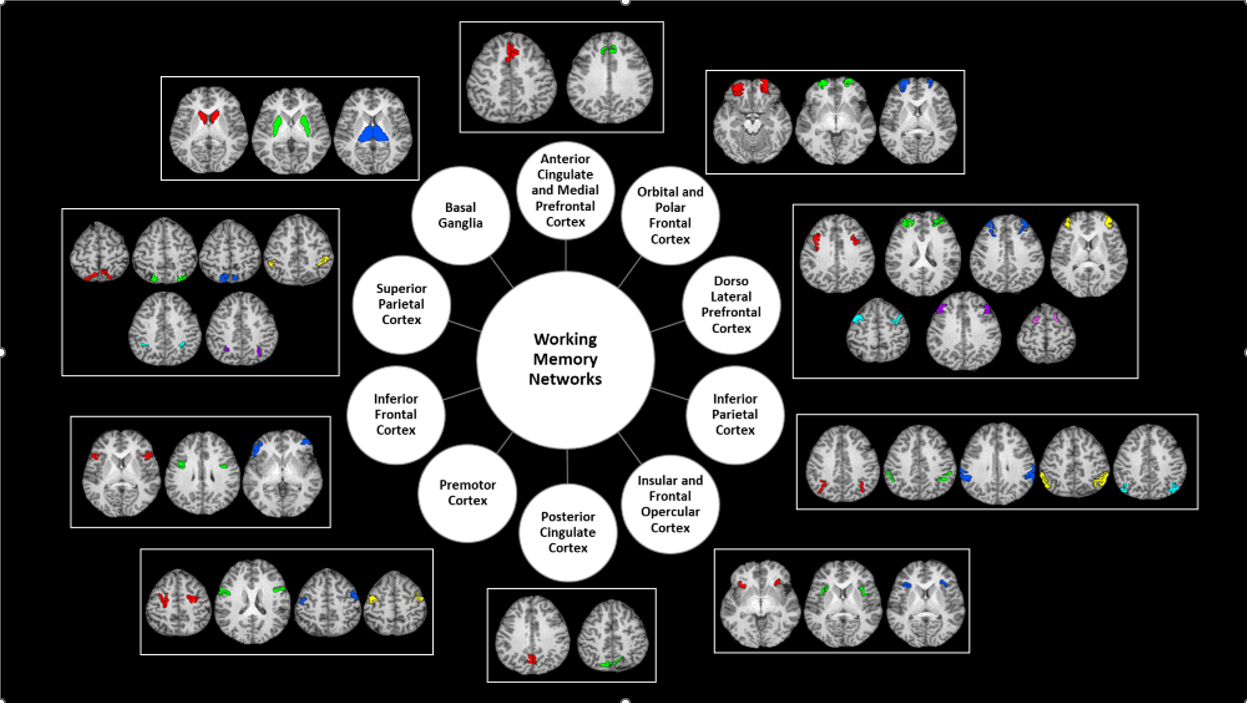
Working memory network regions were identified as the activated regions in 2BK-0BK fMRI task from the HCP-MMP1.0 atlas.13 A total of 24 regions (12 in each hemisphere) were found belonging to the network as shown in Figure 1. To reduce potential noise effects, only edges greater than 0.01 and existing in more than 90% of participants were identified as strong connections. Only bilateral strong connections common across all four timepoints were selected to be included for statistical analysis.
A linear mixed model with random intercept was used for the statistical analysis adjusted for age and sex. Measures during therapy were compared with the baseline for each edge. All analyses were FDR corrected and adjusted p-values < 0.05 were considered significant.
RESULTS
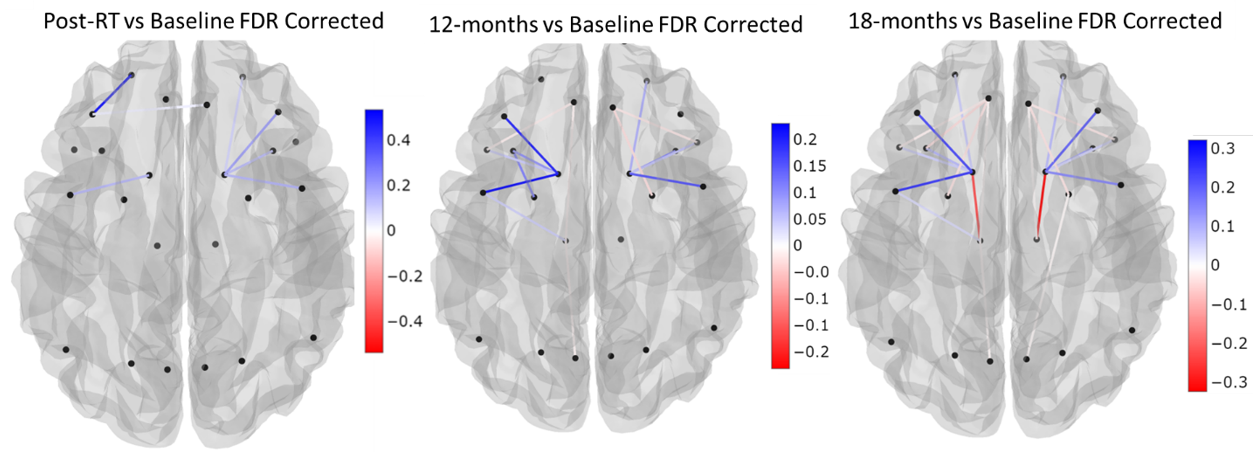
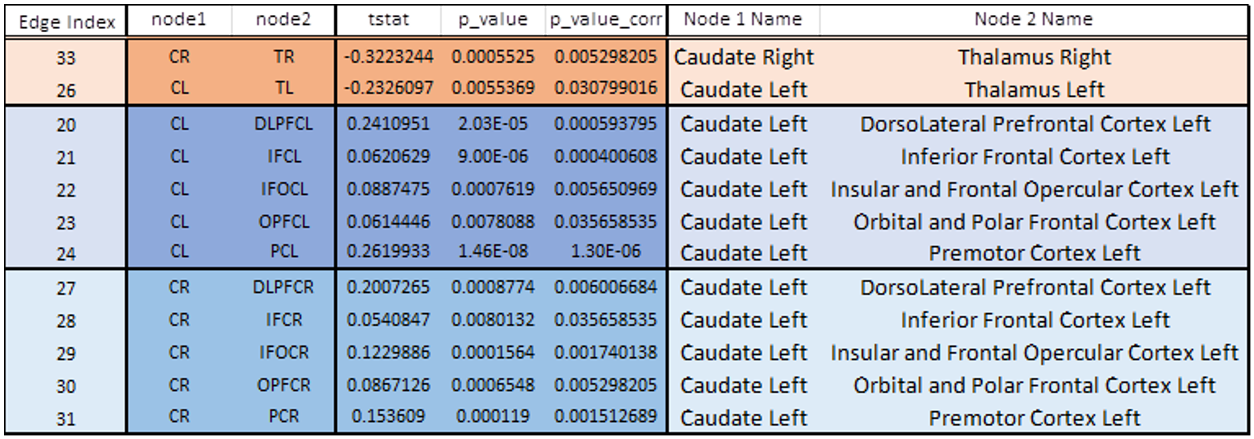
Edges that demonstrated significant differences were compared for post-RT, 12-months, and 18-months relative to baseline are shown in Figure 2. The significant edges for the 18-month follow-up are listed in Figure 3. These results demonstrated that most differences seen were in the frontal striatal edges with increased connectivity and decreased connectivity in the bilateral connections between caudate and thalamus in follow-up.DISCUSSION
Most significant differences in the working memory structural connectome were relatively small and indicated a slight increase in connectivity strength of the frontal striatal edges. These changes could possibly indicate little to no acute changes post irradiation or chemotherapy. However, there were two edges, bilateral connections between caudate and thalamus, at the 18-month follow-up that demonstrated a significant decrease in connectivity. This may possibly be an early indicator of late effects of therapy for a region of white matter that received increased irradiation doses due to the boost to the surgical bed. Associations of edge changes with neurocognitive performance and radiation dosimetry remain to be performed but would further inform this interpretation.CONCLUSION
Increased connectivity of frontal striatal edges after therapy and decreased connectivity of caudate/thalamus edges in follow-up for patients receiving reduced intensity therapy for WNT medulloblastoma support the hypothesis that decreased intensity therapy would result in little acute change in the working memory structural connectome.Acknowledgements
This work was partially supported by the American Lebanese Syrian Associated Charities (ALSAC) at St. Jude Children’s Research Hospital.References
1. Szentes A, Eros N, Kekecs Z, et al. Cognitive deficits and psychopathological symptoms among children with medulloblastoma. Eur J Cancer Care (Engl). Nov 2018;27(6):e12912. doi:10.1111/ecc.12912
2. Saury JM, Emanuelson I. Cognitive consequences of the treatment of medulloblastoma among children. Pediatr Neurol. Jan 2011;44(1):21-30. doi:10.1016/j.pediatrneurol.2010.07.004
3. Duncan EC, Reddick WE, Glass JO, et al. (2016). Application of probabilistic fiber-tracking method of MR imaging to measure impact of cranial irradiation on structural brain connectivity in children treated for medulloblastoma. SPIE Medical Imaging. SPIE vol 9788.
4. Oyefiade A, Beera K, Skocic J, De Medeiros C, Mabbott D. MBCL-34. Structural Connectivity Abnormality in Children Treated for Medulloblastoma. Neuro-Oncology. 20(suppl_2):i124-i124. https://doi:10.1093/neuonc/noy059.430
5. Kool M, Korshunov A, Remke M, et al: Molecular subgroups of medulloblastoma: an international meta-analysis of transcriptome, genetic aberrations, and clinical data of WNT, SHH, Group 3, and Group 4 medulloblastomas. Acta Neuropathol 123:473-84, 2012
6. Ellison DW, Dalton J, Kocak M, et al: Medulloblastoma: clinicopathological correlates of SHH, WNT, and non-SHH/WNT molecular subgroups. Acta Neuropathol 121:381- 96, 2011
7. Gajjar A, Chintagumpala M, Ashley D, et al: Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol 7:813-20, 2006
8. Ellison DW, Onilude OE, Lindsey JC, et al: beta-Catenin status predicts a favorable outcome in childhood medulloblastoma: the United Kingdom Children's Cancer Study Group Brain Tumour Committee. J Clin Oncol 23:7951-7, 2005
9. Smith, S. M., Jenkinson, M., Woolrich, M. W., Beckmann, C. F., Behrens, T. E. J., Johansen-Berg, H., Bannister, P. R., De Luca, M., Drobnjak, I., Flitney, D. E., Niazy, R. K., Saunders, J., Vickers, J., Zhang, Y., De Stefano, N., Brady, J. M., & Matthews, P. M. (2004). Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage, 23(SUPPL. 1), S208-219. https://doi.org/10.1016/j.neuroimage.2004.07.051
10. Tournier, J. D., Smith, R., Raffelt, D., Tabbara, R., Dhollander, T., Pietsch, M., Christiaens, D., Jeurissen, B., Yeh, C. H., & Connelly, A. (2019). MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. NeuroImage, 202(August), 116137. https://doi.org/10.1016/j.neuroimage.2019.116137
11. Jeurissen, B., Tournier, J. D., Dhollander, T., Connelly, A., & Sijbers, J. (2014). Multi-tissue constrained spherical deconvolution for improved analysis of multi-shell diffusion MRI data. NeuroImage, 103. https://doi.org/10.1016/j.neuroimage.2014.07.061
12. Smith, R. E., Tournier, J. D., Calamante, F., & Connelly, A. (2015). SIFT2: Enabling dense quantitative assessment of brain white matter connectivity using streamlines tractography. NeuroImage, 119. https://doi.org/10.1016/j.neuroimage.2015.06.092
13. Glasser, M. F., Coalson, T. S., Robinson, E. C., Hacker, C. D., Harwell, J., Yacoub, E., Ugurbil, K., Andersson, J., Beckmann, C. F., Jenkinson, M., Smith, S. M., & Van Essen, D. C. (2016). A multi-modal parcellation of human cerebral cortex. Nature, 536(7615), 171–178. https://doi.org/10.1038/nature18933
Figures