2356
Hemodynamic quantification for modelling functional outcome in stroke population using 4D Flow Imaging – a pilot study1Department of Nuclear Magnetic Resonance, All India Institute of Medical Sciences, New Delhi, India, 2Department of Neurology, All India Institute of Medical Sciences, New Delhi, India, 3Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India, 4DI-MRI, Siemens Healthineers, Bangalore, India, 5Diagnostic Imaging, Siemens Healthineers, Gurugram, India
Synopsis
Keywords: Stroke, Ischemia
Motivation: Recurrent stroke is associated to hemodynamic abnormalities in ischemic stroke population, and MRI may play a major role in routine clinical setting.
Goal(s): Our goal was to assess hemodynamic variation in aortic region in stroke population (especially in subacute phase) undergoing routine treatment.
Approach: we used 4D flow imaging method which employs a non-contrast method with respiratory motion compensation method to acquire flow dynamics in stroke population to assess the aortic flow quantification.
Results: Flow abnormalities are significantly differing across subacute phase suggesting changes in hemodynamic.
Impact: Understanding cardiac flow dynamics in subacute phase of stroke population (undergoing clinical treatment) can help in understanding the functional recovery pattern to stratify recovery from recurrent stroke condition in future.
Introduction
Atherosclerosis is one of the leading causes of cardiovascular diseases, which may also cause Transient and Acute ischemic stroke1,2. The onset of atherosclerosis and its effect on cardiovascular function is not understood till the onset of symptoms (eg. Stroke, peripheral artery diseases, etc.)3. In stroke population symptomatic treatment for functional symptoms are addressed in clinical setting4. The evaluation of underlying pathology changes is an ongoing process that needs to be understood, as changes occur gradually across subacute to chronic phase. In this study, we targeted stroke population in subacute phase (1-month and 3-month post onset) to understand any flow abnormalities post treatment that may present deterioration in the functional outcomes. We attempted to study the variables that may isolate the functional recovery pattern for patients with poor response to treatment.Method
Five ischemic patients with middle cerebral artery (MCA) territory infarct in subacute phase at 1 (group 2) and 3 months (group 3), with mean age 57 and 50 years respectively and 5 healthy control (group 1) subjects with mean age 51 years were recruited for the study. Cardiac imaging was conducted on a 1.5T MR scanner (Magnetom Aera, Siemens Healthcare GmbH, Erlangen, Germany), with two conventional 4D flow acquisition approaches using prototype sequence provided by Siemens Healthcare GmbH, Germany. An aorta specific 4D flow imaging sequence with rectangular slab in sagittal oblique orientation using an axial haste reference scan with phase encoding in AP direction was used with acquisition plane. Sequence including descending aorta with respirator motion compensation was established using pencil beam navigator to restrict interference for acquisition volume.Data processing for flow parameter extraction was done using 4D Flow demonstrator software version 2.4 (a prototype provided by Siemens Healthineers, Germany). In order to optimize the velocity field, pre-processing for background phase correction inside phase-contrast images was carried out. Phase anti-aliasing and motion tracking were used to generate deformation fields and rectify VENC overestimation for additional vessel model. Aortic flow abnormalities were estimated for ascending and descending aorta with two plane 3 cm away from ascending aorta root and 2 plane at 4 cm of exiting aortic arch. A time integrated averaging approach was used to estimate net value across cardiac cycles. To quantify the parameter that may be associated with hemodynamic variation across subacute phase canonical functional analysis was employed. The analysis of ascending and descending aorta was independent on each plane for quantification of the functional outcome.Result
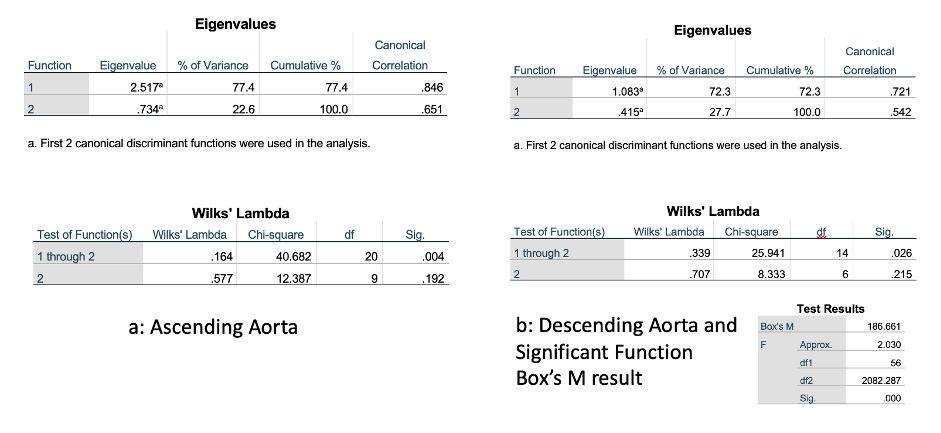
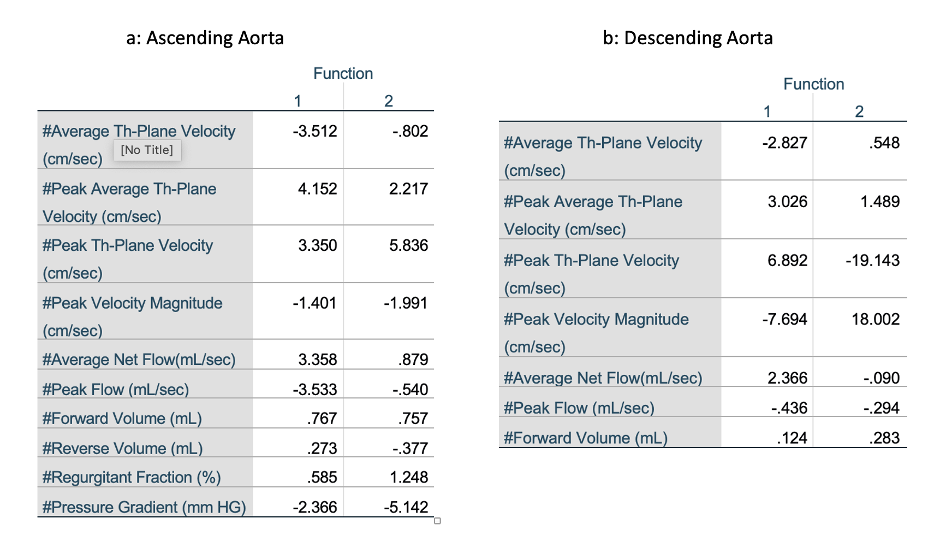
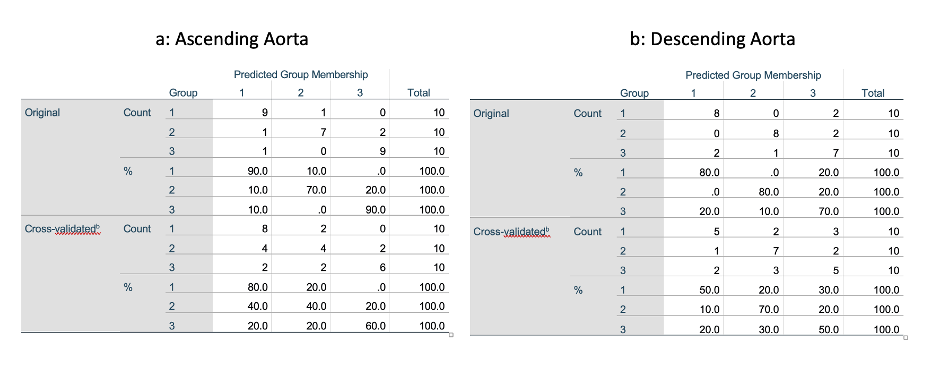
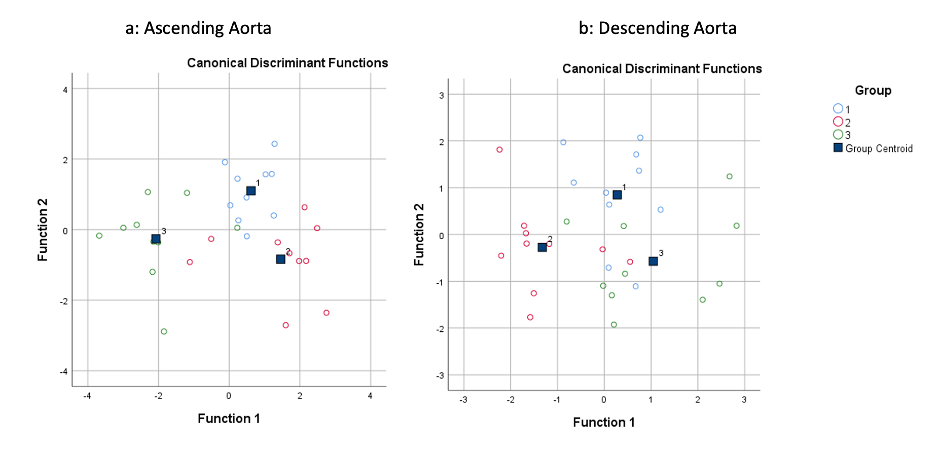
An optimised two function discriminant coefficient was significant in descending aorta in comparison to ascending aorta (Figure 1). Variable coefficient such as Peak Th-Plane Velocity, Average Net Flow, Peak Average Th-Plane Velocity showed highest functional coefficient for ascending/descending aorta (Figure 2). The cross validation of classification function to correctly classify the two timepoints of 1 and 3 months flow parameters was also computed which yield 60% across ascending aorta and 56.7% across descending aorta (Figure 3). The function for ascending aorta and descending aorta also showed centroid placement with similar distribution when evaluated at group means (Figure 4).Discussion
Flow velocity and through plane velocity are significant factors that may also be associated to aortic stiffness5. Recurrent stroke pathology is generally associated to cardiovascular modulation due to initial onset of diseases6. Changes in the flow hemodynamics in both ascending and descending aorta in the study groups highlight the importance of flow estimation quantification for stroke population which were not presented with embolic pathology. Significant canonical coefficient of net flow in ascending and descending aorta shows the changes which may associated to underlying vascular changes7,8. The inference is based on a single time-point pilot study of ischemic stroke patient. As the subjects (in the current study) complete their sub-acute phase, when they enter chronic phase an observational follow-up may cross-validate the hemodynamic modulation observed in current study. This validation will help in modelling functional recovery estimation based on clinical scales and vascular changes assessment using 4D flow technique.Conclusion
The cardiovascular nature of stroke aetiology is well documented, but functional outcome assessment at clinical setting (post onset of disease) is necessary in long term stroke management. 4D flow can provide vascular hemodynamic quantification.Acknowledgements
No acknowledgement found.References
1. Pandian, J. D. et al. Prevention of stroke: a global perspective. The Lancet Preprint at https://doi.org/10.1016/S0140-6736(18)31269-8 (2018).
2. Mendelson, S. J. & Prabhakaran, S. Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review. JAMA - Journal of the American Medical Association 325, 1088–1098 (2021).
3. Sträter, A. et al. 4D-Flow MRI: Technique and Applications. Rofo 190, 1025–1035 (2018).
4. Campbell, B. C. V. & Khatri, P. Stroke. The Lancet 396, 129–142 (2020).
5. François, C. J. et al. Four-dimensional, flow-sensitive magnetic resonance imaging of blood flow patterns in thoracic aortic dissections. J Thorac Cardiovasc Surg 145, 1359–66 (2013).
6. Phan, T. G., Hilton, J., Beare, R., Srikanth, V. & Sinnott, M. Computer modeling of anterior circulation stroke: Proof of concept in cerebrovascular occlusion. Front Neurol (2014) doi:10.3389/fneur.2014.00176.
7. Wehrum, T. et al. Quantification of aortic stiffness in stroke patients using 4D flow MRI in comparison with transesophageal echocardiography. International Journal of Cardiovascular Imaging 34, (2018).
8. Garcia, J., Barker, A. J. & Markl, M. The Role of Imaging of Flow Patterns by 4D Flow MRI in Aortic Stenosis. JACC: Cardiovascular Imaging vol. 12 Preprint at https://doi.org/10.1016/j.jcmg.2018.10.034 (2019).
Figures