2375
Evaluation of AI-based Direct Contrast Synthesis in the Pediatric Brain1Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States, 2Philips Research, Hamburg, Germany
Synopsis
Keywords: Neuro, Neuro
Motivation: Direct contrast synthesis (AI-DCS) enables the derivation of synthetic images from a trained neural network. Its utility in clinical practice has yet to be adequately explored.
Goal(s): To evaluate the image quality and diagnostic confidence of these synthetic images in the brain in the pediatric population.
Approach: The study radiologist compares the image quality and diagnostic confidence of AI-DCS images to standard of care (SOC) and SyMRI.
Results: AI-DCS demonstrates better overall image quality and diagnostic confidence than SyMRI on T1, T2 and FLAIR in majority of patients. AI-DCS demonstrates better overall image quality on FLAIR when compared to SOC.
Impact: AI-DCS demonstrates improved image quality and diagnostic confidence compared to SyMRI and comparable image quality to the current standard of care.
Introduction
Synthetic MRI is a technique for generating contrast-weighted images from simultaneously acquired T1, T2 and proton density maps. This approach provides quantitative parameter maps and clinical contrasts from a single 5-minute scan, promising improvements in both the reproducibility and the efficiency of MRI. However, the synthetic images generated through the maps still have suboptimal image quality due to approximations in the signal model, which hinders the clinical adoption of synthetic MRI. AI-based direct contrast synthesis (AI-DCS) has been previously suggested as a promising alternative to improve the image quality of the synthetic images [1] in the context of MR Fingerprinting.
In this work, we investigate the potential of AI-DCS to improve the image quality of the synthetic images compared to SyMRI for pediatric brain. AI-DCS synthetic images are also compared to the standard of care.
Methods
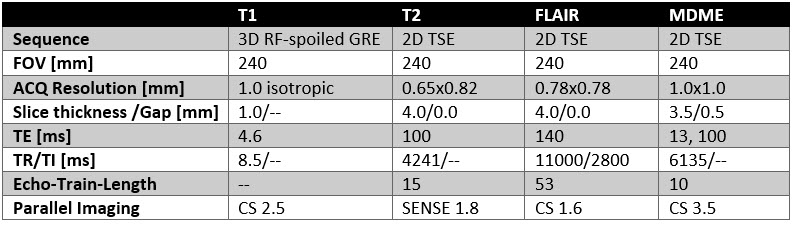
Data acquisition:This is a prospective, IRB approved study in which 50 pediatric patients undergoing clinical brain MRI examinations at Cincinnati Children’s Hospital Medical Center (CCHMC) were enrolled from July 1, 2022 through January 5, 2023. Informed consent was obtained from all study participants, and informed assent was obtained, as appropriate. In addition to the standard of care (SOC) protocol, including 3D T1, and axial T2 and FLAIR, a multi-delay, multi-echo (MDME) [2] was measured. Scan parameters are summarized in Table 1.
Data processing:
Synthetic images were generated from DICOM images of the MDME scan using the SyMRI Neuro software (SyntheticMR, Lund, Sweden). AI-DCS synthetic images were generated using a neural network similar to Ke et al. [1], passing the eight complex AI-DCS images as 16 real-valued channels into the network, similar to [3]. The network simultaneously generates three synthetic images which are trained to approximate the clinical standard of care images for T1w, T2w, and FLAIR sequences. For training the network, the data for 35 patients are assigned as training data with preprocessing involving spatial reorientation to a common frame-of-reference, interpolation to a common matrix size of 320x320 voxels (0.75 mm resolution), denoising of the target images, 2D rigid and deformable registration. The network is implemented in PyTorch, trained using R-ADAM optimizer, using a loss function that combines 90% L1-Loss and 10% Perceptual Loss [4]. The trained network was used to generate synthetic images for the patients in the test set and DICOM images were created for evaluation.
Evaluation:
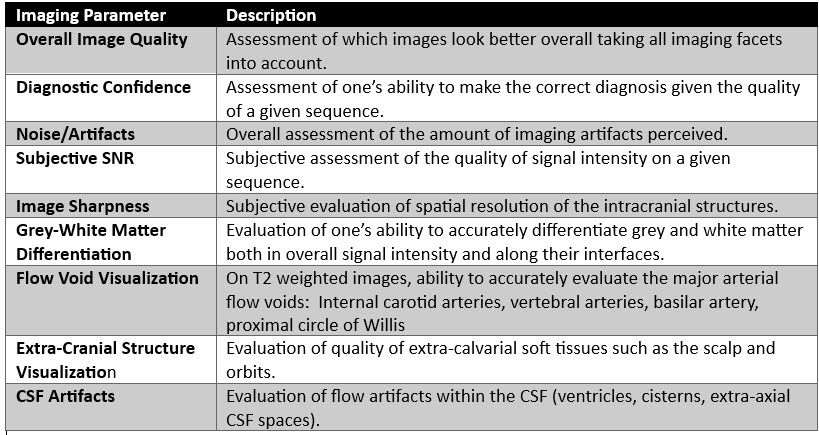
All images were reviewed on a dedicated research PACS by the study radiologist (UN) who was blinded to patient information and clinical data during the review process. Each image was rated on a 3-point scale (worse, same, better) to indicate how AI-DCS image quality compared to the SOC and SyMRI. Descriptive statistical analyses of the reviews were performed. The imaging parameters for rating are described in Table 2.
Results
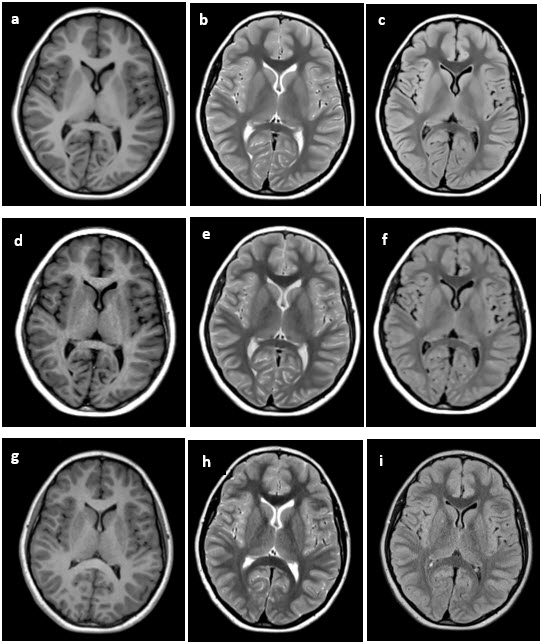
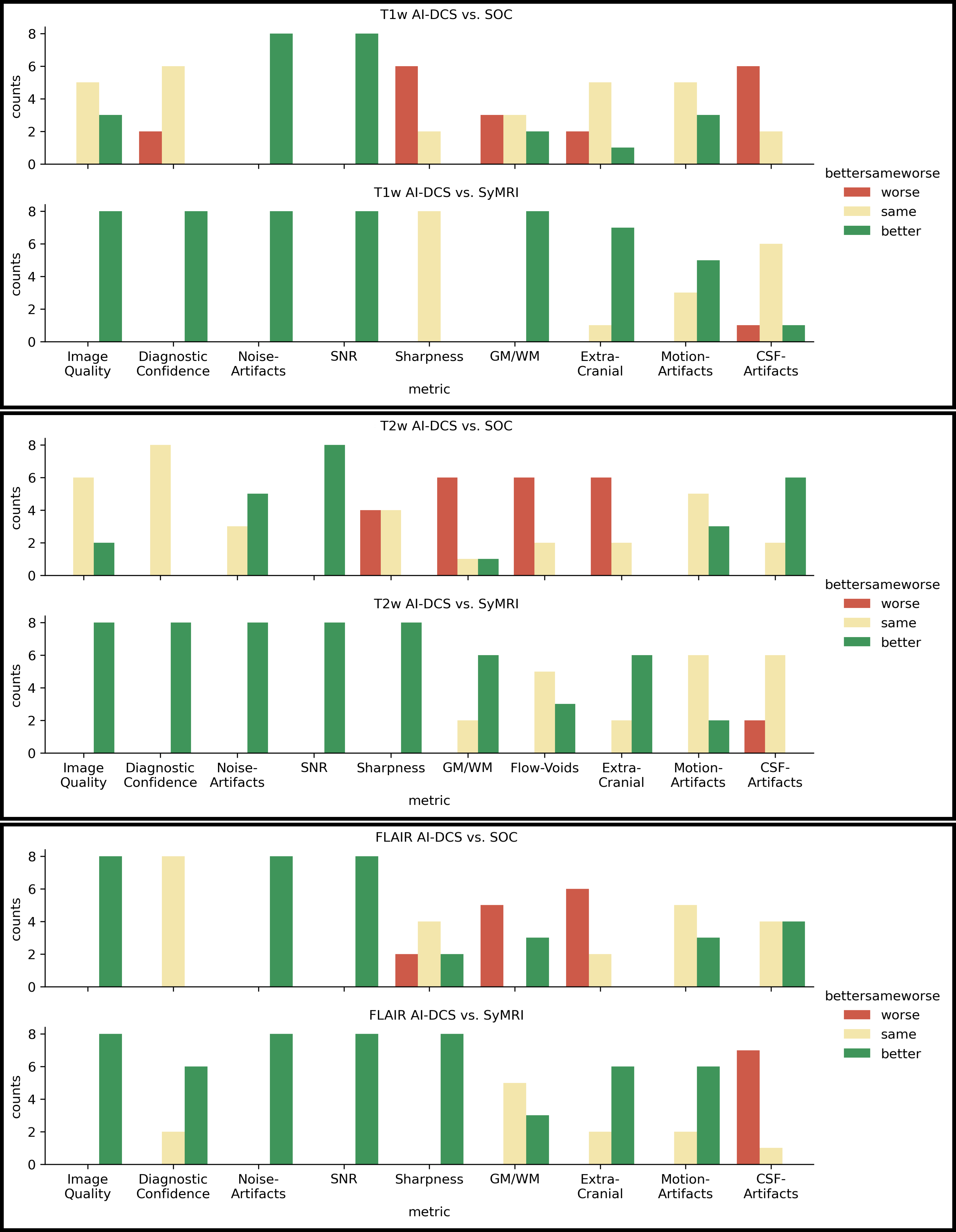
A total of 8 patients were evaluated. Images from a patient example are illustrated in Figure 1. When compared to SyMRI, T1 AI-DCS had better overall image quality, diagnostic confidence, noise/artifacts, and subjective SNR in 100% (8/8) of patients, image sharpness was the same in 100% (8/8) of patients.On T2, overall image quality and diagnostic confidence was better in 100% (8/8) of patients on AI-DCS when compared to SyMRI. When compared to SyMRI, AI-DCS FLAIR was better in 100% (8/8) of patients on overall image quality, noise/artifacts, subjective SNR, and imaging sharpness and was of better diagnostic confidence in 75% (6/8) of patients. On FLAIR, the overall image quality, noise/artifacts, and subjective SNR was better in 100% (8/8) patients when compared to the SOC. These and other findings are summarized in Figure 2, which displays for each category the number of patients which were rated better, same, or worse, respectively.
Conclusions
AI-DCS demonstrates better overall image quality and diagnostic confidence than SyMRI on T1, T2 and FLAIR in the majority of patients. AI-DCS demonstrates the same overall image quality when compared to the SOC on T2 and T1 in the majority of patients and better overall image quality on FLAIR. Further studies are thus warranted to assess the feasibility of using AI-DCS in clinical practice in children.Acknowledgements
No acknowledgement found.References
1. Wang, K et al., “High-fidelity direct contrast synthesis from magnetic resonance fingerprinting”, Magn Reson Med. 2023;90:2116–2129.
2. Warntjes, M et al., “Rapid Magnetic Resonance Quantification on the Brain: Optimization for Clinical Usage”, Magn Reson Med. 60:320 –329 (2008)
3. Wang G, et al, “Synthesize High-Quality Multi-Contrast Magnetic Resonance Imaging From Multi-Echo Acquisition Using Multi-Task Deep Generative Model”, IEEE Trans Med Imaging 39:3089 (2020), 10.1109/TMI.2020.2987026
4. Johnson, J et al., “Perceptual Losses for Real-Time Style Transfer and Super-Resolution”, arXiv:1603.08155v1
Figures