2378
MRI-based Cerebral Palsy Early Diagnosis in Infants with Periventricular White Matter Injury aged 6 to 24 months: A Multireader Multicase Study1Department of Radiology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China
Synopsis
Keywords: Neuro, Brain, Cerebral palsy, Periventricular white matter injury, MRI, Diagnose, MultiReader MultiCase
Motivation: Early diagnosis of cerebral palsy in infants with periventricular white matter injury is crucial for rehabilitation.
Goal(s): To develop and externally validate a MRI-based model to predict CP in infants with PWMI aged 6 to 24 months, and evaluate the diagnostic performance of the model using the MRMC analysis.
Approach: In this study, A MRI-based multivariable logistic regression model was develop at one center , and was validated at the three centers, and to evaluate the diagnostic performance of the model using the MRMC analysis.
Results: The model showed both excellent predictive performance in the multicenter cohorts and high diagnostic performance in MRMC analysis.
Impact: Our model is a reliable and reproducible tool for diagnosis of CP in infants with PWMI aged 6 to 24 months.
Introduction
The periventricular white matter injury (PWMI) is the most common neuroimaging finding in infants with CP1. Early diagnosis of CP before 2 years is crucial for early Intervention 2-3. Previous studies4,5,6,7 reported the various PWMI-associated MR features; among them, the responsible lesion and weight of CP is unclear, and the PWMI-specific tool to early diagnosis of CP is lacking. To address such issue, we aimed to develop and externally validate a MRI-based model to predict CP in infants with PWMI aged 6 to 24 months, and evaluate the diagnostic performance of the model using the MRMC analysis.Methods
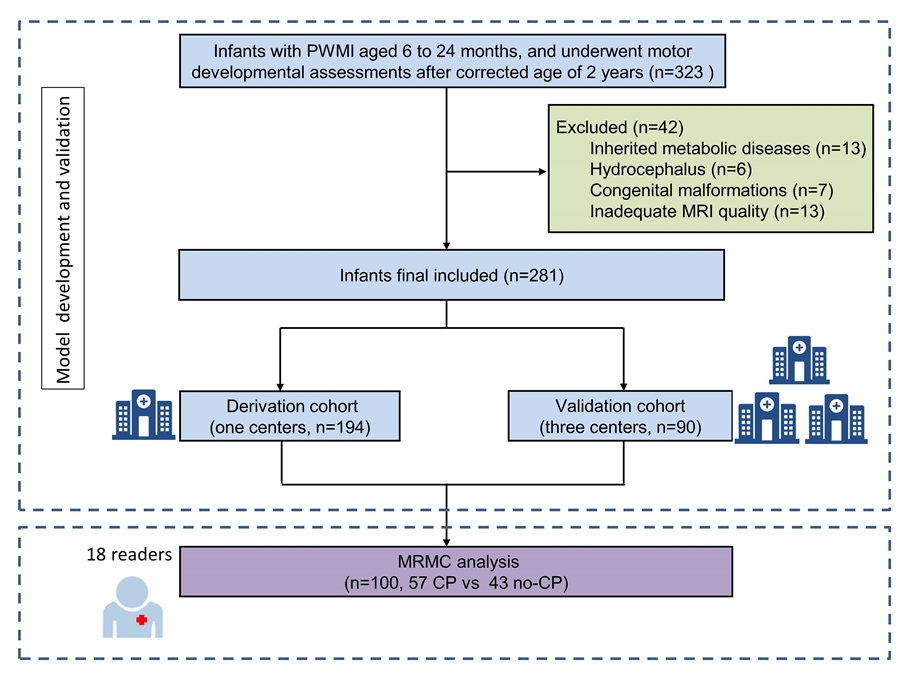
This retrospective multicenter study included infants with suspected CP and diagnosis of PWMI on MRI aged 6 to 24 months from four centers of China, between April 2013 and September 2021. CP was diagnosed according to the international guidelines8. The PWMI-associated lesions were scored using an MRI visual scoring system. A MRI-based multivariable logistic regression model was develop at one center (derivation cohort), and was validated at the three centers (external validation cohort). The predictive performance of the model was assessed by the discrimination, calibration and decision curve in the both two cohorts. To further evaluate the model effects on diagnostic performance of readers, we conducted a MRMC study with 18 readers from 10 centers included both radiologists and neurologist clinicians with a range of experience. Fleiss k statistics was used to analyze interobserver agreement. Analyses were performed with R software (ver 4.2.0, USA) and OR-DBM MRMC (version 2.52). P<0.05 indicated that the difference was statistically significant.Results
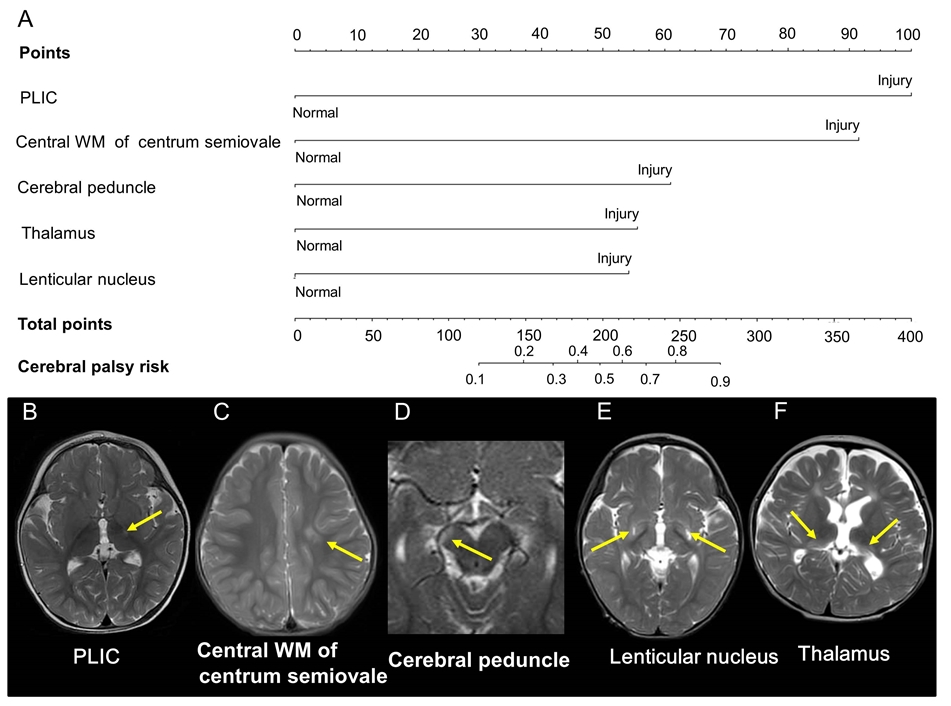
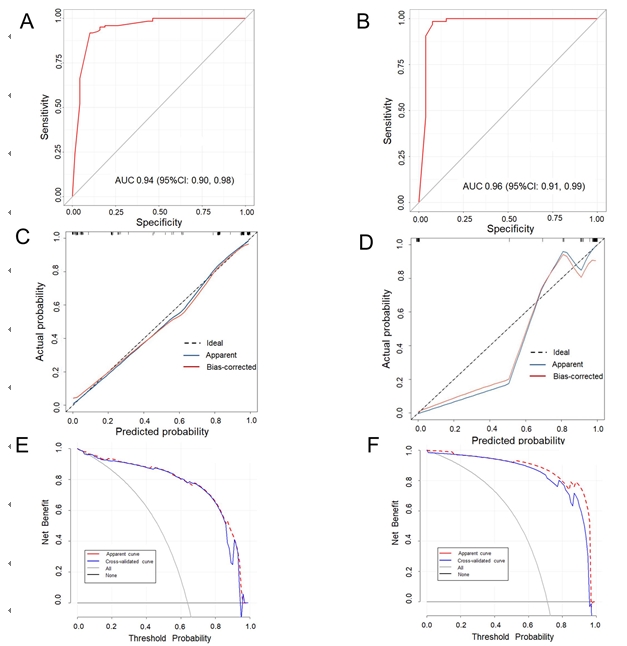
Finally, the derivation cohort consisted of 191 infants (median age, 14 months; IQR, 10-18 months; 122 males), whereas the validation cohort consisted of 90 infants (median age, 14 months; IQR, 10-18 months; 62 males) (Figure 1). Except for a few differences, the baseline characteristics were similar between the derivation and validation cohorts.The results of univariable and multivariable logistic regression analysis are shown in Table 2. Five MRI features were associated with CP: the injury of PLIC (odds ratio [OR], 16.53; 95% CI: 5.54, 49.36), the central white matter of centrum semiovale (OR, 13.01; 95% CI: 3.17, 53.49), the cerebral peduncle (OR, 5.54; 95% CI: 1.10, 27.81), the thalamus (OR, 4.76; 95% CI: 1.32, 17.17), and the lenticular nucleus (OR, 4.58; 95% CI: 1.13, 18.47) (Figure 2) . The model yielded AUCs of 0.94 (95%CI: 0.90, 0.98) in the derivation cohort and 0.96 (95%CI: 0.91, 0.99) in the validation cohort. The calibration curves demonstrated a good consistency between prediction probability and observation probability both in the derivation and validation cohorts (Hosmer-Lemeshow goodness-of-fit test: c2 =5.94, P =0.75 vs c2 =4.12, P =0.90). The decision curve indicating that the model was clinically useful(Figure 3). In the multireader multicase analysis, the readers’ average AUC for CP diagnose were>0.93, sensitivities were 92.3% and specificities were>87.2% in both two reading sessions. The average reading time decreased significantly from 3.1 to 2.7 min. The overall interobserver agreement for CP diagnosis was substantial (k=0.62 to 0.71) and for five MRI features assessment was moderate to substantial (k=0.41 to 0.72).Discussion
In this multicenter study, we developed and external validated a MRI-based model to early diagnosis of CP in infants with PWMI aged 6 to 24 months. These results suggest that the model is a reliable and reproducible tool for early diagnosis of CP in infant with PWMI aged 6 to 24 months. The role of MRI in diagnosis has been previously studied9,10. By comparison, the central WM of the centrum semiovale, PLIC, and cerebral peduncle injury were independent predictors of CP, because these regions are the descending pathway of the CST. These impairments are likely to interrupt motor information transfer of CST, causing considerable disturbances in voluntary motor control. Besides, lenticular nucleus injury has been hypothesized to selectively reduce the activity of the basal ganglia-thalamocortical pathways, thereby causing hyperkinetic movements. Whereas thalamus injury responsible for the sensory deficits and weaken motor coordination or control11. The readers’ average AUC, sensitivities, and specificities across all readers and subgroups in the second session were higher than or equal to those in the first session. This result indicated that the diagnosis performance of model was stably and reliable based on MRI data alone, regardless of reader experience and specialty.Conclusion
The MRI-based model is a reliable and reproducible tool for early diagnosis of CP in infant with PWMI aged 6 to 24 months.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 82204933).References
1. Himmelmann K, Horber V, De La Cruz J, et al. MRI classification system (MRICS) for children with cerebral palsy: development, reliability, and recommendations. Dev Med Child Neurol 2017;59(1):57-64. 2. Novak I, Morgan C, Fahey M, et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr Neurol Neurosci Rep 2020; 20(2):3.
3. Morgan Catherine, Fetters Linda, Adde Lars, et al. Early Intervention for Children Aged 0 to 2 Years With or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA Pediatr 2021;175: 846-858.
4. Novak I, Morgan C, Adde L, et al. Early, accurate diagnosis and early intervention in cerebral palsy: advances in diagnosis and treatment. JAMA Pediatr 2017;171(9):919.
5. Himmelmann K, Horber V, De La Cruz J, et al. MRI classification system (MRICS) for children with cerebral palsy: development, reliability, and recommendations. Dev Med Child Neurol 2017;59(1):57-64. 6. Jauhari P, Singhi P, Sankhyan N, et al. A comparison of spastic diplegia in term and preterm-born children. J Child Neurol 2018;33(5):333-339.
7. Marefi A, Husein N, Dunbar M, et al. Risk Factors for Term-Born Periventricular White Matter Injury in Children With Cerebral Palsy: A Case-Control Study. Neurology. 2022 Nov 29;99(22):e2485-e2493. 8. Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006.Dev Med Child Neurol 2007; 109 (Suppl.): 8-14.
9. Woodward LJ, Anderson PJ, Austin NC, Howard K, et al. Neonatal MRI to predict neurodevelopmental outcomes in preterm infants. N Engl J Med 2006;355(7):685-94.
10. Slaughter LA, Bonfante-Mejia E, Hintz SR,et al. Early Conventional MRI for Prediction of Neurodevelopmental Impairment in Extremely-Low-Birth-Weight Infants. Neonatology 2016;110(1):47-54. 11. Aravamuthan BR, Waugh JL. Localization of Basal Ganglia and Thalamic Damage in Dyskinetic Cerebral Palsy. Pediatr Neurol 2016;54:11-21.
Figures