2395
Associations Between Neurometabolite Levels and Sleep Quality in Survivors of Pediatric Hodgkin Lymphoma (HL)1Psychology and Biobehavioral Sciences, St. Jude Children's Research Hospital, Memphis, TN, United States, 2Diagnostic Imaging, St. Jude Children's Research Hospital, Memphis, TN, United States, 3Oncology, St. Jude Children's Research Hospital, Memphis, TN, United States, 4Epidemiology and Cancer Control, St. Jude Children's Research Hospital, Memphis, TN, United States, 5Nursing Research, St. Jude Children's Research Hospital, Memphis, TN, United States
Synopsis
Keywords: Cancer, Cancer, survivorship, late effects, apnea, sleep
Motivation: Survivors of pediatric Hodgkin’s lymphoma (HL) have excessive daytime sleepiness and fatigue, with substantial consequences to quality of life. Thoracic radiation therapy (TRT), traditionally used to treat HL, is associated with cardiopulmonary morbidity and may result in sleep apnea.
Goal(s): Although sleep is known to impact neurometabolites in the general population, its effect on neurometabolite concentrations in HL survivors has not been established.
Approach: The present study used magnetic resonance spectroscopy (MRS) to explore the relationship between neurometabolites and sleep quality in pediatric HL survivors and community controls.
Results: We found associations between metabolites associated with excitotoxicity and neuroinflammation with sleep and age.
Impact: Our findings may identify therapeutic targets for interventions that mitigate the treatment-related late effects commonly experienced by HL survivors. Our results suggest that excitotoxicity and neuroinflammation could mediate the impact of sleep disturbances on age-associated late effects of cancer treatment.
Introduction
Survivors of pediatric HL are burdened by heightened levels of fatigue and daytime sleepiness, which undermines quality of life and leads to further adverse health outcomes1,2. Our research group has hypothesized that HL survivors experience sleep problems as a consequence of thoracic radiation therapy (TRT): namely, that TRT causes damage to cardiac and respiratory structures necessary for sleep, leading to an increased incidence of obstructive sleep. The present study aimed to explore the relationship between sleep quality and neurometabolite levels in a sample of adult survivors of pediatric HL compared to community controls. We hypothesized that metabolites pertaining to brain aging, neuroinflammation, and oxidative stress would be associated with age and cancer survivorship. We also hypothesized that metabolites associated with cell turnover would be associated with cancer survivorship and that neurotransmitter-related metabolites would be associated with sleep, regardless of survivorship status.Methods
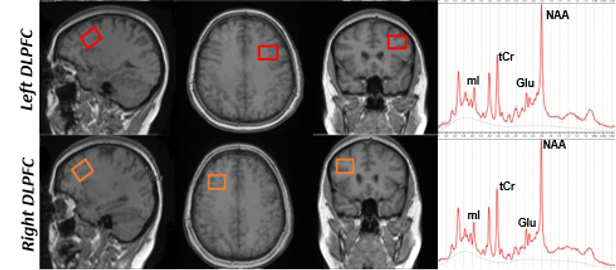
HL survivors (N = 11; 45.5% female; mean age = 33.2 years, SD = 9.5 years) and control subjects (N = 35, 48.6% female, mean age = 40.3, SD = 11 years) completed nighttime polysomnography and proton magnetic resonance spectroscopy (MRS). The MRS was collected from bilateral dorsolateral prefrontal cortex (dlPFC), focusing on neurometabolites related to membrane turnover (Choline: Cho), oxidative stress (glutathione: GSH), brain aging (N-acetyl aspartate: NAA), neuroinflammation (myo-inositol: MI), as well as neurotransmitter-related neurometabolites (Glutamate: Glu; Glutamate + Glutamine: Glx). To measure sleep disturbance, we focused on the apnea-hypopnea index (AHI) derived from nighttime polysomnographic recordings, which measures the average number of apnea (cessation of breathing) and hypopnea (shallow breathing) events per hour of sleep.MRS data were acquired on a 3T MRI scanner (Siemens Medical Systems, Erlangen, Germany). Acquisition of MRS data was preceded by a T1-weighted MPRAGE scan (TR/TE/ 6.9/3.2 ms; FA 8°) with 1 mm3 isotropic resolution for voxel positioning and tissue segmentation. PRESS localization (1.3 kHz refocusing bandwidth) was employed to acquire metabolite spectra with voxels localized in the right and left dorsolateral prefrontal cortex (DLPFC) (20x20 mm3) as shown in Fig 1. PRESS localization was configured with the following parameters: TR/TE: 2000/30 ms; 30 × 26 × 26 mm3. Regional concentrations of each metabolite were determined using LCmodel software. Metabolites in the present analysis are expressed as concentration ratios relative to total creatine (tCr). Metabolite ratios with an SD>30 were included in the analysis. Polysomnography data were collected using a Sleep Profiler PSG2 system. Participants' breathing was measured using a nose cannula and respiration belt.
To determine the effect of sleep quality on neurometabolite levels in survivors vs control subjects, we computed interaction tests modeling the effect of AHI and group (survivor vs control) on each metabolite. A significant interaction effect from these tests can be interpreted as a significant difference in the slope of the relationship between AHI and metabolite between survivors vs control subjects. We then conducted similar interaction tests modeling the effect of age and group on each metabolite. We conducted multiple comparisons correction using the Bonferroni method based on the a-priori hypotheses outlined in the Introduction.
Results
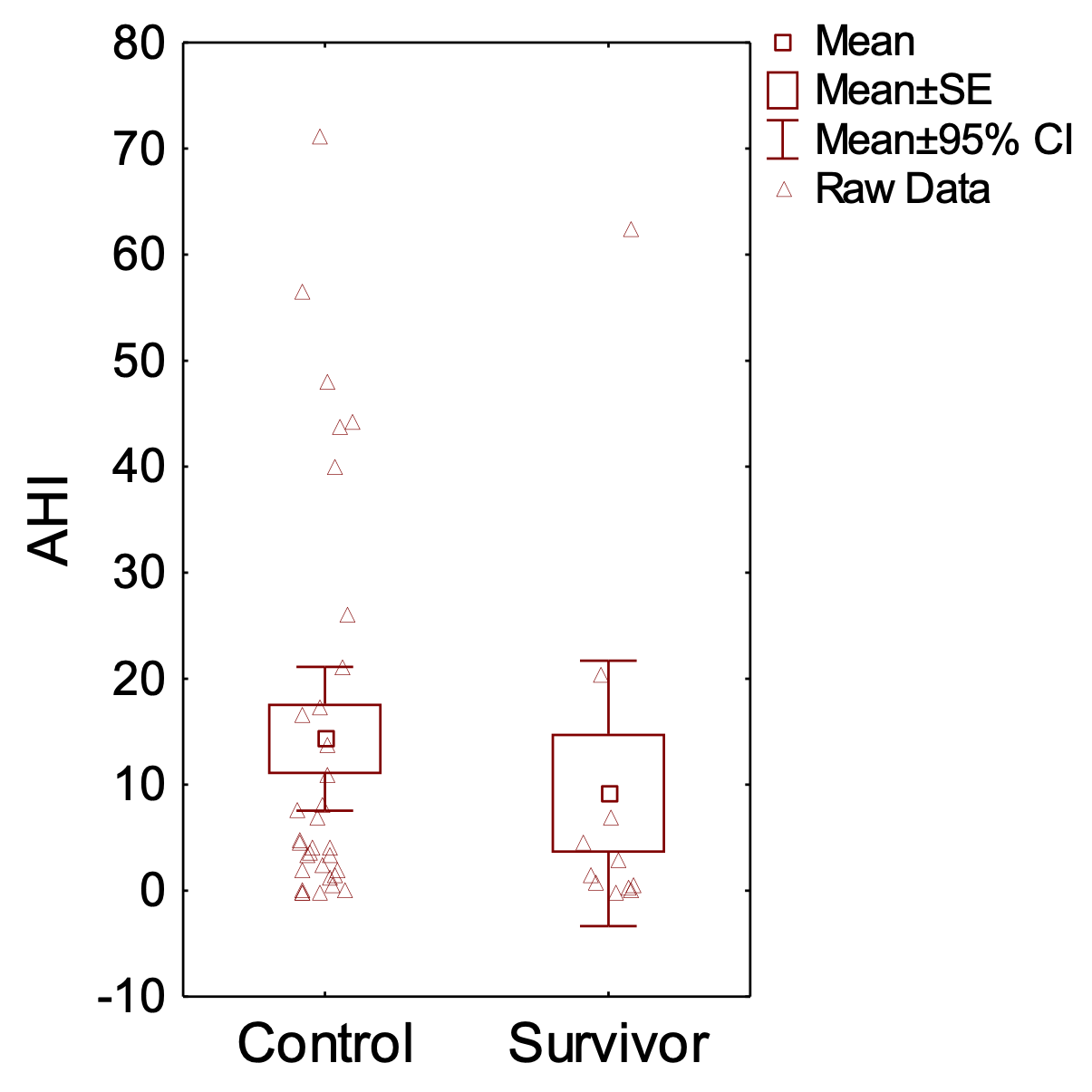
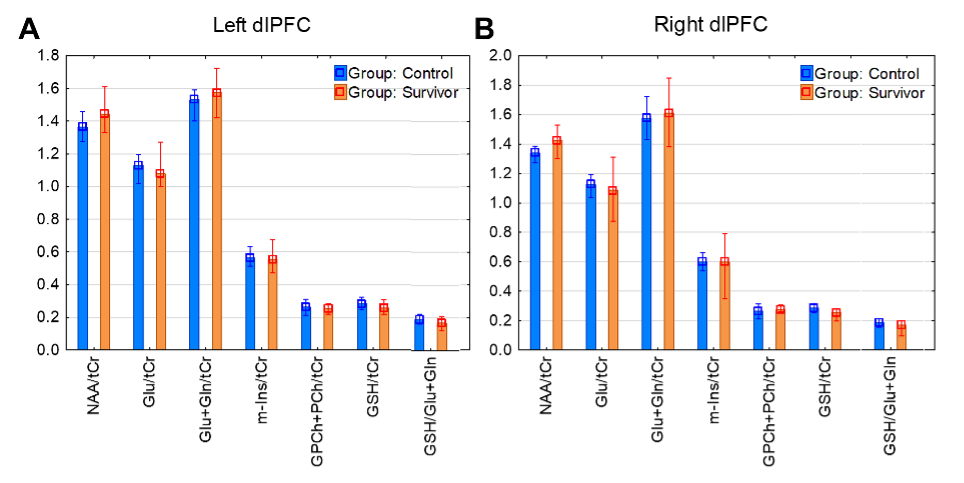
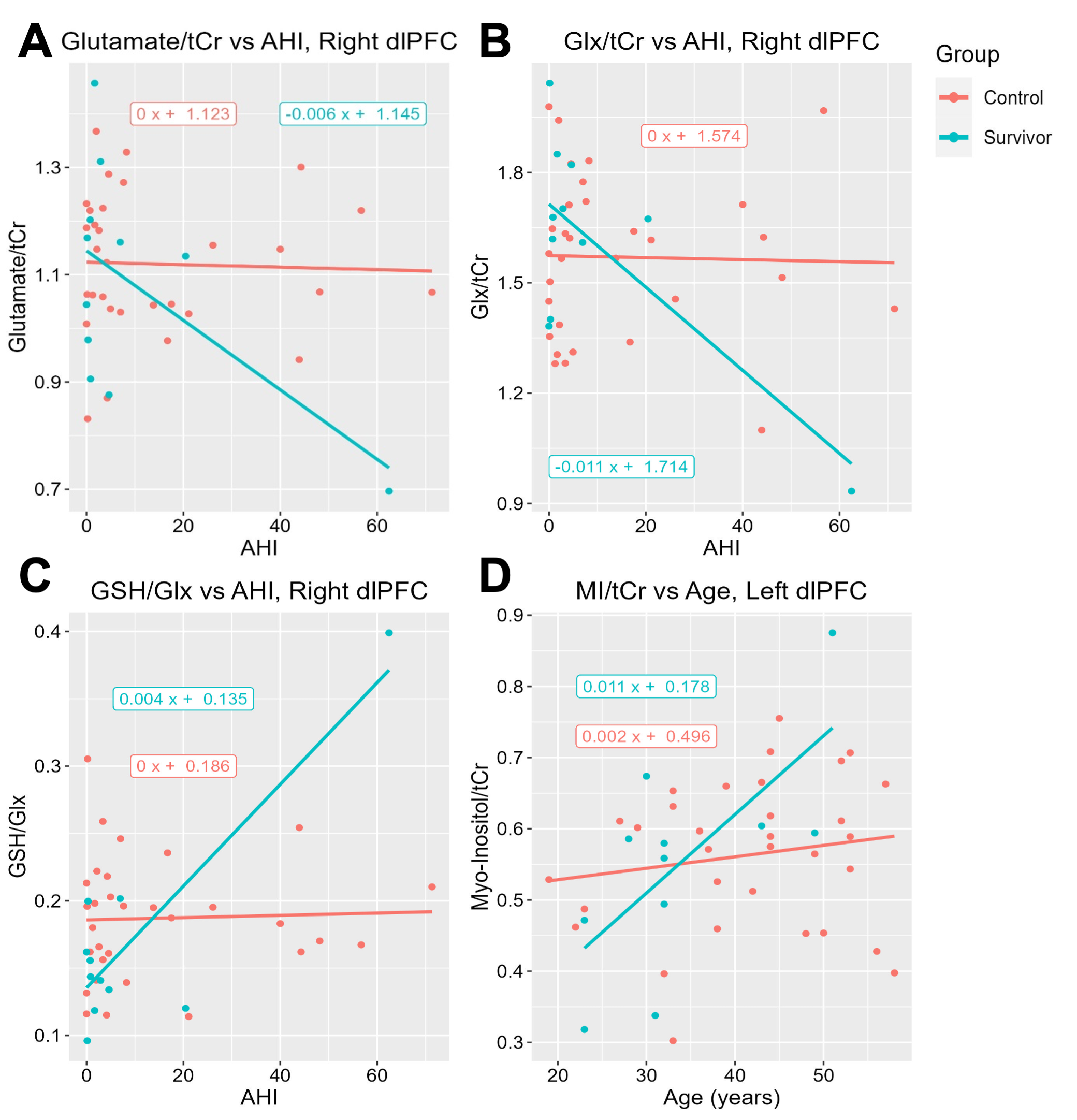
One-way ANOVA found no significant differences in AHI between survivors and control subjects (Fig. 2). Furthermore, we found no significant differences in metabolite levels in the dlPFC between survivors and controls after correcting for multiple comparisons (Fig. 3).In survivors, Glu (Fig. 4A) and Glx (Fig. 4B) were negatively associated with AHI, and GSH/Glx (Fig. 4C) was positively associated with AHI. We also found a positive relationship between age and MI in survivors (Fig. 4D). Meanwhile, control subjects showed no such association(s). We found significant interactions effects for Glu (p = 0.034), Glx (p = 0.014), and GSH/Glx (p = 0.00016) with AHI in right dlPFC, as well as a significant interaction for MI with age in left dlPFC (p = 0.025).
Discussion
These findings suggest that poor sleep has a stronger effect on brain metabolite levels in cancer survivors than in control subjects. Because glutamatergic metabolites were more strongly affected, this may indicate a relationship between excitotoxicity and sleep that is more prominent in cancer survivors than in the general population, possibly as a consequence of cancer treatment. Our finding that myo-inositol is more impacted by age in cancer survivors than control subjects suggests that cancer survivors are particularly vulnerable to neuroinflammation associated with poor sleep.Acknowledgements
No acknowledgement found.References
1. Krull, K. R. et al. Neurocognitive Function and CNS Integrity in Adult Survivors of Childhood Hodgkin Lymphoma. J. Clin. Oncol. 30, 3618–3624 (2012).
2. Phillips, N. S., Duke, E. S., Schofield, H.-L. T. & Ullrich, N. J. Neurotoxic Effects of Childhood Cancer Therapy and Its Potential Neurocognitive Impact. J. Clin. Oncol. 39, 1752–1765 (2021).
Figures