2365
T1-Weighted MP2RAGE Optimisation for Neonates at 7T1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 2London Collaborative Ultra high field System (LoCUS), London, United Kingdom, 3Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 4Guy's and St Thomas’ NHS Foundation Trust, London, United Kingdom, 5MR Research Collaborations, Siemens Healthcare Limited, London, United Kingdom, 6MRC Centre for Neurodevelopmental Disorders, King’s College London, London, United Kingdom
Synopsis
Keywords: Neonatal, Neonatal
Motivation: There is currently no high contrast structural T1-weighted protocol available for neonatal imaging at ultrahigh field (7T), as the longer T1 relaxation times make existing protocols optimized for older subjects unsuitable.
Goal(s): To produce submillimeter T1-weighted images for neonates at 7T in a clinically feasible scan time.
Approach: We optimised a T1-weighted MP2RAGE protocol using the genetic algorithm for constrained optimisation while accounting for transmit field inhomogeneities.
Results: 3D whole-brain images with 0.65-0.8mm isotropic resolution were acquired in under 6-7 minutes from 3 infants. Quantitative T1 maps were produced using an in-house fitting algorithm.
Impact: We describe the first neonatal optimised MP2RAGE protocol for acquiring high-contrast submillimeter-resolution images with full-brain coverage that are relatively insensitive to transmit field inhomogeneities.
Introduction
Ultra-high field enables imaging with increased signal-to-noise ratio and spatial resolution. These attributes are potentially very beneficial for imaging neonates born preterm1 as their brains are undergoing a critical period of development and have smaller brain structures.However, obtaining good T1-weighted contrast on brain images from neonates at 7T is non-trivial due to the combination of the inherently long T1 values of the developing tissue compared to adults1-3 which increases further at higher field strengths4. Furthermore, contrast is inverted in neonatal T1-weighted images5 compared to adult T1-weighted images as myelination is not complete until 2-3 years of age6.
MP2RAGE7 is the most frequently used T1-weighted sequence for structural brain imaging at 7T due to its insensitivity to receive field inhomogeneity, proton density, and T2* effects7. In this study, we aimed to optimise an MP2RAGE protocol for neonates at 7T for obtaining high-resolution and high-contrast images in clinically feasible scan times.
Methods
The MP2RAGE signal expressions7 for steady-state longitudinal magnetization (mz,ss) and the modified GRE signal equations8 for partial Fourier acquisitions of 6/8 in the first phase-encoding (partition) direction (the innermost k-space loop) are given in Eqs.1-3. EA, EB, and EC are time constants related to the acquisition parameters7 and E1=exp(-TRGRE/T1) where TRGRE is the time between consecutive excitations (n in total) and TRMP2RAGE is the time between two inversion pulses. The inversion efficiency is given as eff.$$m_{z,ss}=\frac{M_0\left[\left(\left((1-EA)(cos(α_1)E1)^n+(1-E1)\frac{1-(cos(α_1)E1)^n}{1-cos(α_1)E1}\right)EB+(1-EB)\right)(cos(α_2)E1)^n+(1-E1)\frac{1-(cos(α_2)E1)^n}{1-cos(α_2)E1}\right]EC+(1-EC)M_0}{1+eff(cos(α_1)cos(α_2))^n\hspace{1mm}e^{-MP2RAGETR/T_1}}\hspace{1mm}[1]$$
$$\begin{align}GRE_{TI1}&=M_0\hspace{1mm}B_1^-e^{-TE/T_2^*}sin(α_1)\left[\left(\frac{-eff.m_{z,ss}}{M_0}EA+(1-EA)\right)(cos(α_1)E1)^\frac{n}{3}+(1-E1)\frac{1-(cos(α_1)E1)^\frac{n}{3}}{1-cos(α_1)E1}\right]\hspace{1mm}[2] \\ GRE_{TI2}&=M_0\hspace{1mm}B_1^-e^{-TE/T_2^*}sin(α_2)\left[\frac{\frac{m_{z,ss}}{M_0}-(1-EC)}{EC(cos(α_2)E1)^\frac{2n}{3}}-(1-E1)\frac{(cos(α_2)E1)^\frac{-2n}{3}-1}{1-cos(α_2)E1}\right]\hspace{1mm}[3]\end{align}$$
$$S=\hspace{1mm}\left[\frac{GRE_{TI1}GRE_{TI2}}{{GRE_{TI1}}^2+{GRE_{TI2}}^2}\right]\hspace{1mm}[4]$$
S given above is the MP2RAGE signal (Eqn.4). We optimized sequence parameters while keeping TRGRE at 7.9ms to maximize contrast between white matter (WM) and deep grey matter (DGM) at the nominal B1 value. A relatively short TRMP2RAGE was desired to limit overall scan duration: we found that in this range the MP2RAGE signal can become very B1-sensitive, hence the optimization was also framed to minimize the degree of B1 sensitivity. We used the genetic algorithm (MATLAB, R2022b) to maximize the cost function $$f(x,B_1)=\hspace{1mm}|S(x,B_1,T_{1,WM})-S(x,B_1,T_{1,DGM})|$$ with the optimisation framed as: $$\max_{x}\{f(x,B_1=1)\}$$ subject to: $$ 1)\hspace{2mm}S(x,B_1,T_{1,DGM})-S(x,B_1,T_{1,WM})≥0.12\hspace{2mm}for\hspace{2mm}B_1=0.8:0.1:1.4 $$ $$ 2)\hspace{2mm}S(x,B_1,T_{1,WM})-S(x,B_1,T_{1,CSF})≥0.12\hspace{2mm}for\hspace{2mm}B_1=0.5:0.1:1.4 $$ $$3)\hspace{2mm}S(x,B_1,T_{1,cortex})-S(x,B_1,T_{1,WM})≥0.10\hspace{2mm}for\hspace{2mm}B_1=0.5:0.1:0.8 $$ $$ 4)\hspace{2mm}max\{S(x,B_1=1.4,T_{1,range})-S(x,B_1=0.5,T_{1,range})\}\hspace{2mm}where\hspace{2mm}T_{1,range}=200:200:5000\hspace{1mm} ms $$
Constraints 1-3 avoid solutions resulting in very poor contrast between other tissues across the range of expected B1+ levels. Constraint 4 further aims to limit the degree of B1+ variability over a broad range of T1 values. T1 values of 2477ms/2775ms/2930ms/3800ms for DGM, cortex, WM, and CSF, respectively2 were used in the above expressions. Parameters were constrained to TI1:[300ms 3500ms], TI2:[600ms 4500ms], TRMP2RAGE:[3000ms 5000ms], α1:[3° 15°], α2:[3° 15°].
The optimised protocol was used to acquire data from three preterm infants studied at term equivalent age (2F, postmenstrual age at scan (PMA) 39.7/39.7/38 weeks) in a MAGNETOM Terra 7T system (Siemens Healthcare, Erlangen, Germany) with a 1TX/32RX head coil (Nova Medical) with a locally modified safety model9. Imaging was performed during natural sleep following feeding. Clinical staff observed temperature, heart rate, and oxygen saturation during the scan using a Philips Expression MR400 patient monitor.
Eqs.1-3 were combined to fit T1 using an in-house algorithm8. The eff was assumed to be 1 for the hyperbolic secant10-11 adiabatic inversion. B1+ maps12 registered to the MP2RAGE images using FLIRT were used in the fitting process13-15.
T1 maps were segmented using an in-house 3D deep learning BOUNTI segmentation pipeline with 17 brain tissue labels16 optimised for T2-weighted neonatal MRI. Segmentation provided ROIs for reporting tissue averaged T1 values.
Results
The optimized protocol had scan parameters: TRGRE/TI1/TI2/TRMP2RAGE=7.9ms/1270ms/2770ms/5000ms; α1/α2=4°/3°; GRAPPA18 factor=3; slice partial Fourier=6/8 which resulted in images with 0.8mm isotropic resolution with full brain coverage in 5:54 min:s. Additional images were acquired with 0.65mm isotropic resolution in one neonate (6:44 min:s). The MP2RAGE images, T1 maps produced by the fitting algorithm, and the segmentations are given in Figs.1-3, respectively. Table 1 shows the quantitative results.Discussion and Conclusion
In this study, T1-weighted MP2RAGE images were optimised for the first time for neonatal MRI at 7T producing 3D whole-brain images with submillimeter-resolution in under 6 minutes. The T1-weighted images (Fig 1) show strong T1 contrast and low B1 inhomogeneity. Figure 4 shows T1-weighted and T2-weighted (TSE) images from the same infant for comparison; features such as the early myelinating structures in the corticospinal tract are more visible on the T1-weighted image as expected. T1 values for neonates 1&2 (twins) are similar and slightly shorter than for neonate 3 – this is expected since neonate 3 was around 2 weeks younger at time of scan2 - though the T1 values are generally slightly longer compared to those obtained with a single-shot TSE sequence2. Future work will explore these acquisitions' sensitivity for identifying pathology and incorporate motion correction methods.Acknowledgements
The authors would like to acknowledge Tobias C. Wood for valuable discussions.
The work was supported by a project grant awarded by Action Medical Research [GN2728], an MRC Clinician Scientist Fellowship [MR/P008712/1], an MRC Transition Support Award [MR/V036874/1], the KCL MRC Centre for Neurodevelopmental Disorders [MR/N026063/1], Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z], Great Ormond Street Hospital Children's Charity (GOSHCC) Sparks Grant V4419, by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and/or the NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
References
1) Annink KV, van der Aa NE, Dudink J, et al. Introduction of Ultra-High-Field MR Imaging in Infants: Preparations and Feasibility. AJNR Am J Neuroradiol 2020;41:1532-1537.
2) Malik SJ. T1 and T2 measurements from Neonates at 7T. In Proceedings of the Annual Meeting of ISMRM. 2023. Abstract 5653.
3) Bridgen, P., Tomi-Tricot, R., Uus, A., Cromb, D., Quirke, M., Almalbis, J., ... & Arichi, T. (2023). Exploration of the potential of high resolution and contrast 7 Tesla MR brain imaging in neonates. medRxiv, 2023-09.
4) Rooney WD, Johnson G, Li X, et al. Magnetic field and tissue dependencies of human brain longitudinal H2O relaxation in vivo. Magn Reson Med. 2007; 57: 308-318.
5) Saunders, D. E., Thompson, C., Gunny, R., Jones, R., Cox, T., & Chong, W. K. (2007). Magnetic resonance imaging protocols for paediatric neuroradiology. Pediatric radiology, 37, 789-797.
6) Barkovich, A. J. (2000). Concepts of myelin and myelination in neuroradiology. American Journal of Neuroradiology, 21(6), 1099-1109.
7) Marques JP, Kober T, Krueger G, van der Zwaag W, Van de Moortele PF, Gruetter R. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. Neuroimage. 2010;49:1271-1281.
8) Dokumaci AS. Evaluation of quantitative T1 and PD mapping at 7T from an MP2RAGE sequence optimised to obtain UNI and FLAWS contrast images in a single scan. In Proceedings of the Joint Annual Meeting of ISMRM-ESMRMB. 2022. Abstract 1244.
9) Malik, S. J., Hand, J. W., Satnarine, R., Price, A. N., & Hajnal, J. V. (2021). Specific absorption rate and temperature in neonate models resulting from exposure to a 7T head coil. Magnetic resonance in medicine, 86(3), 1299-1313.
10) Silver MS, Joseph RI, Hoult DI. Highly selective π/2 and π pulse generation. J Magn Reson. 1984;59:347-351.
11) Baum J, Tycko R,Pines A. Broadband and adiabatic inversion of a two-level system by phase-modulated pulses. Phys Rev A. 1985;32:3435.
12) Yarnykh VL. Actual flip‐angle imaging in the pulsed steady state: a method for rapid three‐dimensional mapping of the transmitted radiofrequency field. Magn Reson Med. 2007;57.1:192-200.
13) Jenkinson, M., Bannister, P., Brady, J. M. and Smith, S. M. Improved Optimisation for the Robust and Accurate Linear Registration and Motion Correction of Brain Images. NeuroImage, 17(2), 825-841, 2002.
14) Jenkinson, M. and Smith, S. M. A Global Optimisation Method for Robust Affine Registration of Brain Images. Medical Image Analysis, 5(2), 143-156, 2001.
15) Greve, D.N. and Fischl, B. Accurate and robust brain image alignment using boundary-based registration. NeuroImage, 48(1):63-72, 2009.
16) Uus Alena U., Kyriakopoulou Vanessa, Makropoulos Antonios, Fukami-Gartner Abi, Cromb Daniel, Davidson Alice, Cordero-Grande Lucilio, Price Anthony N., Grigorescu Irina, Williams Logan Z. J., Robinson Emma C., Lloyd David, Pushparajah Kuberan, Story Lisa, Hutter Jana, Counsell Serena J., Edwards A. David, Rutherford Mary A., Hajnal Joseph V., Deprez Maria (2023) BOUNTI: Brain vOlumetry and aUtomated parcellatioN for 3D feTal MRI eLife 12:RP88818.
17) Paul A. Yushkevich, Joseph Piven, Heather Cody Hazlett, Rachel Gimpel Smith, Sean Ho, James C. Gee, and Guido Gerig. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006 Jul 1; 31(3):1116-28.
18) Griswold MA, Jakob PM, Heidemann RM, et al. Generalized Autocalibrating Partially Parallel Acquisitions (GRAPPA). Magn Reason Med. 2002;47:1202-1210.
19) Kuklisova-Murgasova, M., Quaghebeur, G., Rutherford, M. A., Hajnal, J. V., & Schnabel, J. A. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Medical image analysis. 2012;16(8):1550-1564.
Figures
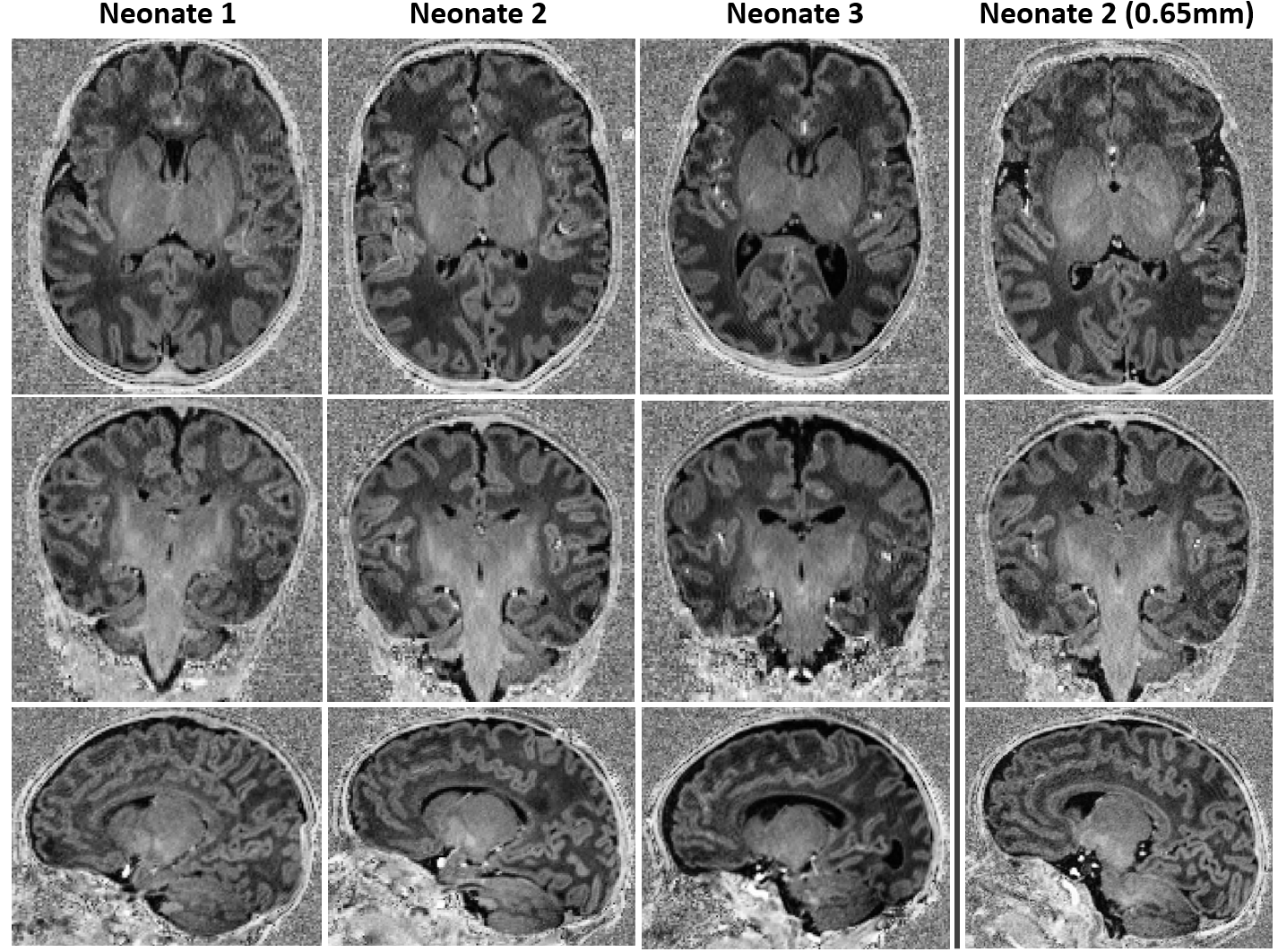
Figure 1. Optimised protocol with 0.8 mm isotropic resolution in 3 different preterm infants. Additionally, images with 0.65 mm isotropic resolution were acquired from neonate 2 using the optimised protocol. The protocols are very similar to each other with most of the parameters being the same except TI2 (2770 ms vs 2760 ms) and TRGRE (7.9 ms vs 8 ms) due to constraints on the scanner. 0.65 mm isotropic resolution led to lower SNR. The FOV was slightly larger for the neonate 3 which led to a TRGRE value of 8 ms to have the same inversion times as those in neonates 1 and 2.
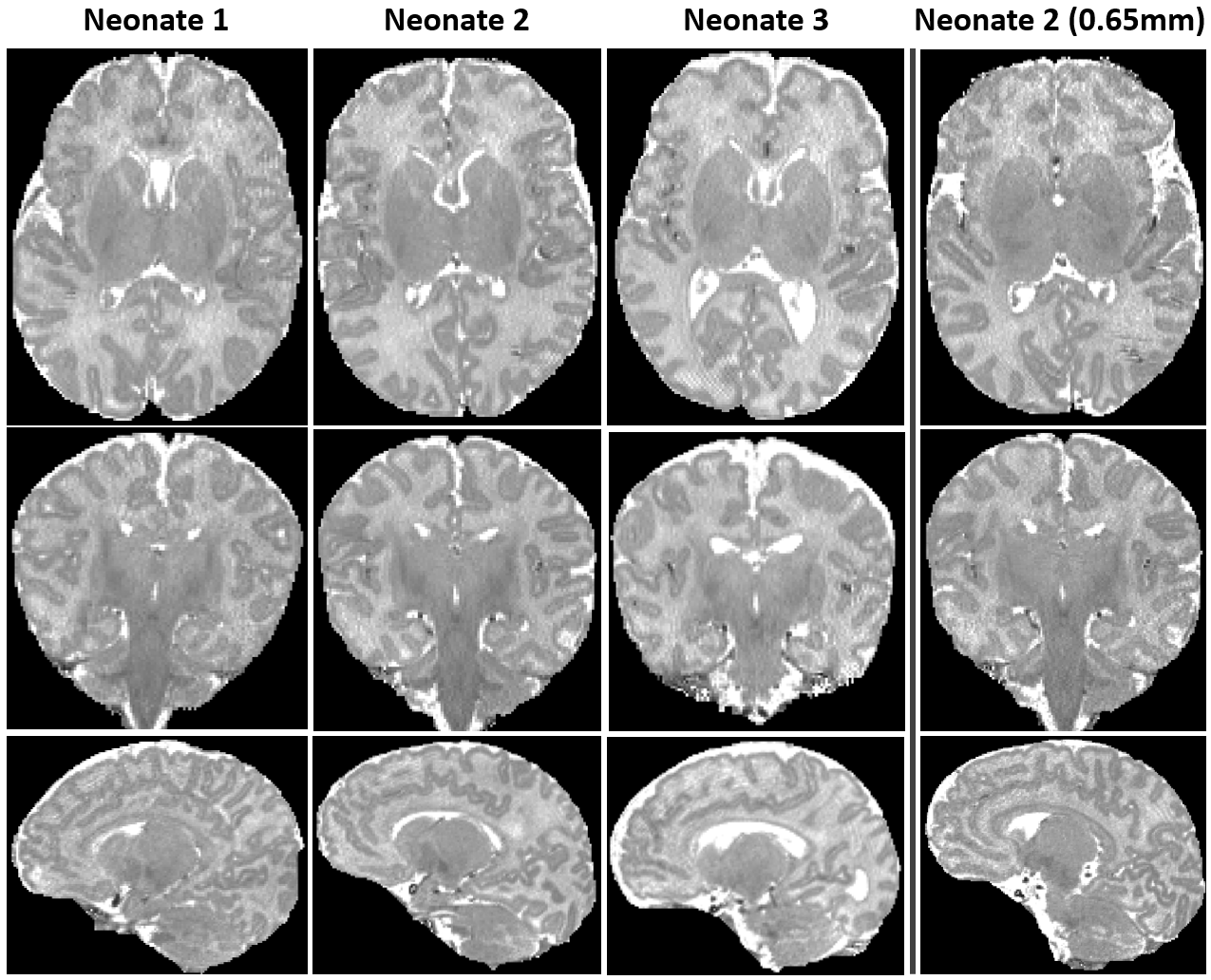
Figure 2. Quantitative T1 maps obtained via a dedicated fitting algorithm8 corresponding to the images in Fig. 1. All maps are displayed in [0 4095] ms range. The low SNR of the images with 0.65 mm isotropic resolution (Fig. 1 rightmost column) affects the quality of the T1 maps as well.
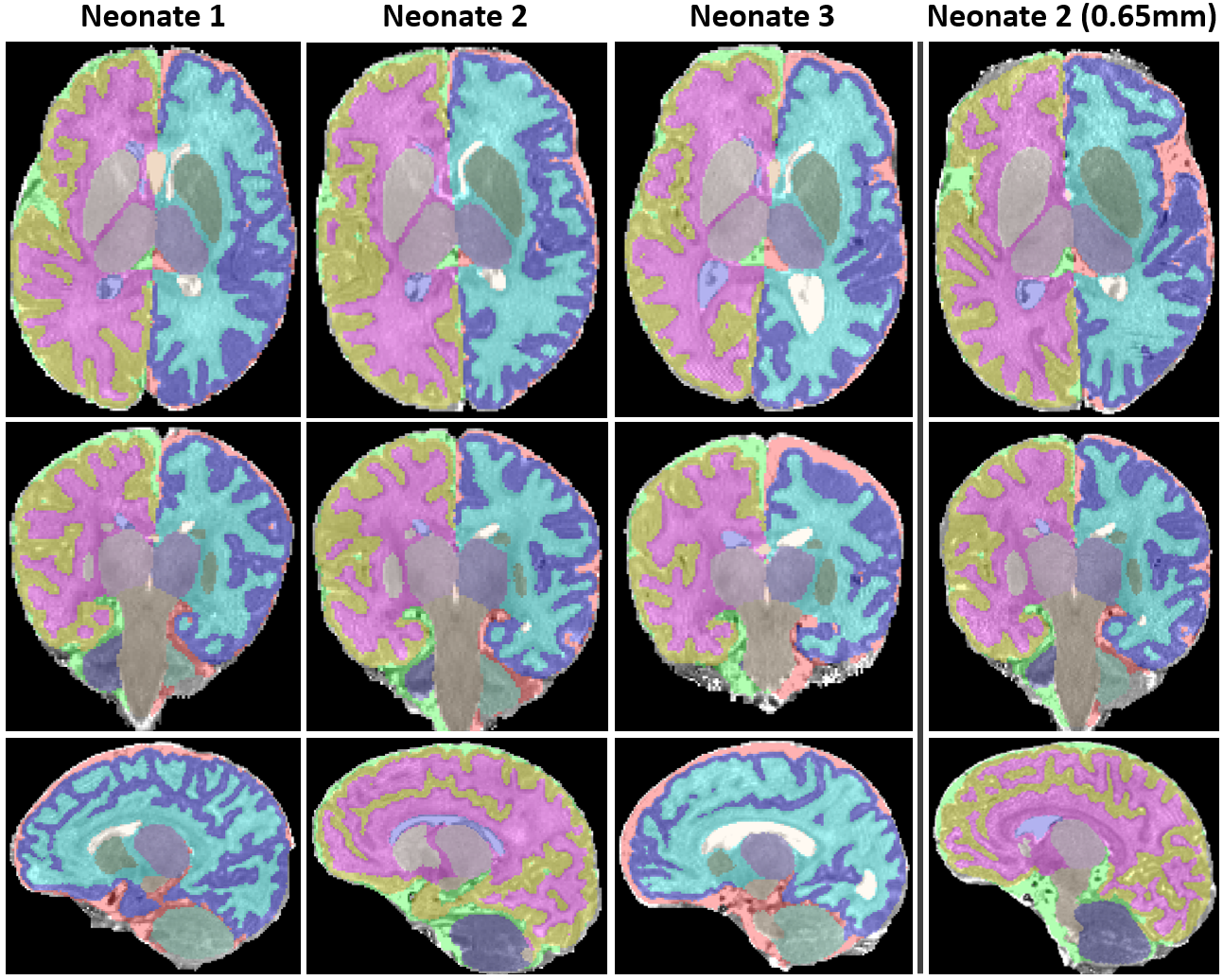
Figure 3. Segmentations of the quantitative T1 maps in Fig. 2 using an in-house 3D deep learning segmentation pipeline16 optimised for T2-weighted neonatal MR images.

Table 1. T1 means ± standard deviations (ms) of the segmented regions across the whole 3D quantitative volume in 3 preterm infants for whom exemplary single slice images were demonstrated in Figs. 1-3. Neonates 1 and 2 are twins (female) and their T1 values are closer to each other compared to those of neonate 3 (male) and shorter in line with the expected decrease in age2.
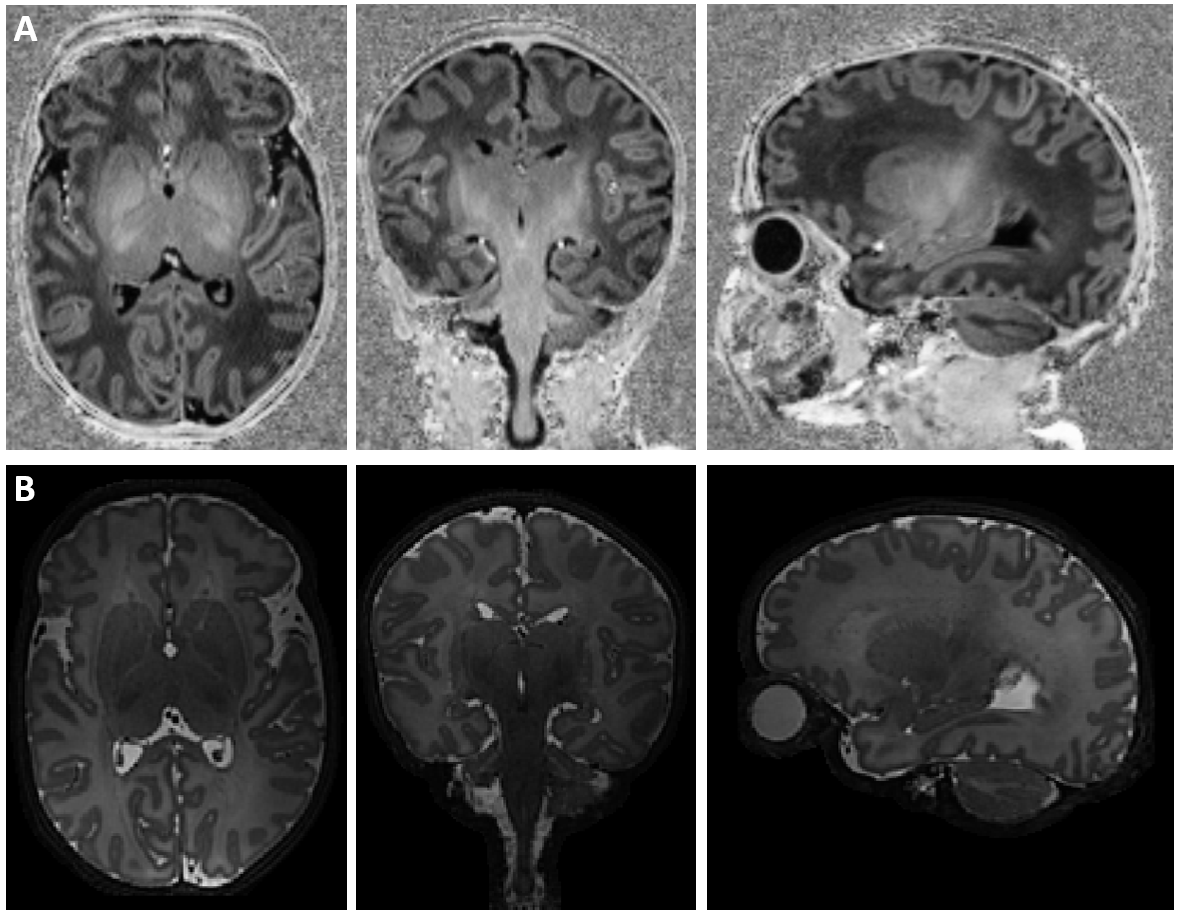
Figure 4. Optimised T1-weighted MP2RAGE image compared with T2-weighted TSE scan in the same neonate (number 2). T2-weighted TSE images of different orientations were combined into a single volume with 0.45 mm isotropic resolution using Slice to Volume Reconstruction19 as implemented in SVRTK (https://svrtk.github.io).