2359
Reduced cerebral oxygen extraction and metabolic rate in newborns with hypoxic ischemic encephalopathy1Department of Radiology, Johns Hopkins School of Medicine, Baltimore, MD, United States, 2Department of Pediatrics, Johns Hopkins School of Medicine, Baltimore, MD, United States, 3Department of Biomedical Engineering, Johns Hopkins School of Medicine, Baltimore, MD, United States, 4Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 5Department of Pediatrics, University of Maryland School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: Neonatal, Oxygenation
Motivation: Over 40% of neonates with moderate or severe hypoxic-ischemic-encephalopathy (HIE) still suffer from death, disability or neurodevelopmental delay after standard hypothermia treatment. Assessment of the brain’s oxygen metabolism may provide useful biomarkers to identify the risk of permanent neurologic injury and determine the necessity of adjuvant treatments.
Goal(s): To evaluate cerebral oxygen-extraction-fraction (OEF) and cerebral-metabolic-rate-of-oxygen (CMRO2) in neonates with HIE in comparison with healthy newborns.
Approach: We measured OEF and CMRO2 in 42 neonates with HIE and 52 healthy newborns.
Results: Neonates with HIE exhibited diminished OEF and CMRO2. Furthermore, a lower OEF predicted a longer stay in the neonatal ICU.
Impact: The brain’s physiological parameters such as oxygen-extraction-fraction can provide additional information (beyond standard clinical indices) for cerebral injury evaluation and treatment planning for hypoxic-ischemic-encephalopathy.
INTRODUCTION
Hypoxic ischemic encephalopathy (HIE) is a leading cause of neonatal mortality and neurological disabilities, affecting 1.5 newborns per 1000 live birth1. Although the introduction of therapeutic hypothermia has reduced the risk of death and disability in neonates with HIE, over 40% of neonates with moderate or severe HIE still suffer from death, disability or neurodevelopmental delay, suggesting the need for adjuvant therapies2. Because HIE is associated with the disruption of the brain’s oxygen supply, the assessment of cerebral oxygen metabolism may provide useful biomarkers to identify the risk of permanent neurologic injury and determine the necessity of adjuvant treatments in HIE. Cerebral oxygen metabolism is characterized by physiological parameters including oxygen-extraction-fraction (OEF), cerebral-blood-flow (CBF) and cerebral-metabolic-rate-of-oxygen (CMRO2). In this study, we aimed to evaluate these physiological parameters in neonates with HIE in comparison with healthy newborns and examine whether these parameters could predict short-term clinical outcome.METHODS
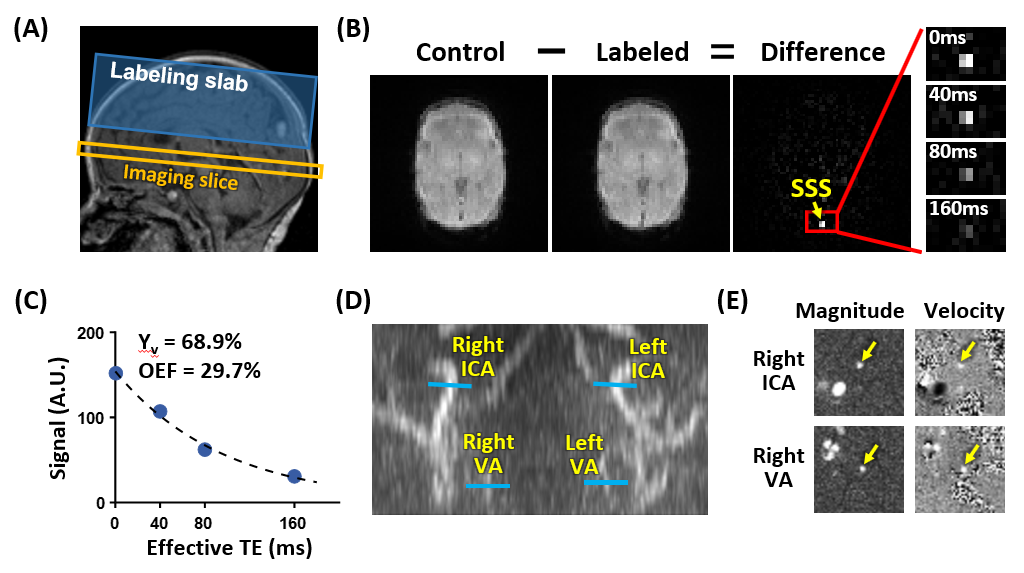
Participants: In this IRB-approved study, we included 42 neonates with HIE (20 females, birth-age 38.9±1.7weeks) and 52 control neonates (26 females, birth-age 39.0±1.0weeks). Table 1 lists the characteristics of the participants.MRI Experiments: All neonates were scanned on 3T Siemens Skyra or Trio systems. Global OEF was evaluated using T2-relaxation-under-spin-tagging (TRUST) MRI, which is a PET-validated technique3 and has been optimized for neonatal applications4. To quantify global CBF, phase-contrast MRI was employed to measure the total blood flow in the brain’s feeding arteries in a subset of neonates (35 HIE and 20 control)5. Arterial-oxygenation (Ya) of each neonate was assessed by an MRI-compatible pulse oximeter.
Data Processing: The TRUST data were processed to obtain global venous-oxygenation (Yv)3,4. Global CBF was calculated as the total arterial blood flow normalized by the brain mass. Global OEF and CMRO2 were computed as: $$OEF=(Y_a-Y_v)/Y_a\times100\%$$
$$CMRO_2=(Y_a-Y_v){\times}CBF{\times}C_h$$
where Ch=8.97μmol O2/ml for a hematocrit of 0.446. MRI images of neonates with HIE were graded by a board-certified neuroradiologist using the National-Institute-of-Child-Health-and-Human-Development (NICHD) score7.
Statistical Analysis: Linear regression analyses were used to compare OEF, CBF and CMRO2 between neonates with HIE and healthy controls, with postmenstrual-age at the MRI scan and sex as covariates. We further stratified neonates with HIE based on their Sarnat scores (a clinical rating of neonatal HIE severity) or the presence of structural brain lesions (NICHD>0) and employed analysis-of-covariance (ANCOVA) followed by Tukey’s tests to compare OEF, CBF and CMRO2 across the control group and the HIE subgroups. Finally, we utilized linear regression (adjusted for birth-age and sex) to examine whether OEF, CBF or CMRO2 can predict NICU length-of-stay (LoS) in neonates with HIE, a metric for short-term clinical outcome.
RESULTS AND DISCUSSION
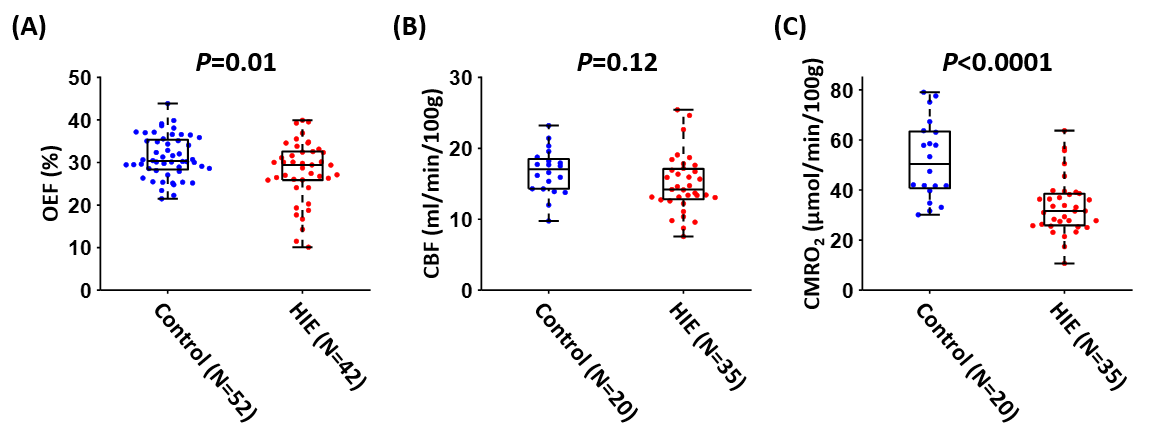
Figure 1 depicts representative TRUST and phase-contrast data of a neonate with HIE.As shown in Figure 2, compared to control neonates, neonates with HIE exhibited diminished OEF (P=0.01) and CMRO2 (P<0.0001), suggesting impaired cerebral oxygen metabolism. CBF showed no significant difference (P=0.12).
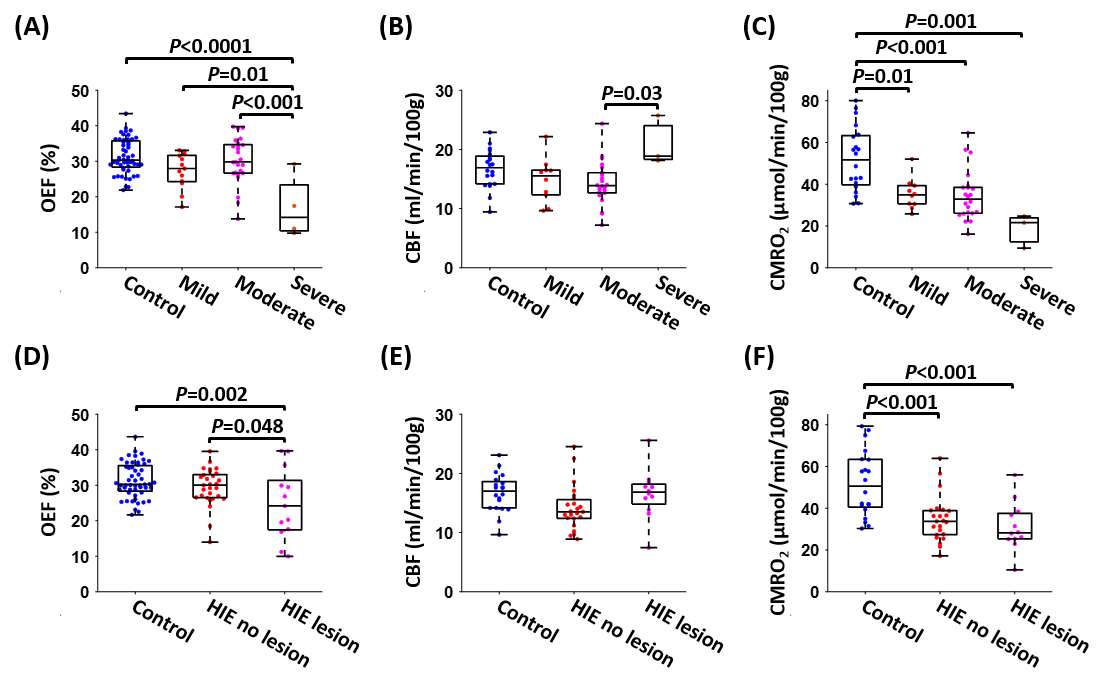
When stratifying neonates with HIE based on the Sarnat score (Figure 3A-C), ANCOVA revealed significant group differences in OEF (P<0.0001), CBF (P=0.02) and CMRO2 (P<0.0001). Specifically, neonates with severe HIE had reduced OEF compared to other groups (Figure 3A), while all HIE subgroups had lower CMRO2 than the control group (Figure 3C). When categorizing the neonates with HIE based on the presence of structural brain lesions (Figure 3D-F), significant group differences were found in OEF (P=0.003) and CMRO2 (P=0.0001), but not in CBF (P=0.07). HIE neonates with structural brain lesions exhibited lower OEF compared to both the controls (P=0.002) and HIE neonates without brain lesions (P=0.048). Compared to control neonates, CMRO2 was diminished in HIE neonates with (P<0.001) or without (P<0.001) structural brain lesions. These results suggest that CMRO2 is sensitive to mild brain impairments even when there are no abnormalities in structural MRI. On the other hand, reduction in OEF is mostly seen in neonates with more severe brain injury.
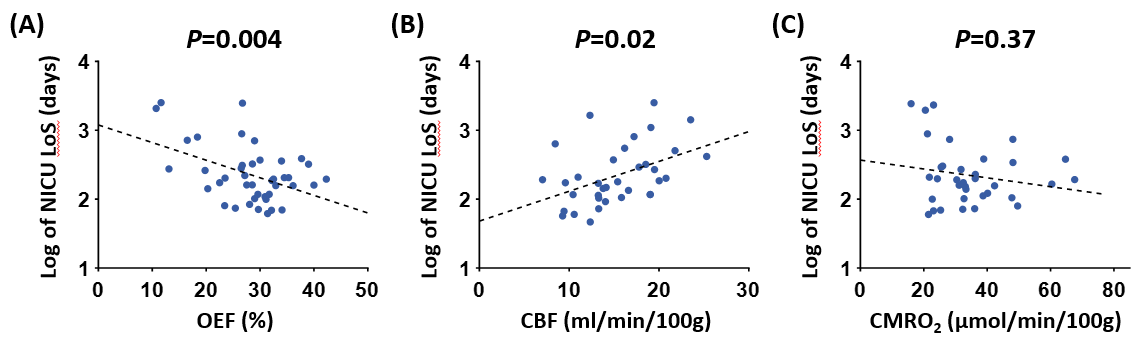
Finally, we found that a lower OEF predicted a longer NICU LoS (P=0.004, Figure 4A). NICU LoS was positively associated with CBF (P=0.02, Figure 4B) but not with CMRO2 (P=0.37, Figure 4C). It is worth noting that NICU LoS was not associated with Sarnat score (P=0.33) or the presence of structural brain lesions (P=0.12), indicating that physiological parameters such as OEF can provide additional information (beyond standard clinical indices) for treatment planning in HIE.
CONCLUSION
This work demonstrated that the brain’s OEF and CMRO2 were diminished in neonates with HIE. Furthermore, a lower OEF predicted longer stay in NICU. These findings suggest that physiological biomarkers such as OEF and CMRO2 may be useful in cerebral injury evaluation and treatment planning for HIE.Acknowledgements
No acknowledgement found.References
1. Kurinczuk JJ, White-Koning M, Badawi N. Epidemiology of neonatal encephalopathy and hypoxic-ischaemic encephalopathy. Early Hum Dev 2010;86:329-338.2. Shankaran S, Pappas A, McDonald SA et al. Childhood outcomes after hypothermia for neonatal encephalopathy. N Engl J Med 2012;366:2085-2092.
3. Jiang D, Deng S, Franklin CG, O'Boyle M, Zhang W, Heyl BL, Pan L, Jerabek PA, Fox PT, Lu H. Validation of T2 -based oxygen extraction fraction measurement with (15) O positron emission tomography. Magn Reson Med 2021;85:290-297.
4. Liu P, Parkinson C, Jiang D, Ouyang M, De Vis JB, Northington FJ, Tekes A, Huang H, Huisman T, Golden WC. Characterization of MRI techniques to assess neonatal brain oxygenation and blood flow. NMR Biomed 2019;32:e4103.
5. Liu P, Qi Y, Lin Z, Guo Q, Wang X, Lu H. Assessment of cerebral blood flow in neonates and infants: A phase-contrast MRI study. Neuroimage 2019;185:926-933.
6. Liu P, Huang H, Rollins N, Chalak LF, Jeon T, Halovanic C, Lu H. Quantitative assessment of global cerebral metabolic rate of oxygen (CMRO2) in neonates using MRI. NMR Biomed 2014;27:332-340.
7. Shankaran S, Barnes PD, Hintz SR et al. Brain injury following trial of hypothermia for neonatal hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed 2012;97:F398-404.
Figures
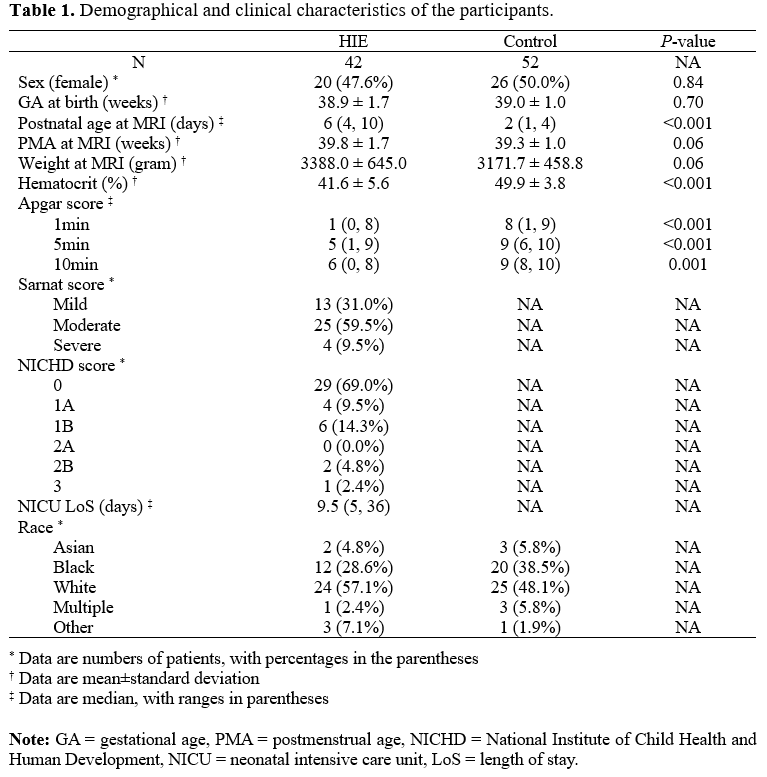
Table 1. Demographical and clinical characteristics of the participants.