2364
Detecting silent lesions in hypoxic-ischemic encephalopathy using submillimeter isotropic resolution diffusion MRI1Department of Electronic Engineering, Tsinghua University, Beijing, China, 2Department of Radiology, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, China, 3Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, China
Synopsis
Keywords: Fetal, Brain
Motivation: MRI is crucial for the diagnosis and prognosis of hypoxic-ischemic encephalopathy (HIE). High-resolution imaging benefits the detection of subtle lesions. However, neonates may not tolerate lengthy scans .
Goal(s): To obtain ultrahigh resolution brain diffusion-weighted MR images(DWIs) within a feasible time frame to detect lesions invisible on images acquired using standard clinical protocols.
Approach: One b=0 volume and six DWI volumes at submillimeter isotropic resolution (0.86×0.86×0.86 mm3) were acquired using the Generalized SLIce Dithered Enhanced Resolution Simultaneous MultiSlice (gSlider-SMS) sequence, in addition to standard protocols.
Results: Ischemic lesions and cytotoxic edema invisible on standard clinical images were found on submillimeter resolution diffusion MRI data.
Impact: Submillimeter isotropic resolution diffusion MR images show lesions invisible on standard clinical images, which helps diagnose HIE earlier and more accurately for timely and appropriate treatment, as well as provides new biomarkers for accurate HIE staging.
Introduction
Hypoxic-ischemic encephalopathy (HIE) is a type of brain injury that occurs in newborns due to inadequate oxygen supply during the perinatal period. The incidence of HIE is reported to be 4.5 per 1000 live births in developed countries, while exceeds 25.0 per 1000 live births in developing countries1. It is estimated that 15% to 20% of infants with HIE die during the newborn period and 25% of survivors suffer from neurological disabilities2. HIE diagnosis based on clinical manifestations requires a considerable amount of time for observation. Unfortunately, neonatal conditions can deteriorate rapidly, necessitating the use of MRI as a fundamental tool for early and accurate diagnosis3,4. Furthermore, MRI serves as a surrogate biomarker for neurodevelopmental evaluation, aiding in the prognosis following interventions for HIE such as hypothermia5.Previous studies suggest that T2-weighted images are effective in identifying non-punctate white matter lesions6. Diffusion-weighted MR images (DWIs) also show sensitivity to early-phase ischemic changes in the brain7. Nonetheless, subtle lesions are often missed due to the low spatial resolution of MR images, a practical choice due to limited scan time.
To address this challenge, we adopted a new Generalized SLIce Dithered Enhanced Resolution Simultaneous MultiSlice (gSlider-SMS) sequence8,9 to obtain submillimeter isotropic resolution diffusion MRI data. Specifically, one b=0 T2-weighted image volume and DWIs along six diffusion-encoding that provide detailed information regarding the extent of brain damage were acquired within a reasonable time frame. Ultrahigh resolution gSlider-SMS images unveiled numerous ischemic lesions and potential cytotoxic edema that were imperceptible using standard imaging methods.
Methods
Data acquisition. Five patients (Table 1) with HIE were scanned using gSlider-SMS sequence, in addition to standard clinical sequences on a Siemens MAGNETOM Skyra 3.0 T MRI scanner at West China Second University Hospital, equipped with an 18-channel phased-array coil, with approval from the IRB of Sichuan University and written consent forms from their legal guardians. Images were acquired using:(1) 2D T2-weighted turbo spin echo (TSE) sequence (TR/TE=5110/108 ms, 0.44×0.44 mm2 in-plane resolution);
(2) 2D T2-weighted FLAIR TSE sequence (TR/TE=2020/11 ms, inversion time=2600ms, 0.66×0.66 mm2 in-plane resolution);
(3) 2D diffusion-weighted EPI (TR/TE=5660/78 ms, 1.125×1.125 mm2 in-plane resolution, b=1000 s/mm2);
(4) gSlider-SMS sequence (TR/TE = 4300/92ms, 0.86×0.86×0.86 mm3 resolution, b=1000 s/mm2, 5 RF excitations, 4.3 mm section thickness, one b=0 and six DWI volumes, B1 map for RF calibration, ~4 minutes acquisition time).
For 2D imaging, section thickness ranged between 4 to 5 mm without gap.
Data processing. gSlider-SMS technology excited slabs of 5× desired high-resolution image thickness. Each slab was excited five times, using five different RF pulses, which were corrected for B1 inhomogeneity using a separately acquired B1 map. Thin image slices were computed from the five thick-slice slabs by solving a linear equation with Tikhonov regularization. The reconstructed high-resolution b=0 and six DWI volumes were preprocessed using FSL’s “eddy_correct”10 for eddy current correction and image co-registration.
Results
High-resolution b=0 and DWI volumes at 0.86 mm isotropic resolution were successfully reconstructed (Fig. 1v, vi). A significant number of ischemic lesions which were invisible on standard thick-slice images were detected in four patients (Fig. 1 magenta arrowheads): in the cerebellar hemisphere and cerebellar peduncle (Fig. 1A), near the posterior horn of the lateral ventricle (Fig. 1B), in the temporal lobe (Fig. 1C) and beneath the ependyma (Fig. 1D, slice 1).Moreover, high signals were seen on the standard DWI (Fig. 1C, iii) and gSlider-SMS DWI (Fig. 1C, vi) diffusively in the white matter of patient C, indicating potential cytotoxic edema and lactic acid accumulation. For patient D (slice 2), these high signals can be only observed in the parietal lobe on gSlider-SMS DWI (Fig. 1D, Slice 2, vi) but not on the standard DWI (Fig. 1D, Slice 2, iii).
Finally, the gSlider-SMS submillimeter DWI showed microscopic hemorrhage lesion in patient A (Fig. 2 magenta arrowheads). The small lesion was not clearly visible on standard thick-slice images.
Discussion and Conclusion
Small ischemic lesions, microscopic hemorrhages, potential cytotoxic edema and lactic acid accumulation can be overlooked on thick-slice clinical images, which might lead to inaccurate diagnosis in the early phase of HIE. The detection of these small lesions is useful for initiating rehabilitation and assessing prognosis. The imaging time of gSlider-SMS is currently ~4 minutes and ~5 minutes with manual shimming, which can be reduced by only acquiring three DWIs and/or using a lower b-value. The novel ultrahigh resolution imaging method might transform the diagnosis of HIE and substantially improves its treatment.Acknowledgements
No acknowledgement found.References
1. Kurinczuk, J. J., White-Koning, M. & Badawi, N. Epidemiology of neonatal encephalopathy and hypoxic–ischaemic encephalopathy. Early Human Development 86, 329–338 (2010).2. Vannucci, R. C. & Perlman, J. M. Interventions for perinatal hypoxic–ischemic encephalopathy. Pediatrics 100, 1004–1114 (1997).
3. Lv, H. et al. Neonatal hypoxic ischemic encephalopathy-related biomarkers in serum and cerebrospinal fluid. Clinica Chimica Acta 450, 282–297 (2015).
4. Li, L. et al. The Use of Fuzzy BackPropagation Neural Networks for the Early Diagnosis of Hypoxic Ischemic Encephalopathy in Newborns. Journal of Biomedicine and Biotechnology 2011, 349490 (2011).
5. Rollins, N. et al. Predictive value of neonatal MRI showing no or minor degrees of brain injury after hypothermia. Pediatric neurology 50, 447–451 (2014).
6. Liauw, L. et al. Hypoxic-ischemic encephalopathy: diagnostic value of conventional MR imaging pulse sequences in term-born neonates. Radiology 247, 204–212 (2008).
7. Dag, Y. et al. Clinical outcomes of neonatal hypoxic ischemic encephalopathy evaluated with diffusion-weighted magnetic resonance imaging. Diagnostic and Interventional Radiology 12, 109 (2006).
8. Setsompop, K. et al. High‐resolution in vivo diffusion imaging of the human brain with generalized slice dithered enhanced resolution: Simultaneous multislice (g S lider‐SMS). Magnetic resonance in medicine 79, 141–151 (2018).
9. Liao, C. et al. Phase-matched virtual coil reconstruction for highly accelerated diffusion echo-planar imaging. NeuroImage 194, 291–302 (2019).
10. Smith, S. M. et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23, S208–S219 (2004).
Figures
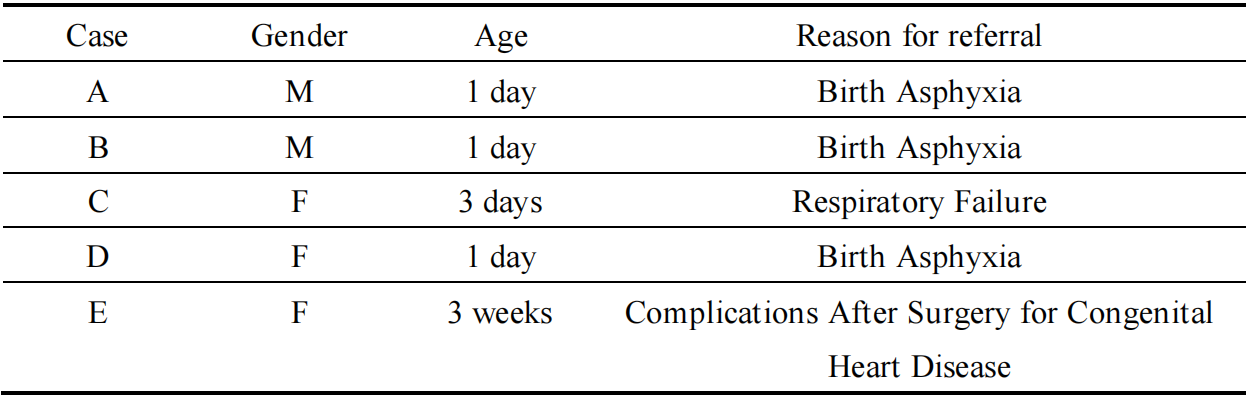
Table 1. Demographic information.
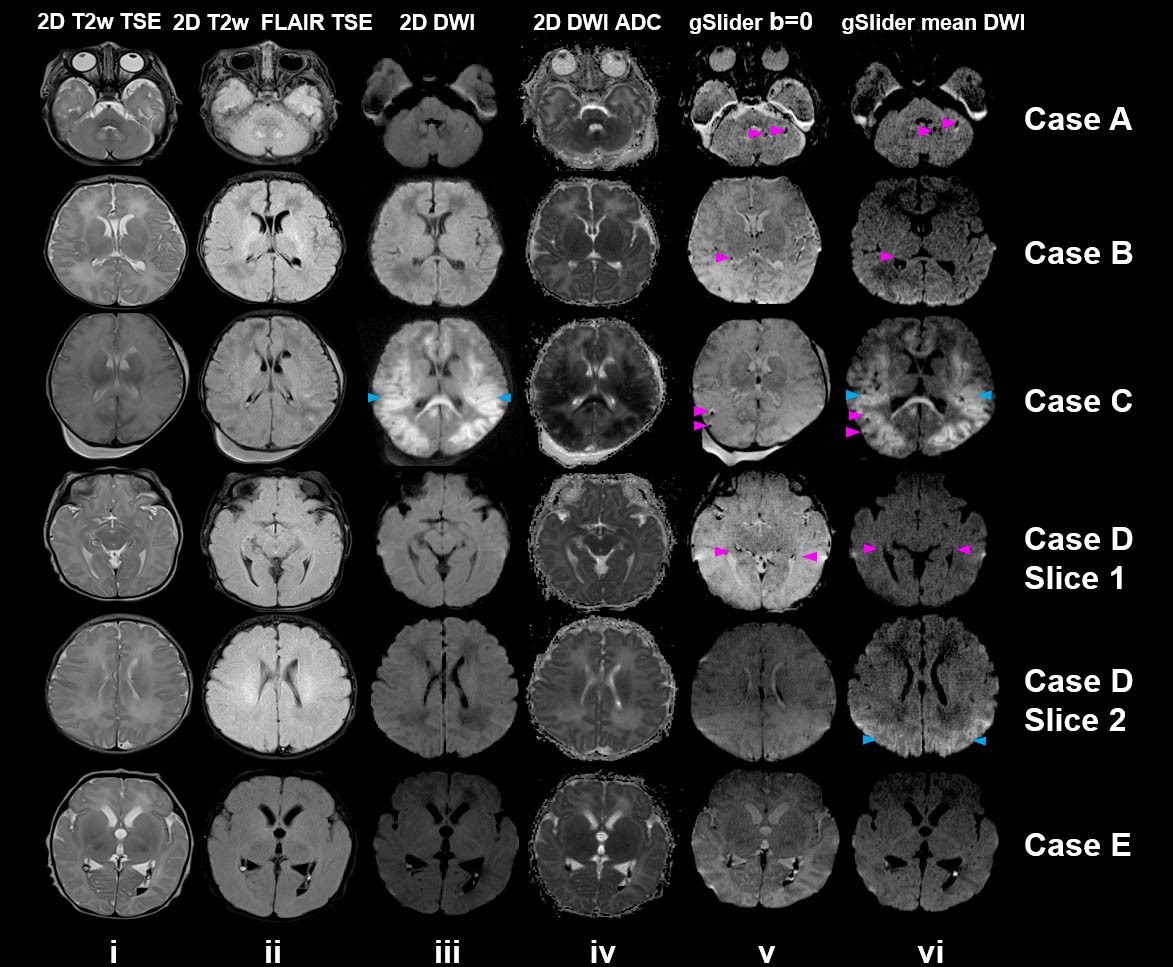
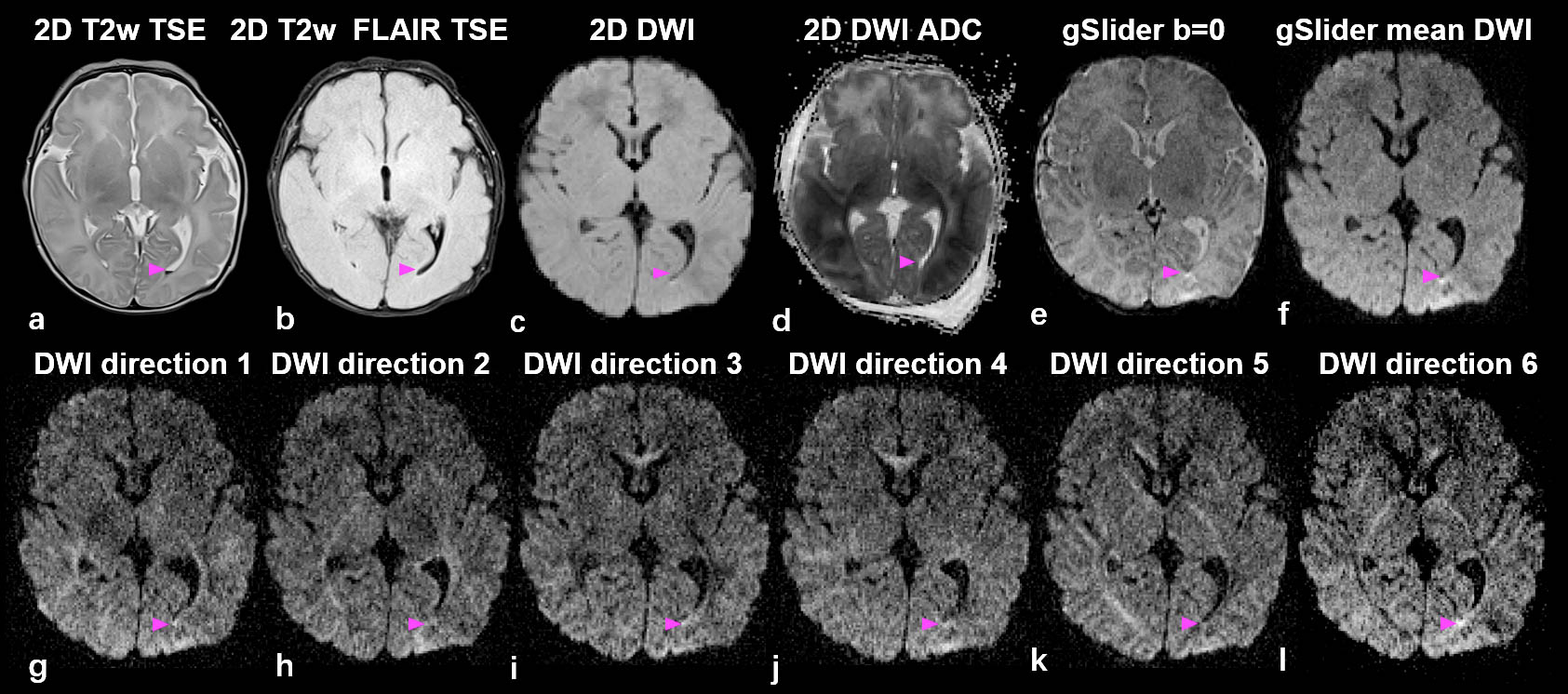
Figure 2. Microscopic hemorrhages. Images acquired using (a) 2D T2-weighted TSE, (b) 2D T2-weighted FLAIR TSE, (c) 2D diffusion-weighted EPI, along with (d) the derived apparent diffusion coefficient (ADC) map, and (e-l) g-Slider sequences are displayed. The magenta arrowheads highlight the location for microscopic hemorrhage near posterior horn of the lateral ventricle.