2357
The association between white matter hyperintensity and acute cerebral infarction using MTP synthetic sequence1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2The First Affiliated Hospital of Dalian Medical University, dalian, China
Synopsis
Keywords: Stroke, Stroke, synthetic sequence, white matter hyperintensity,acute ischemic stroke
Motivation: The application of MTP synthetic sequence can shorten the examination time of patients and obtain routine and quantitative MRI images, widely used in clinical.
Goal(s): This study aims to distinguish acute ischemic stroke and white matter hyperintensity (WMH) as well as normal tissue using MTP synthetic sequence.
Approach: We compared acute ischemic stroke, WMH and normal gray-white matter ADC and MTP values, investigated the clinical value of MTP in distinguishing these two kinds of diseases.
Results: The signal of acute cerebral infarction was obviously different from WMH and normal cerebral tissue.
Impact: MTP imaging offers the potential to distinct acute ischemic stroke from WMH and normal brain regions in just a few minutes.
Introduction
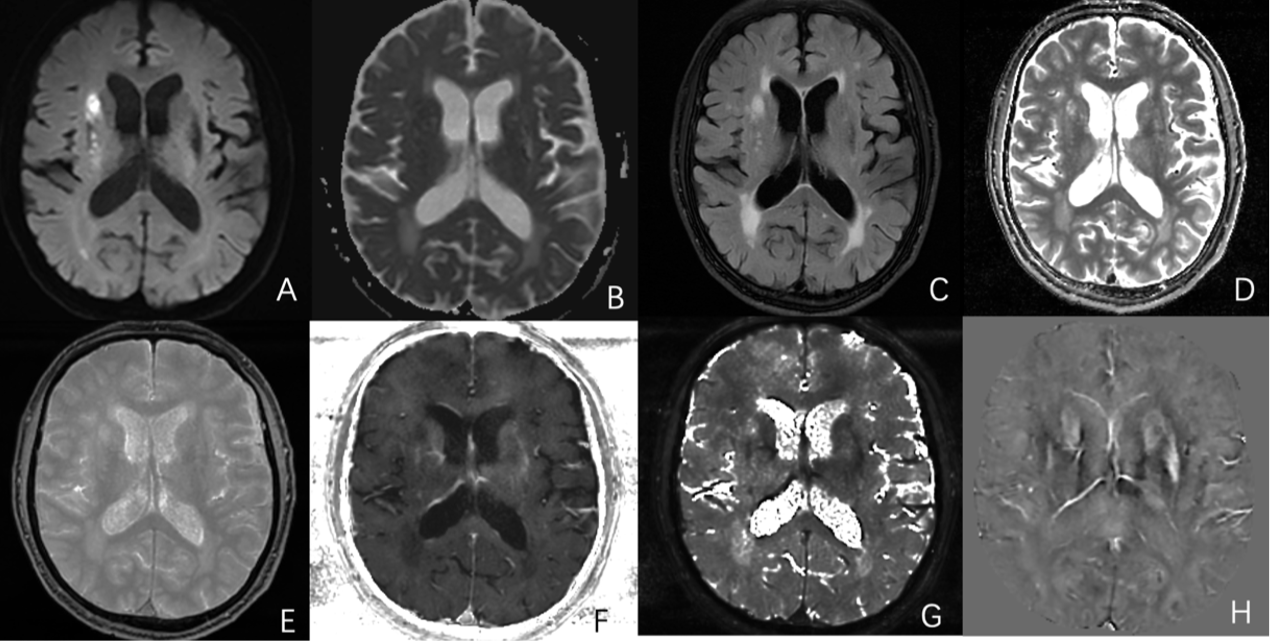
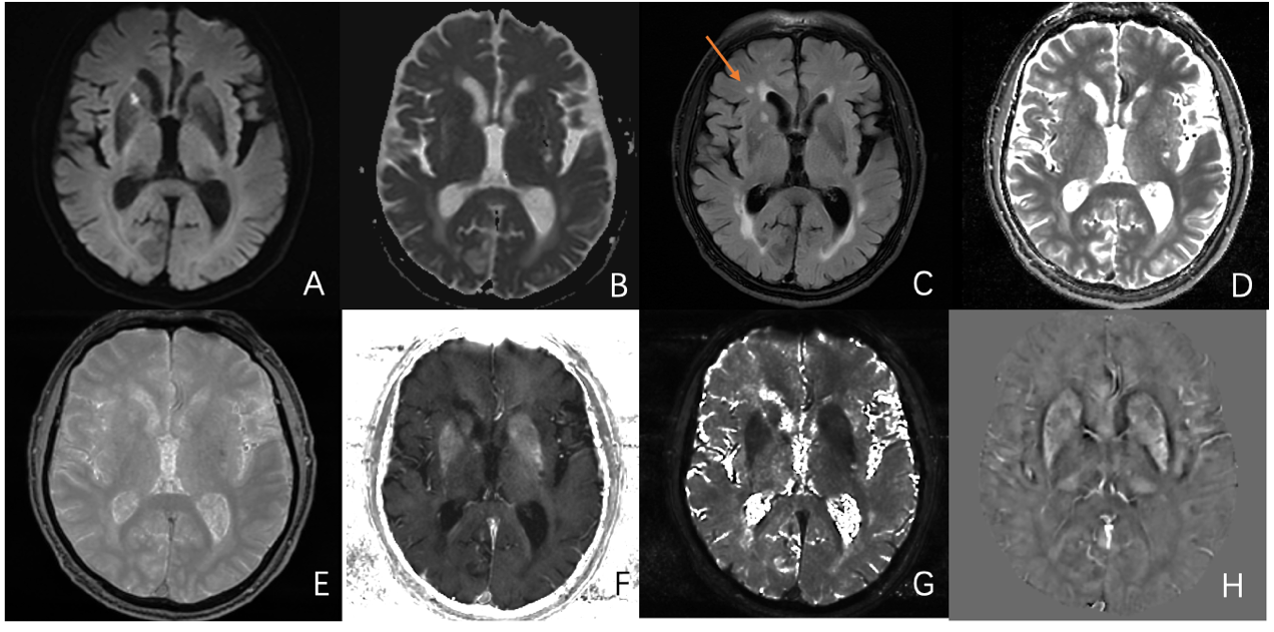
In general, acute ischemic infarction is identified by DWI sequences, which need a certain amount of time. Besides, acute ischemic infarction and WMH are difficult to distinguish without DWI. MTP synthetic sequence allows rapid simultaneous quantification of multiple tissue characteristics, including T1 map, T2 Star, R2 star, proton density (PD) map, and quantitative susceptibility mapping (QSM) with one acquisition. This study was conducted to investigate the value of MTP in the diagnosis of acute cerebral infarction and WMH.Methods
Forty patients with acute or subacute cerebral infarction were scanned by conventional MR imaging as well as MTP. The clinical base data of all patients were recorded. We placed a circular ROI in ischemic lesion and mirror area to quantify MTP-derived T1 map, PD map, R2 Star, T2 Star and QSM values. For WMH, ROIs were placed in significant areas of periventricular hyperintensity (PVH) or deep white matter hyperintensities (DWMH). For normal tissue, ROIs were placed in white matter (centrum semiovale, genu of the corpus callosum), grey matter (superior frontal cortex andthalamus) on the lesion side. Statistical analysis of the obtained T1 map, PD map, R2 Star, T2 Star and QSM values between ischemic stroke and WMH, and normal tissue were compared by the independent sample t-test or Mann-Whitney U test. Receiver operating characteristic (ROC) curves, wherein areas under the curves (AUCs) and 95% confidence intervals were calculated to compare the discriminatory power of quantitative parameters of MTP for predicting infarction and WMH.Results
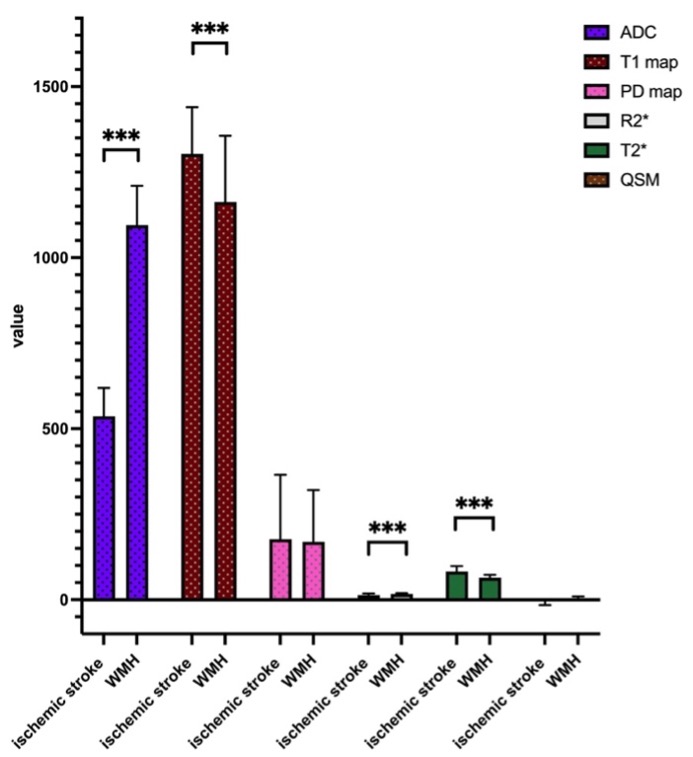
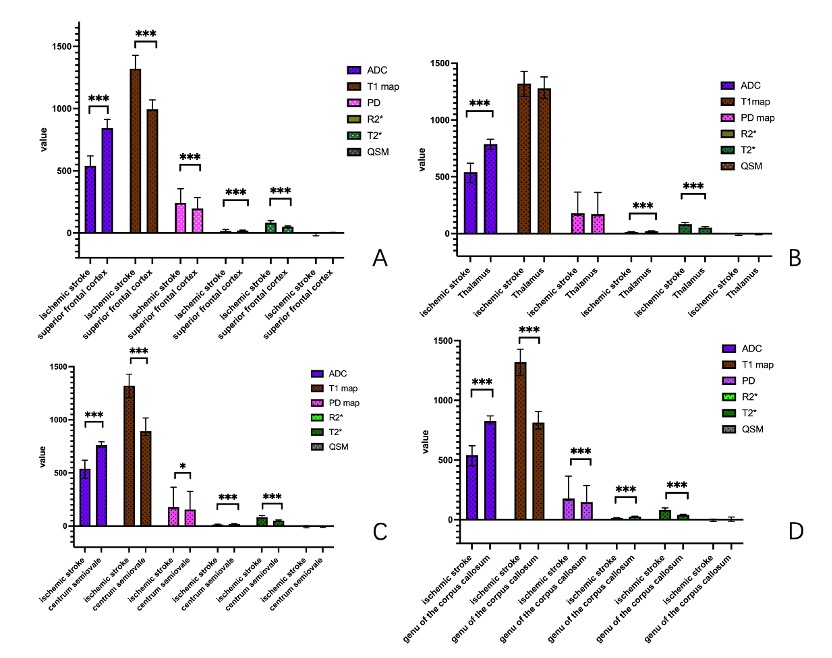
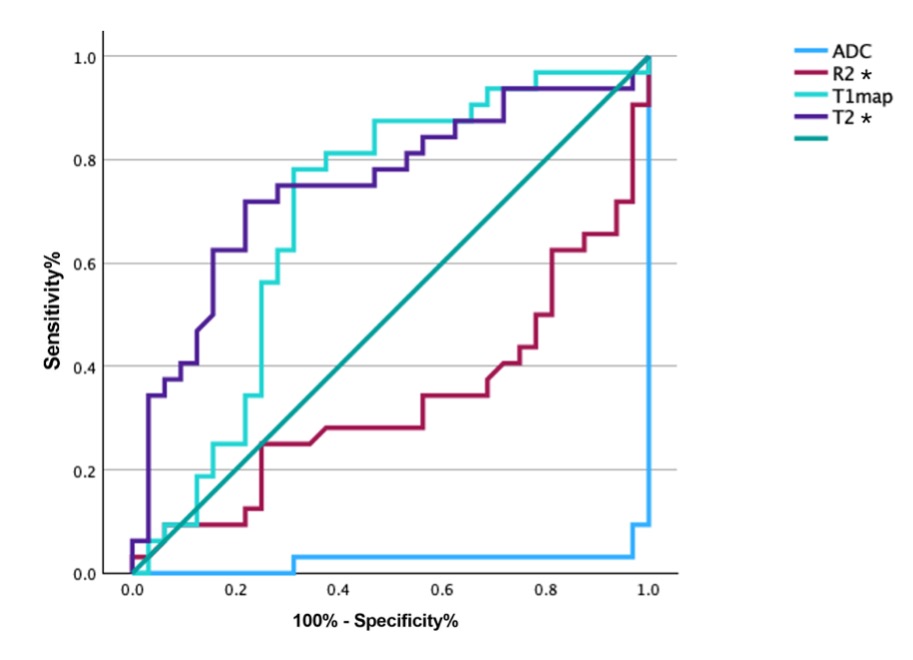
A total of 40 patients (age 66.48±12.06, 67.5% men) were analyzed, and 32 patients with obvious WMH. The value of ADC and R2 Star of ischemic lesion area were significantly lower than WMH, while the value of T1 Map and T2 Star was higher in ischemic lesion (p<0.05). There were no differences in the value of PD Map and QSM between infarction and WMH (Figure 1-3). Except for QSM,infarction and WMH values of MTP were significantly different from those of normal gray matter and white matter, especially in T2 Star and R2 Star (p<0.001, Figure 4).The AUC of ADC, T1 Map, R2 Star, T2 Star to predict acute ischemic stroke was 0.02, 0.69, 0.33, 0.75, respectively (p < 0.05). Among these parameters, T1 map and T2 Star have produced best performances, even better than ADC values (Figure 5)Discussion
Acute ischemic lesions MTP values compared to WMH showed lower ADC, R2 Star and higher T1 map, T2 Star, maybe reflect the development of vasogenic edema and increasing tissue water content. The signal of acute cerebral infarction was obviously different from normal cerebral tissue, WMH also very different from normal deep white matter or periventricular white matter, which means different pathological mechanism. Accurate and rapid diagnosis helps the clinician’s diagnosis, management, and prognosis by describing lesion evolution and abnormalities. MTP can offer multiple parameters dynamically adjustable for contrast and color-coded visualization, these advantages are very useful for patients with acute cerebral infarction. T2 Map has been assessed in acute stroke in a previous study focused on ischemic lesion with a known time of symptom onset [1]. Li et al provided a phantom validation study of the reliability of sMRI relaxometry measures for chronic ischemic stroke [2]. These studies indicate that MTP has great clinical application value,quantitative data may be related to clinical characteristics and deserve further study.Conclusion
T1 map and T2 Star can effectively distinguish infarcted brain tissue from WMH and normal region by providing quantitative and qualitative information.Acknowledgements
No acknowledgement found.References
1.Duchaussoy, T. et al. Synthetic T2 mapping is correlated with time from stroke onset: A future tool in wake-up stroke management? Eur. Radiol. 29, 7019–7026 (2019).
2. Li, C.-W. et al. Reliability of synthetic brain MRI for assessment of ischemic stroke with phantom validation of a relaxation time determination method. J. Clin. Med. 9, 1857 (2020).
Figures