2367
Brain Metabolite Concentrations in Neonates with Congenital Heart Disease Before and After Cardiac Surgery1Developing Brain Institute, Children's National Hospital, Washington, DC, United States, 2Departments of Radiology, The George Washington University School of Medicine and Health Sciences, Washington, DC, United States, 3Departments of Pediatrics, The George Washington University School of Medicine and Health Sciences, Washington, DC, United States, 4Division of Neonatology, Children’s National Hospital, Washington, DC, United States, 5Prenatal Pediatric Institute, Children’s National Hospital, Washington, DC, United States
Synopsis
Keywords: Neonatal, Spectroscopy
Motivation: Alterations in brain metabolism before and after surgical repair of congenital heart disease is not well studied.
Goal(s): To investigate changes in key brain metabolites and primary neurotransmitters before and after cardiac surgery using 1H-MRS.
Approach: Data were acquired in the cerebellum, right basal ganglia and right frontal lobe using MEGA-PRESS in 3T.
Results: Measurements of myo-inositol (mI) in the cerebellum were significantly higher in the preoperative CHD group compared to the healthy controls. γ-Aminobutyric acid (GABA) measurements were significantly higher in the right basal ganglia in the postoperative CHD group compared to the preoperative group.
Impact: Expanded investigation of brain biochemistry in neonates with congenital heart disease has revealed dynamic changes in key metabolites before and after cardiac repair, especially in key neurotransmitters GABA and mI which are known to play important roles in neurodevelopmental disabilities.
Introduction
Critical congenital heart disease is associated with decreased perfusion and oxygenation to the developing brain; early cardiac repair aims to improve systemic (and cerebral) hemodynamics. The purpose of this study was to compare brain metabolite measurements including GABA in healthy controls and neonates with congenital heart disease (CHD) before and after cardiac surgery using 1H-MRS.Methods
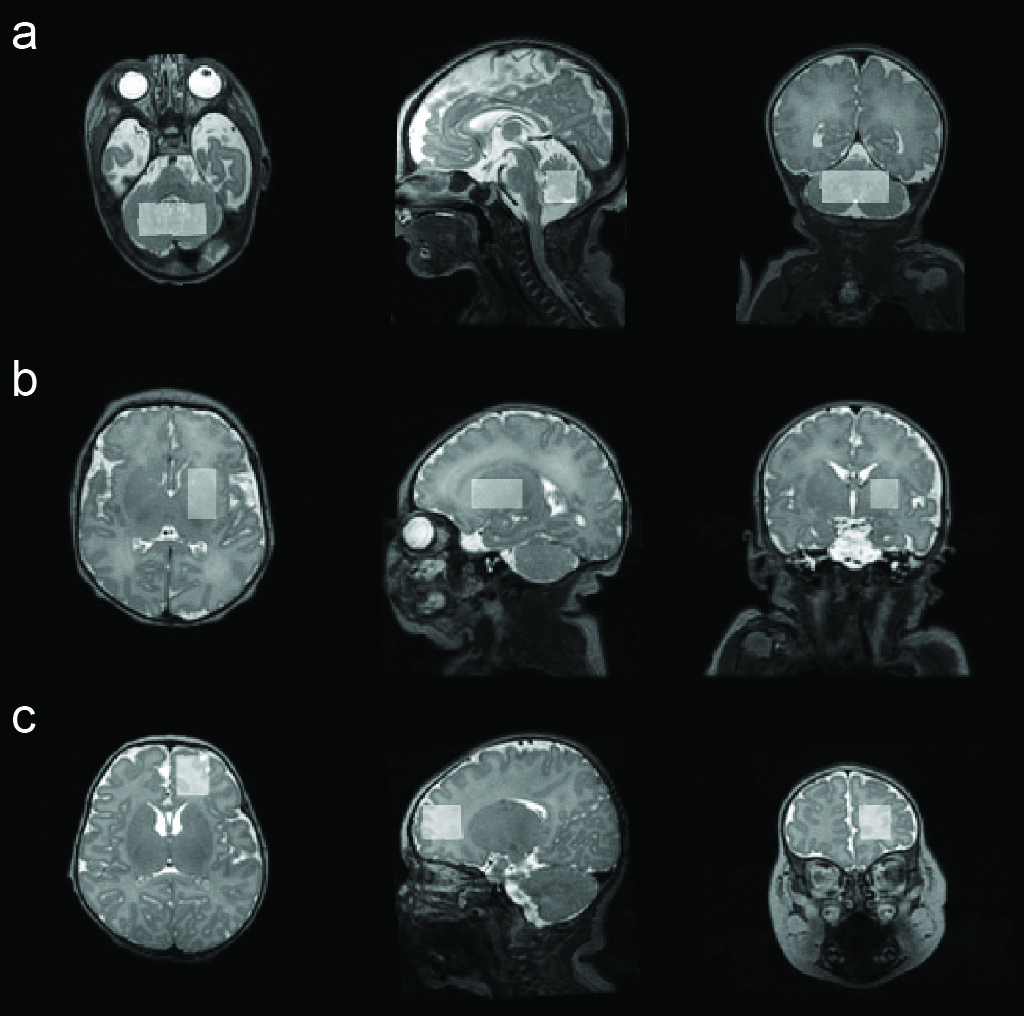
Healthy newborns and neonates with CHD were recruited prospectively. Inclusion criteria comprised neonates diagnosed with complex CHD. Clinical data including weight, postmenstrual age (PMA), sex, lesion type, lesion class, bypass time and survival rate were extracted.MRI scans were performed on a 3T GE scanner (Milwaukee, Wisconsin) using an 8-channel surface receive coil. Anatomic images were acquired using T2-weighted 3D CUBE FSE (thickness=1 mm, TR=2500 ms, TE=64.7–89.9 ms, flip angle=90°, number of slices=120, matrix=160x160). MR spectra were acquired using MEGA-PRESS (1) (TR/TE=2000/68 ms, 256 transients of 4096 datapoints sampled at 5 kHz with VAPOR (2) water suppression). Frequency-selective 16-ms editing pulses were placed at 1.9 and 7.5 ppm during ON and OFF acquisitions. Data were acquired in the middle of the cerebellum (25x15x10 mm3), white matter of the right frontal lobe (20x15x15 mm3) and the right basal ganglia (20x20x20 mm3). Representative voxel locations are shown in Figure 1.
Spectra were processed and modeled using the Osprey software v2.4 (3). The basis set consisted of 18 simulated metabolite basis functions and the cohort-averaged measured mobile macromolecule basis functions (4-6). Brain tissue segmentation was performed using the Osprey-integrated SPM12 (7). Metabolite measurements were water-scaled and tissue-corrected based on literature values (8).
Statistical analyses were performed using R v4.3.1 (9). One-way ANCOVA was performed to compare metabolite measurements among healthy controls, preoperative and postoperative CHD cases. Measurements were adjusted for PMA. Within-subject comparisons were performed using a linear mixed-effects model (LMM), considering time points before and after surgery while adjusting for PMA between preoperative and postoperative measurements. P-values less than 0.05 were considered statistically significant.
Results
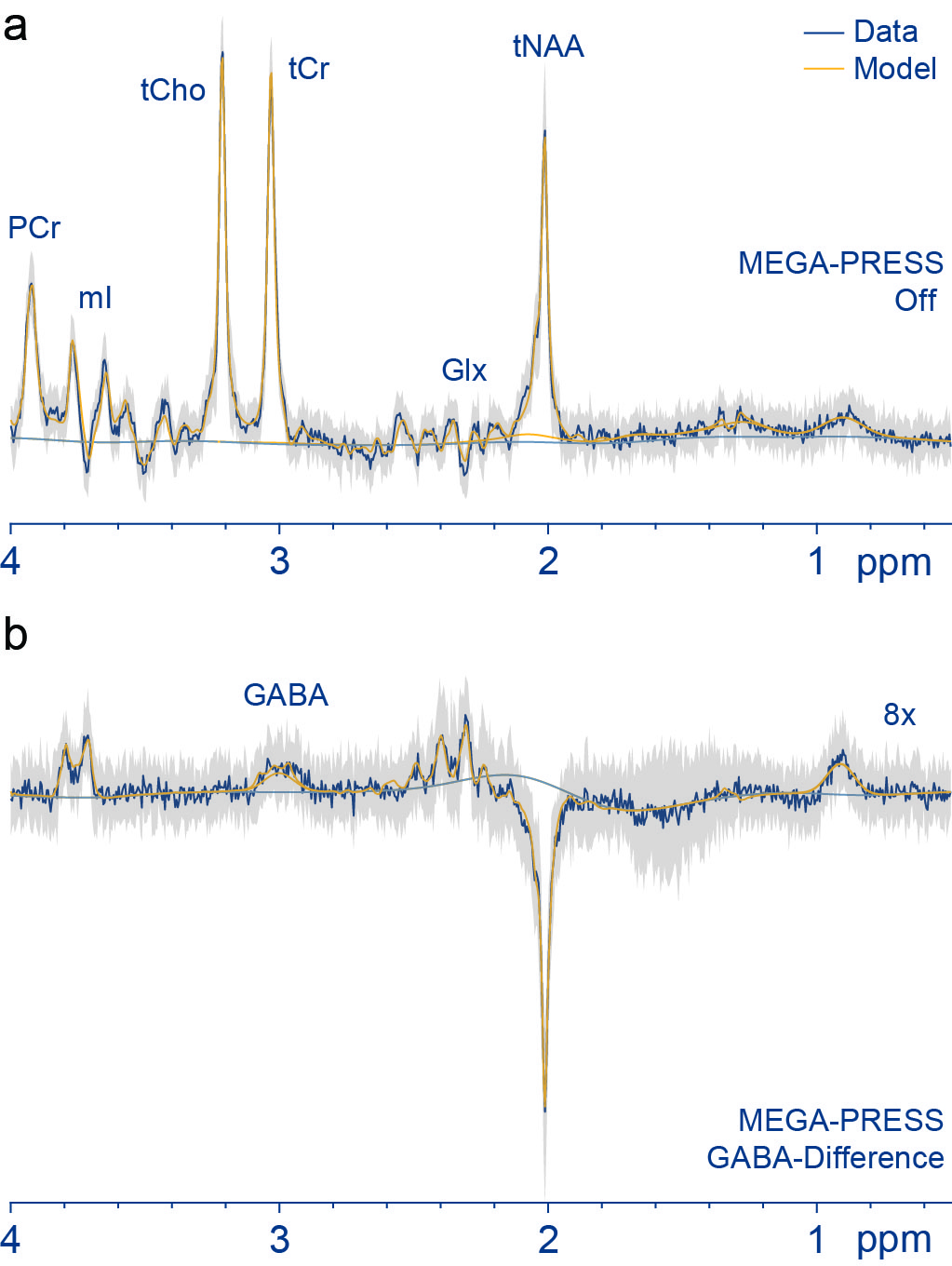
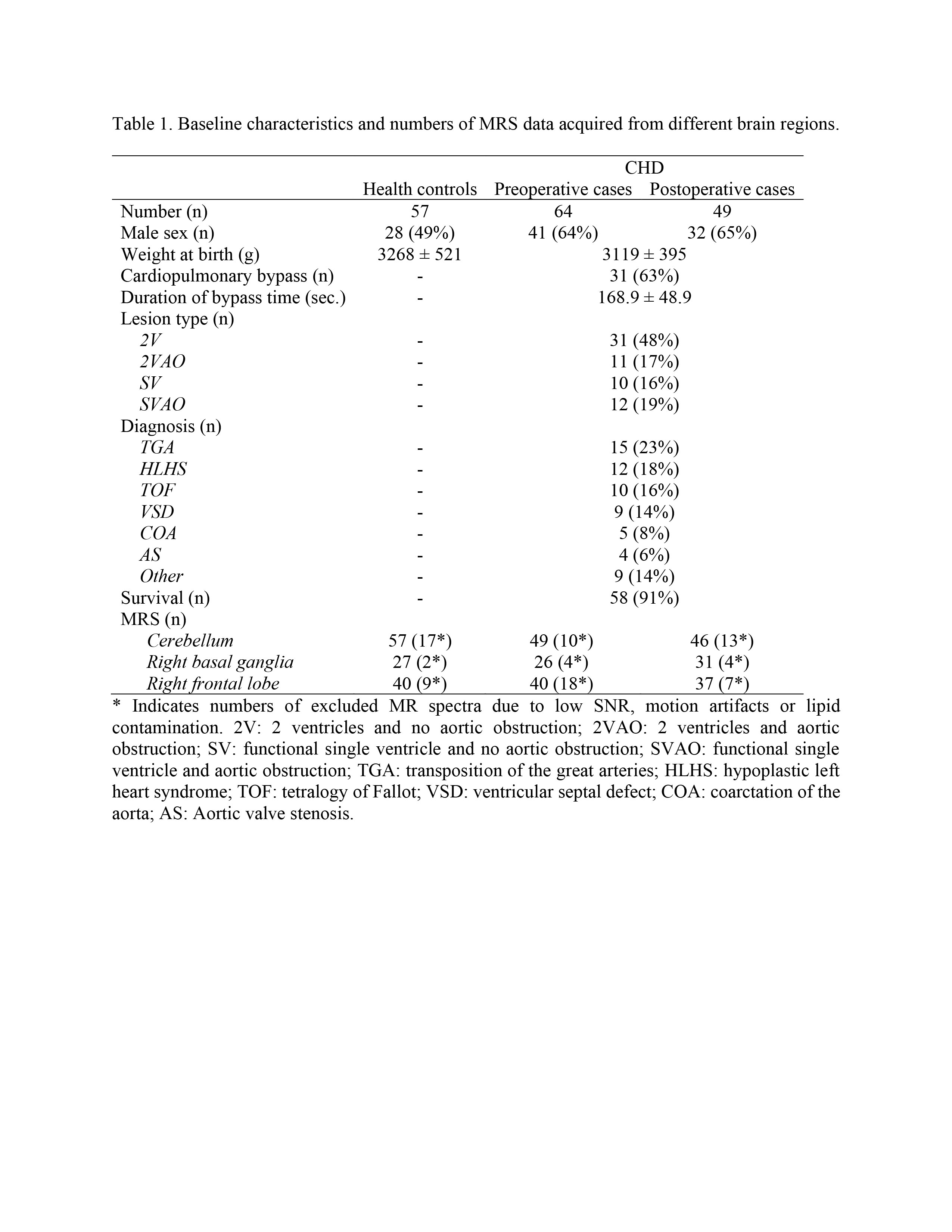
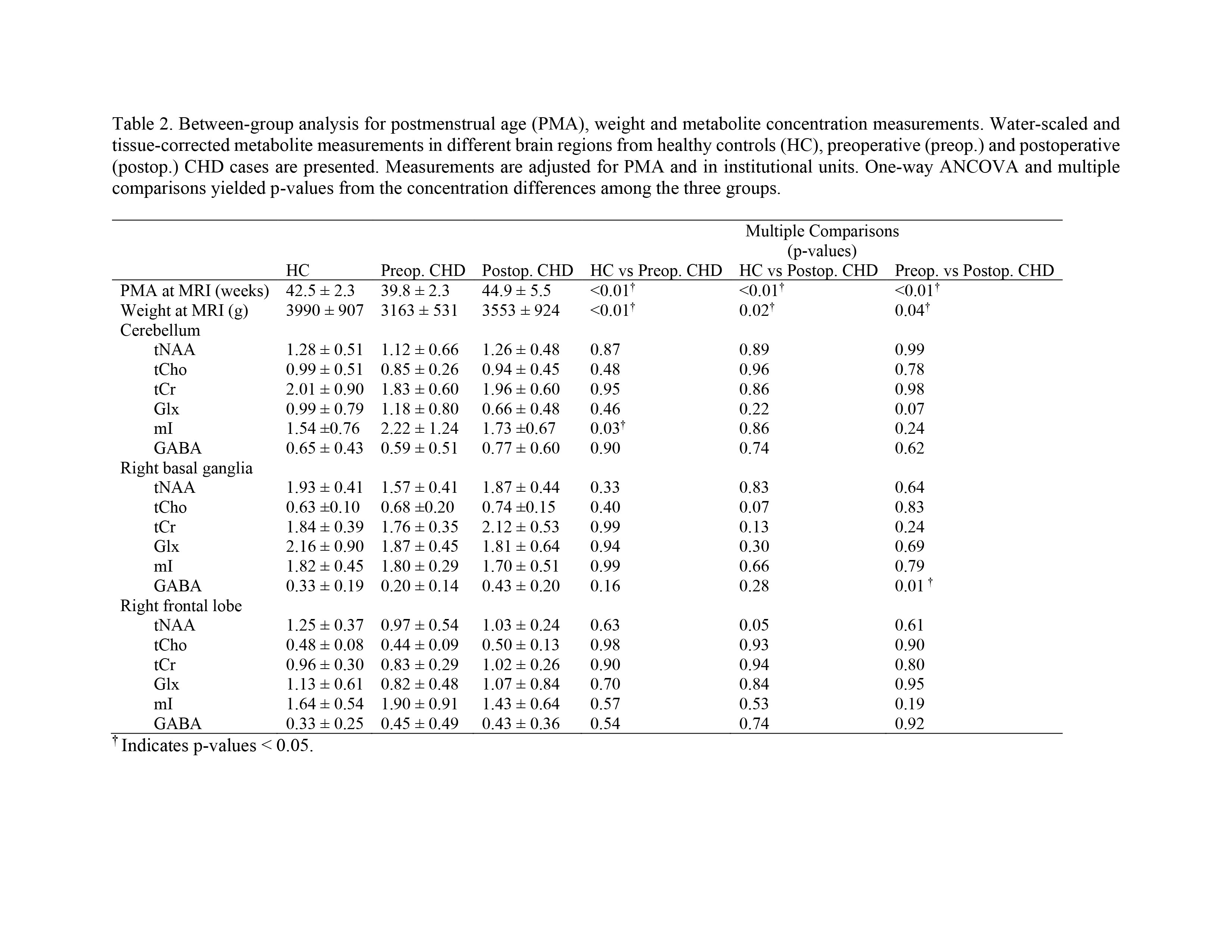
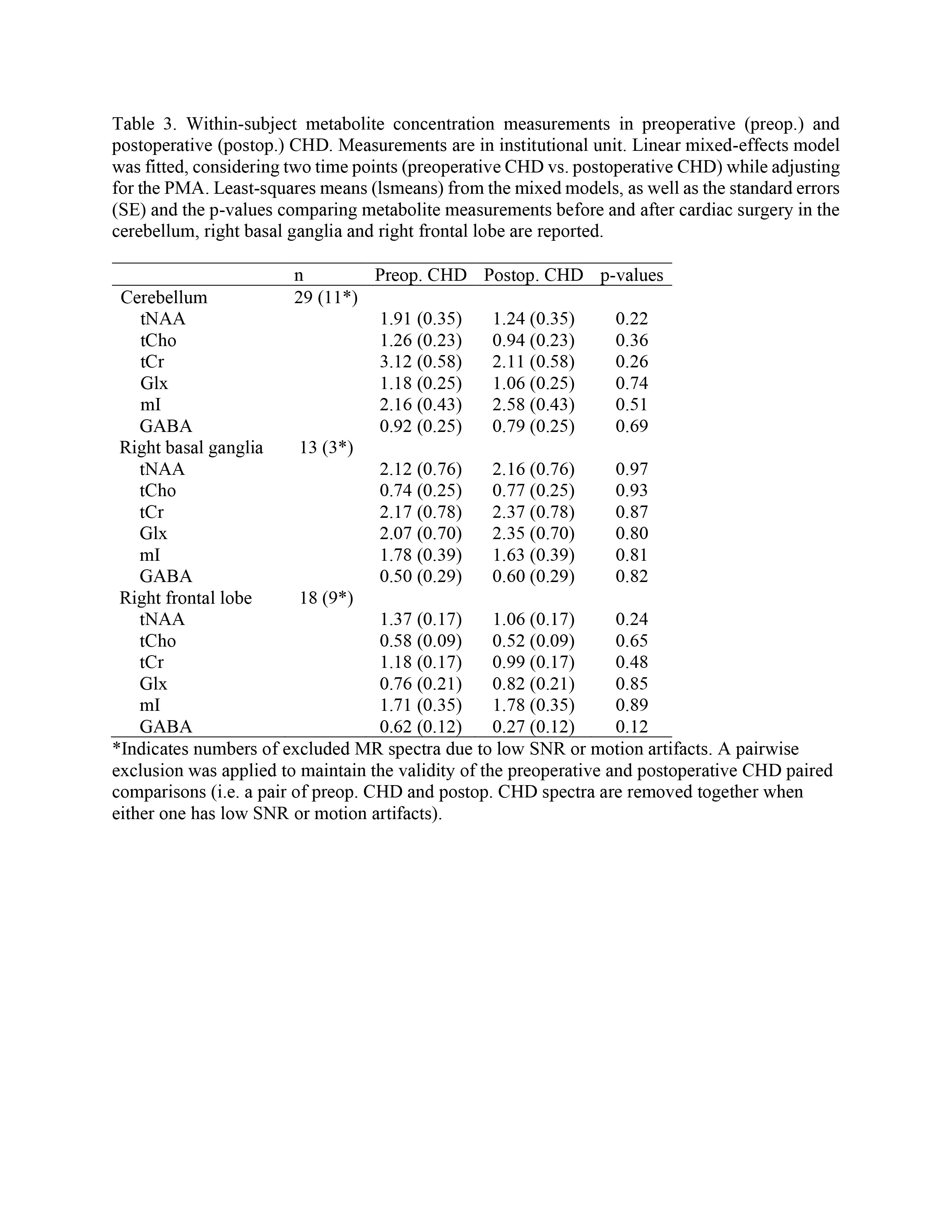
MRI and MRS were successfully obtained from 121 newborns (57 controls and 64 with CHD). Of those, 29 CHD cases underwent both preoperative and postoperative scans. The numbers of spectra successfully acquired from different brain regions varied due to inherent challenges with neonatal scans as indicated in Table 1. Data with excessive motion artifacts and low SNR were excluded. The most common CHD diagnosis was TGA (23%) and in two-ventricle CHD without obstruction (48%). 91% of cases survived after surgery. Representative cohort-mean spectra are shown in Figure 2.One-way ANCOVA and multiple comparisons indicated that metabolite measurement of mI in the cerebellum was significantly higher (p<0.05) in the preoperative CHD cases compared to healthy controls. GABA measurements in the right basal ganglia were significantly higher (p<0.05) in the postoperative cases compared to the preoperative as shown in Table 2. Within subject comparisons, we did not find significant differences in all metabolites of interest after adjusting for PMA as shown in Table 3.
Discussion
In this work, we demonstrate a significant increase in GABA after cardiac repair in neonates with CHD. Previous work has shown that in healthy neonates, GABA concentrations do not vary as a function of age (10). Prior to repair, neonates with CHD had lower GABA concentration compared to healthy controls, though this did not reach statistical significance. Post repair, GABA concentration increased significantly in the right basal ganglia, and may reflect a critical period of neuronal organization and maturation of the neurotransmitter systems resulting from improved cerebral hemodynamics.mI was significantly higher in the preoperative CHD cases compared to the healthy controls in the cerebellum. The reasons for its elevation could be a response to brain injury in the form of astrogliosis (11,12). Emerging evidence suggests that mI can promote recovery from white matter injury caused by chronic neonatal hypoxia as it activates phosphoinositide signaling pathways that promote oligodendrocyte myelination during development and in the setting of white matter injury. We did not detect significant differences in tNAA, tCho, tCr and Glx in all regions of interest, which is mostly in line with similar reports of MR using PRESS (13).
LMM reported no significant differences were found in least-squares means for within-subject comparisons (pre- and postoperatively). However, the statistical power of the within-subject comparisons is weakened due to the number of paired data available – additional studies in larger cohorts are needed to better understand the impact of cardiac repair on cerebral metabolism. To the best of our knowledge, this is the first study to measure GABA with other high concentration metabolites using MEGA-PRESS in neonates with CHD underwent cardiac surgery.
Acknowledgements
This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) grant R01HL116585.References
1. Mescher M, Merkle H, Kirsch J, Garwood M, Gruetter R. Simultaneous in vivo spectral editing and water suppression. NMR Biomed 1998;11(6):266-272.
2. Tkac I, Starcuk Z, Choi IY, Gruetter R. In vivo 1H NMR spectroscopy of rat brain at 1 ms echo time. Magn Reson Med 1999;41(4):649-656.
3. Oeltzschner G, Zollner HJ, Hui SCN, et al. Osprey: Open-source processing, reconstruction & estimation of magnetic resonance spectroscopy data. J Neurosci Methods 2020;343:108827.
4. Zollner HJ, Davies-Jenkins CW, Murali-Manohar S, et al. Feasibility and implications of using subject-specific macromolecular spectra to model short echo time magnetic resonance spectroscopy data. NMR Biomed 2022:e4854.
5. Hui SCN, Gong T, Zollner HJ, et al. The macromolecular MR spectrum does not change with healthy aging. Magn Reson Med 2022;87(4):1711-1719.
6. Tkac I, Oz G, Adriany G, Ugurbil K, Gruetter R. In vivo 1H NMR spectroscopy of the human brain at high magnetic fields: metabolite quantification at 4T vs. 7T. Magnetic resonance in medicine 2009;62(4):868-879.
7. Friston KJ, Holmes AP, Worsley KJ, Poline JP, Frith CD, Frackowiak RSJ. Statistical parametric maps in functional imaging: A general linear approach. Human Brain Mapping 1994;2(4):189-210.
8. Wansapura JP, Holland SK, Dunn RS, Ball WS, Jr. NMR relaxation times in the human brain at 3.0 tesla. J Magn Reson Imaging 1999;9(4):531-538.
9. RStudioTeam. RStudio: Integrated Development for R. RStudio, PBC. Boston, MA; 2020.
10. Basu SK, Pradhan S, Barnett SD, et al. Regional Differences in Gamma-Aminobutyric Acid and Glutamate Concentrations in the Healthy Newborn Brain. AJNR American journal of neuroradiology 2022;43(1):125-131.
11. Harris JL, Choi IY, Brooks WM. Probing astrocyte metabolism in vivo: proton magnetic resonance spectroscopy in the injured and aging brain. Frontiers in aging neuroscience 2015;7:202.
12. Kierans AS, Kirov, II, Gonen O, et al. Myoinositol and glutamate complex neurometabolite abnormality after mild traumatic brain injury. Neurology 2014;82(6):521-528. 13. Steger C, Feldmann M, Borns J, et al. Neurometabolic changes in neonates with congenital heart defects and their relation to neurodevelopmental outcome. Pediatric research 2023;93(6):1642-1650.
Figures