2386
Altered cerebral oxygen extraction and metabolism in preterm neonates and the relationship to anemia: a non-contrast MRI study1Department of Biomedical Engineering, Zhejiang University, Hangzhou, China, 2Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 3Department of Radiology, Shengjing Hospital of China Medical University, Shengyang, China
Synopsis
Keywords: Neonatal, Pediatric
Motivation: The effect of preterm birth on cerebral oxygenation and its underlying mechanism have not been fully elucidated.
Goal(s): The goal of current study is to evalute cerebral oxygenation with non-contrast MRI techniques in a group of preterm-born neonates.
Approach: Cerebral oxygen extraction fraction (OEF) and metabolic rate of oxygen (CMRO2) were measured with TRUST MRI together with cerebral blood flow (CBF) in 50 neonates.
Results: We showed that neonates with lower gestational age had higher OEF, lower CBF and lower CMRO2, controlling for postmenstrual age. Higher OEF was associated with higher Apgar score. Hematocrit significantly mediated the increase of OEF in preterm neonates.
Impact: The results suggested a potential role of MRI-based oxygenation measurement in the assessment of transfusion and intervention for preterm neonates.
INTRODUCTION
Due to a less-developed cerebral vasculature or disrupted auto-regulation1-3, oxidative metabolism can be altered in preterm brain, and may be an upstream cause of structural injuries. However, the underlying mechanism have not been fully elucidated. Furthermore, anemia of prematurity is a common comorbidity in preterm neonates. Oxygen extraction fraction (OEF) was reported to increase as a compensation in these patients4-6. A better understanding of the interplay among preterm, anemia and oxygen metabolism may be important for assessing the need of transfusion.In this study, we aim to assess cerebral oxygen extraction and metabolism in neonates with gestational age (GA) of 28-42 weeks. We examined the GA dependence of OEF, cerebral metabolic rate of oxygen (CMRO2) and cerebral blood flow (CBF). We also explored the mediation effect of anemia on the association between preterm and cerebral oxygenation.
METHODS
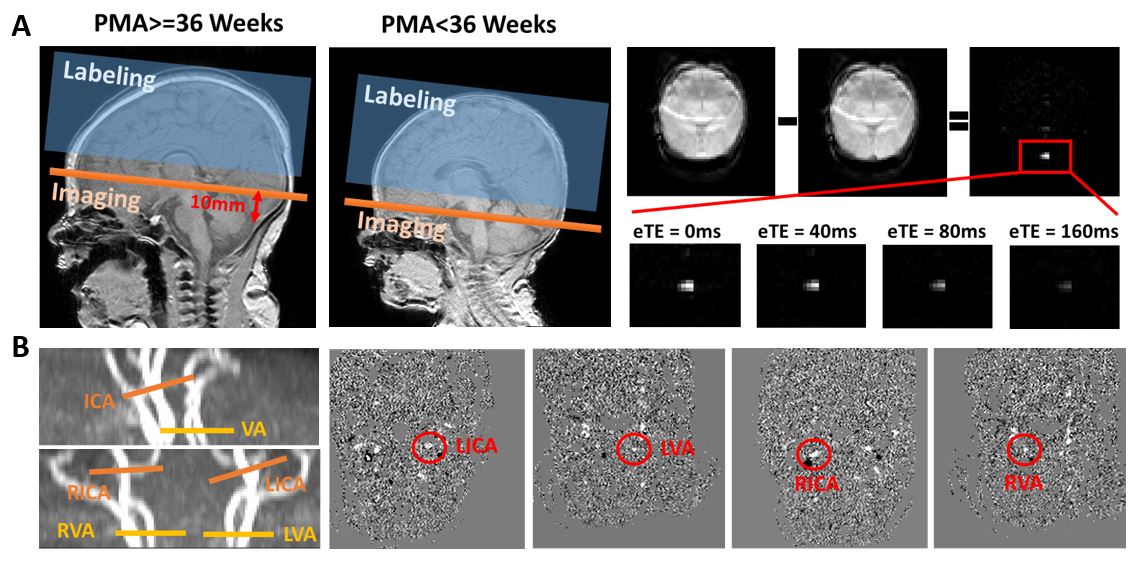
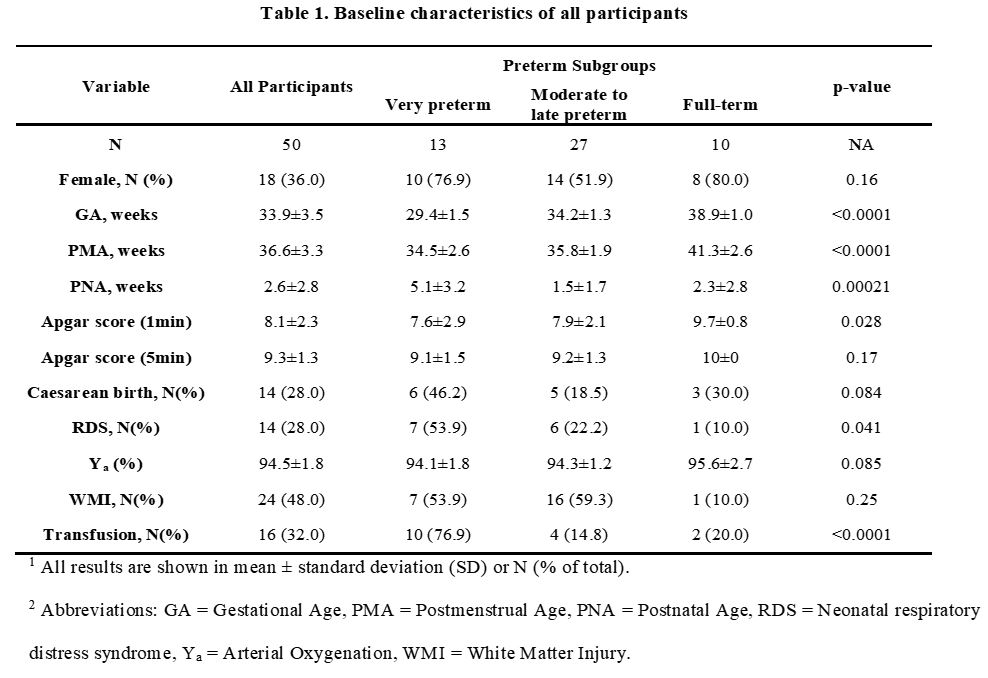
A total of 50 neonatal participants were recruited with a PMA at MRI scan of 36.6±3.3 weeks. Among them, 13 were very preterm-born with a GA<32 weeks, 27 were moderate to late preterm-born with a GA of 32 to 37 weeks, and 10 were full-term with a GA>38 weeks.All MRI scans were performed on a 3T Philips System. Standard clinical scans were first performed and a binary rating for white matter injury was given to each participant. Global venous oxygenation (Yv) was measured non-invasively with T2-relaxation-under-spin-tagging (TRUST) MRI which isolates the venous blood signal using spin labeling, followed by a series of T2 preparation pulses. Subtraction between control and label images yield pure venous blood signal and mono-exponential fitting was applied to obtain venous T2, which was converted to Yv using a neonatal calibration model. OEF was then calculated using , where Ya is arterial oxygenation. In order to assess CBF, phase-contrast (PC) MRI was acquired for four feeding arteries, i.e. left and right internal carotid arteries, left and right vertebral arteries with encoding velocity=20cm/s. Global CBF was calculated by normalizing the total flux of four arteries with brain volume. CMRO2 was calculated based on Fick Principle: CMRO2=CBF·(Ya-Yv)·Ch, where Ch is the amount of oxygen that a unit of volume of blood can carry.
Concentration of hematocrit (Hct) was determined using blood samples drawn on the day of MRI scan. Apgar score measured shortly after birth was also retrieved.
The relationship between cerebral physiological parameters, i.e. OEF, CBF and CMRO2, and GA was assessed using linear regression analysis, where the physiological parameter was the dependent variable and GA was the independent variable, with PMA and sex as covariates. The association between cerebral physiology and Apgar scores was evaluated similarly. Finally, mediation analysis was performed, where GA was the independent variable, Hct was the mediator and physiological parameter was the dependent variable, using a bootstrap method.
RESULTS
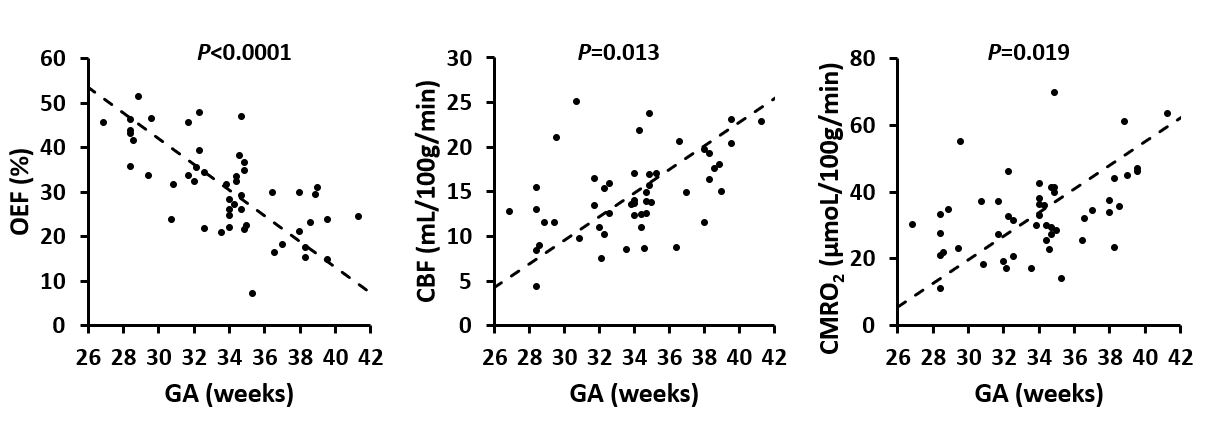
The baseline characteristics of these participants was summarized in Figure 2. As expected, Hct decreased as PNA increased (β=-1.78, p=0.00011), and increased as GA increased (β=1.22, p=0.00093).As shown in Figure 3, GA had a significant negative relationship with OEF (β=-0.019, p<0.0001) and positive relationships with CBF (β=0.61, p=0.013) and CMRO2 (β=1.55, p=0.019), correcting for PMA and sex. These relationships preserved when accounting for respiratory distress syndrome or white matter injury.
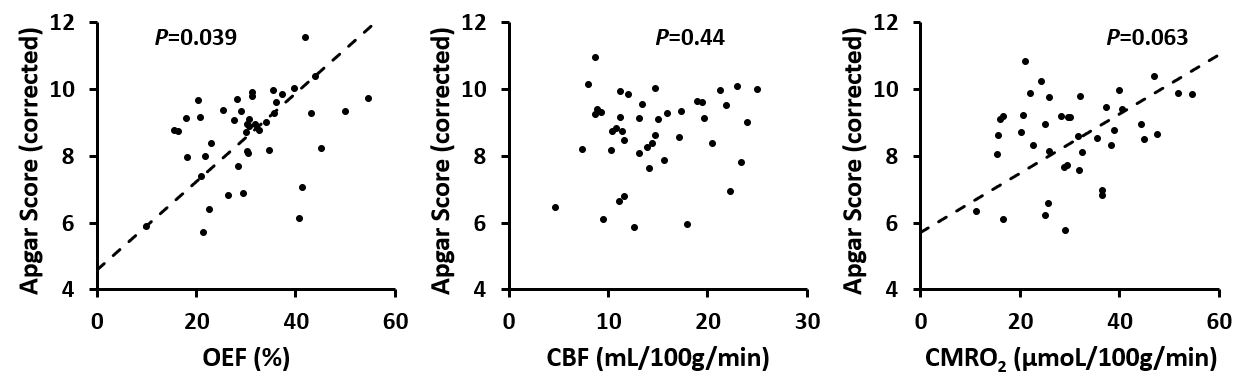
It was also found that higher Apgar score was associated with higher OEF (β=5.18, p=0.039) and a trend of higher CMRO2 (β=0.032, p=0.063), but not with CBF, after accounting for GA, PMA and sex (Figure 4).
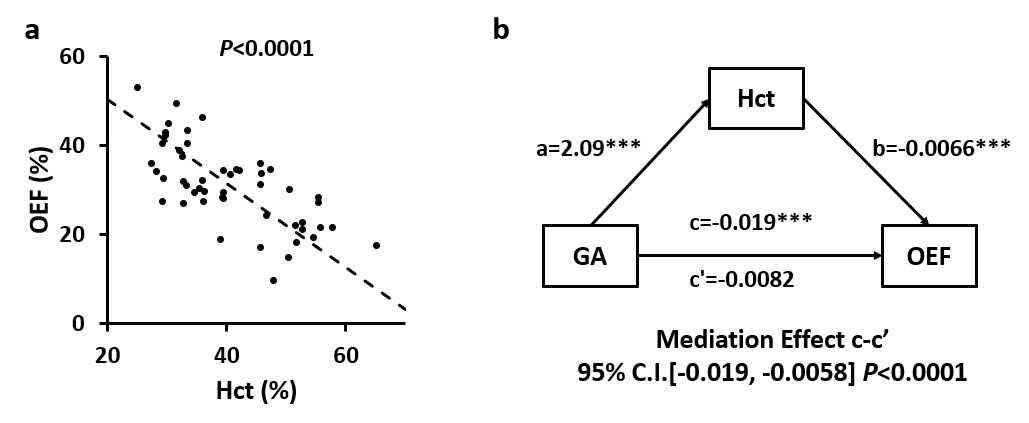
Regression analysis showed that neonates with a lower hematocrit had a significantly higher OEF (β=-0.0066, p<0.0001, Figure 5), but not CMRO2 and CBF. Mediation analysis suggested that the negative effect of GA on OEF was significantly mediated by Hct (95% CI [-0.019, -0.0058], p<0.0001).
DISCUSSION AND CONCLUSION
Most studies on cerebral oxygenation in preterm-born neonates were not conducted at term-equivalent age or did not control for PMA, i.e. the difference may be caused by different maturation time. Our results suggested that even with a same total maturation, neonates with smaller GA still showed a lower CBF and CMRO2, which may be related to the under-development of cerebral vasculature due to an interruption of intrauterine maturation7, 8.Additionally, we found that anemia played a critical role in mediating the association between preterm and oxygen extraction. It is possible that due to a deprivation of in-utero fetal erythropoietin9, red blood cell production is less active, leading to an increase in OEF as a compensation.
These results suggest that OEF may provide important information in clinical assessments of the need of transfusion or intervention.
Acknowledgements
No acknowledgement found.References
1. Schneider J and Miller SP. Preterm brain Injury: White matter injury. Handb Clin Neurol 2019; 162: 155-172. 2019/07/22. DOI: 10.1016/b978-0-444-64029-1.00007-2.
2. Soul JS, Hammer PE, Tsuji M, et al. Fluctuating Pressure-Passivity Is Common in the Cerebral Circulation of Sick Premature Infants. Pediatric Research 2007; 61: 467-473. DOI: 10.1203/pdr.0b013e31803237f6.
3. Verhagen EA, Hummel LA, Bos AF, et al. Near-infrared spectroscopy to detect absence of cerebrovascular autoregulation in preterm infants. Clinical Neurophysiology 2014; 125: 47-52. DOI: https://doi.org/10.1016/j.clinph.2013.07.001.
4. Morris EA, Juttukonda MR, Lee CA, et al. Elevated brain oxygen extraction fraction in preterm newborns with anemia measured using noninvasive MRI. Journal of Perinatology 2018; 38: 1636-1643. DOI: 10.1038/s41372-018-0229-1.
5. Whitehead HV, Vesoulis ZA, Maheshwari A, et al. Progressive anemia of prematurity is associated with a critical increase in cerebral oxygen extraction. Early Human Development 2020; 140: 104891. DOI: https://doi.org/10.1016/j.earlhumdev.2019.104891.
6. Chock VY, Smith E, Tan S, et al. Early brain and abdominal oxygenation in extremely low birth weight infants. Pediatric Research 2022; 92: 1034-1041. DOI: 10.1038/s41390-022-02082-z.
7. Fyfe KL, Yiallourou SR, Wong FY, et al. The development of cardiovascular and cerebral vascular control in preterm infants. Sleep Medicine Reviews 2014; 18: 299-310. DOI: https://doi.org/10.1016/j.smrv.2013.06.002.
8. Piccirilli E, Chiarelli AM, Sestieri C, et al. Cerebral blood flow patterns in preterm and term neonates assessed with pseudo-continuous arterial spin labeling perfusion MRI. Human Brain Mapping 2023; 44: 3833-3844. DOI: https://doi.org/10.1002/hbm.26315.
9. Strauss RG. Anaemia of prematurity: pathophysiology and treatment. Blood Rev 2010; 24: 221-225. 2010/09/08. DOI: 10.1016/j.blre.2010.08.001.
Figures