2352
Assessment of cerebral microbleeds using improved 7T SWI in Alzheimer’s disease1Urmia University of Medical Science, urmia, Iran (Islamic Republic of), 2Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
Keywords: Alzheimer's Disease, Alzheimer's Disease
Motivation: Cerebral microbleeds (CMBs) are small hemosiderin-laden macrophage clusters resulting from blood leakage about damaged cerebral vessels, often linked to β-amyloid (Aβ) deposition.
Goal(s): To improve the visualization of CMBs that might be missed or undetectable with lower field strengths in mild cognitive impairment (MCI) and AD patients.
Approach: A new SWI technique named CLEAR-SWI was reported to eliminate the artifacts common in standard, single-echo SWI, reduce signal dropouts, and improve image homogeneity and contrast-to-noise.
Results: We found a significant correlation between the number of lobar CMBs and the Aβ PET SUVR levels in AD/MCI patients.
Impact: Improved visualization of CMBs with CLEAR SWI sequences at 7T may contribute to more accurate identification of MCI and AD patients, who typically present a lobar distribution of CMBs.
Introduction
Cerebral microbleeds (CMBs) are small, round aggregations of hemosiderin-laden macrophages that indicate leakage of blood products from cerebral vessels damaged by β-amyloid (Aβ)1. Studies have shown that the presence of CMBs is associated with a higher risk of cognitive decline and an increased likelihood of developing Alzheimer's disease (AD)2. CMBs can be visualized commonly using T2*-weighted GRE sequences in MRI3. In recent years, the introduction of susceptibility-weighted imaging (SWI) has improved CMB detection in MRI4. The increased magnetic field strength at 7T MRI results in substantially enhanced sensitivity to variations in magnetic susceptibility5. The more robust SWI at 7T MRI proves especially advantageous in the detection of CMBs. However, at 7T, inhomogeneous static and transmit fields lead to intensity alterations which make SWI challenging to window and interpret6. A new SWI technique named CLEAR-SWI was reported to eliminate the artifacts common in standard, single-echo SWI, reduce signal dropouts, and improve image homogeneity and contrast-to-noise7. In this study, we used the CLEAR SWI technique at 7T MRI to improve the visualization of CMBs that might be missed or undetectable with lower field strengths in mild cognitive impairment (MCI) and AD patients.Methods
Imaging with two AD, four MCI, and six healthy subjects (73 ± 6 years old) was performed using a 7T MRI scanner (Siemens Healthineers, Erlangen, DE) with a Nova Medical 32Rx/1Tx head coil (Wilmington, Massachusetts, USA). To acquire CLEAR SWI, a 3D multi-echo GRE sequence was used (six echo times (TE), TE=4 ms, ΔTE=4ms, voxels size = 0.3x0.3x1.5 mm3, TR= 32 ms, flip angle = 12, and bw = 160 Hz/px). All steps in SWI processing including coil combination, phase unwrapping, image combination over echoes, phase filtering, and homogeneity correction have been addressed. The images were analyzed by two neuroradiologists. CMBs were defined as small hypointense lesions within the brain parenchyma on the SWI images. The microbleeds were categorized into two groups according to their locations: non-lobar region (basal ganglia, thalamus, and infratentorial) and the lobar region (frontal, parietal, temporal, and occipital). Calcifications of the basal ganglia and deep cerebellar nuclei were considered as normal findings. The analysis was performed to evaluate the associations between the number of CMB lesions with the patient’s Aβ PET SUVR levels.Results
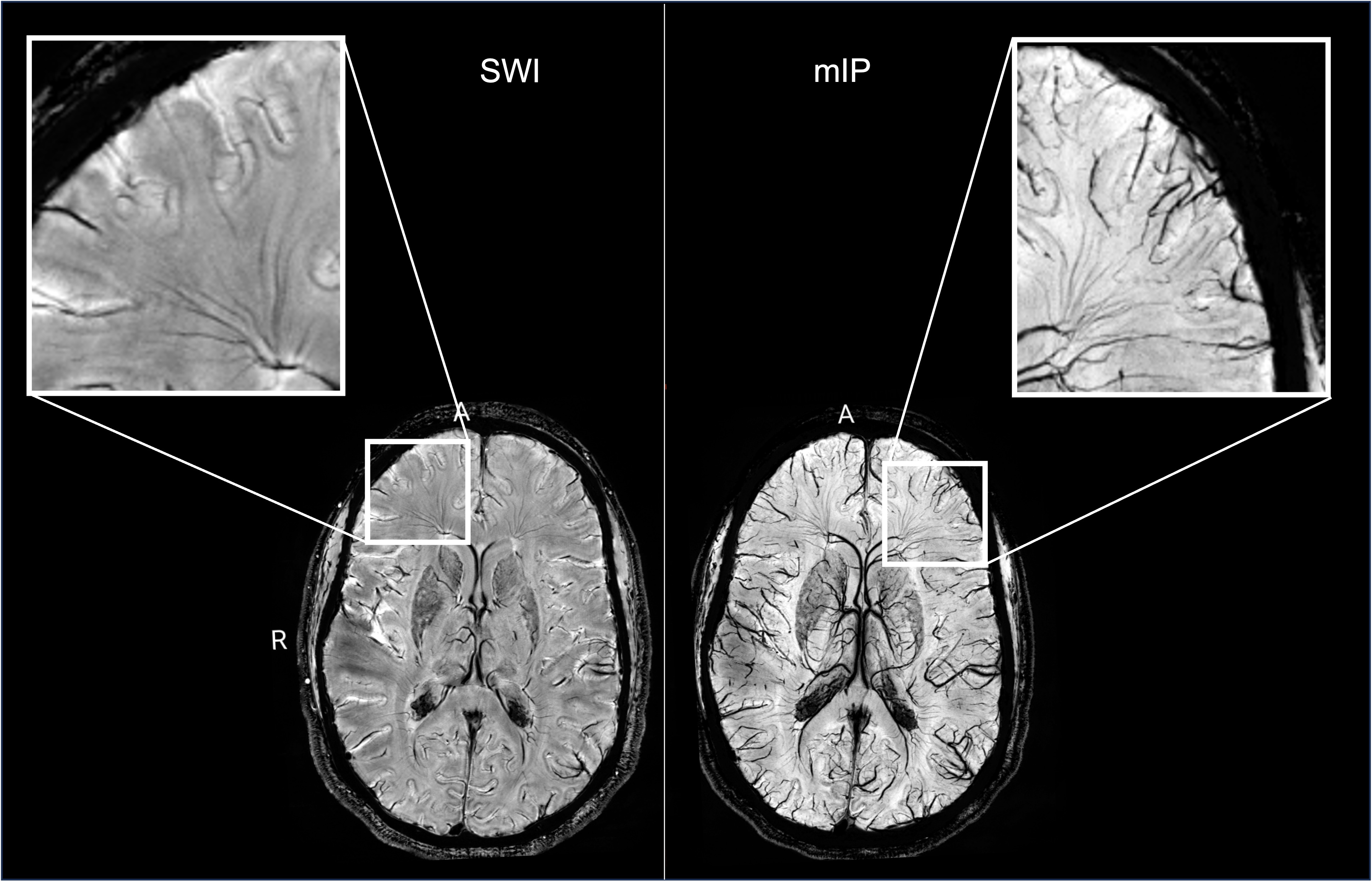
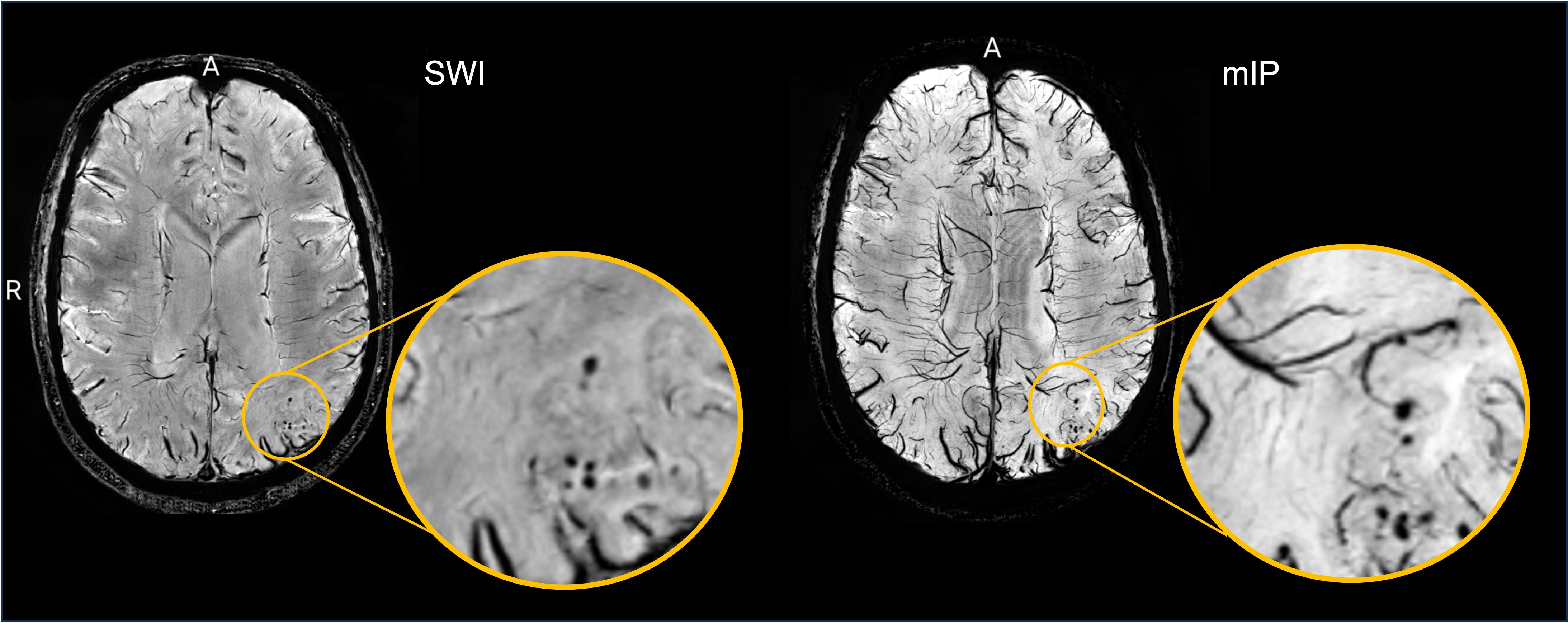
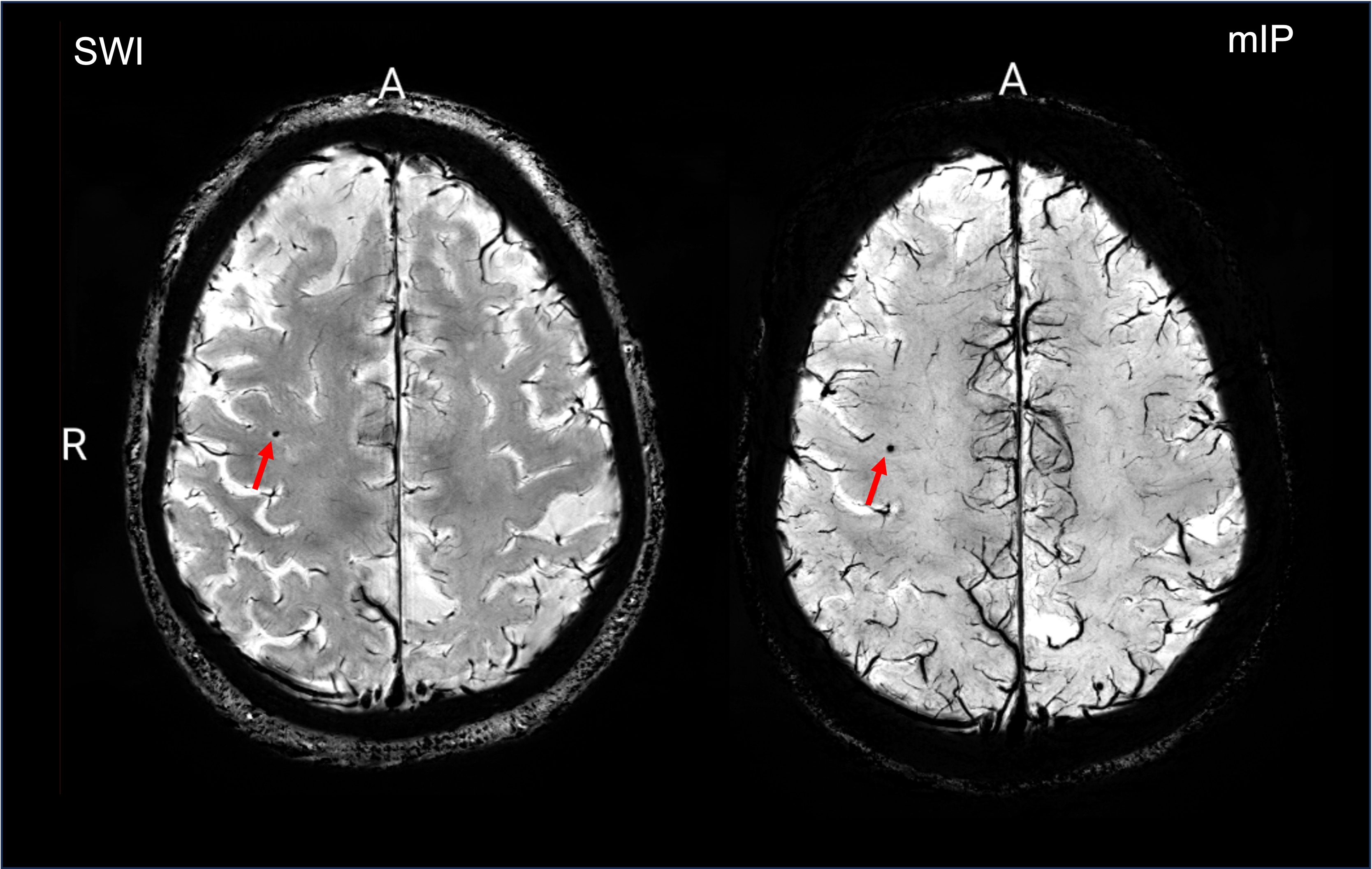
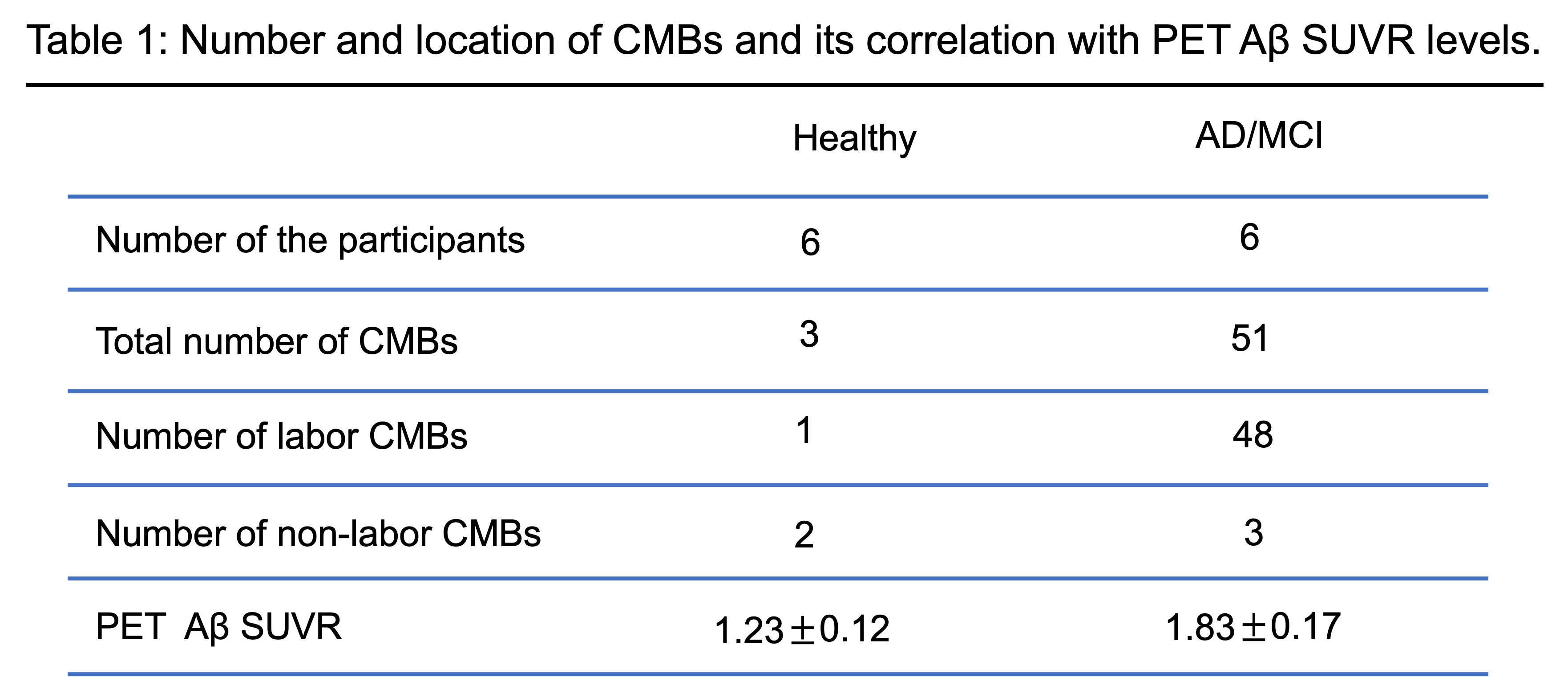
Using CLEAR- SWI at 7T led to higher contrast-to-noise images, reduced inhomogeneities, and allowed for better detection of CMBs and visibility of veins (Figure 1). Our results showed that out of 51 observed CMBs in six MCI/AD patients 48 (94%) CMBs were lobar and 3 (6%) non-lobar. One non-lobar CMB was found in an AD patient (1 CMB) and two CMBs were found in an MCI patient. SWI and corresponding mIP images show the lobar distribution of CMBs in an AD patient (Figure 2). It is important to note that SWI is indicated with mIP where ASPIRE applies. Enhanced SWI at 7T led to improved visualization of small CMBs in the zoomed images. A total of 3 CMBs (one labor and 2 non-lobar) were observed in six healthy participants. Figure 3 illustrates a labor CMB in the partial lobe in a healthy participant, as indicated by the red arrow. Table 1 summarizes the number and location of the CMBs. The number of lobar CMBs was correlated to Aβ PET SUVR levels of MCI and AD patients. A significant correlation was found between the number of lobar CMBs and the Aβ PET SUVR levels in AD/MCI patients (Table 1).Discussion
We used a comprehensive enhanced SWI acquisition and processing (CLEAR-SWI) technique to improve the visualization of CNBs in MCI and AD patients at 7T MRI. In this study, we showed lobar distribution of CMBs is associated with MCI and AD as reported in previous studies. We reviewed six healthy individuals, two AD, and four MCI patients. Out of a total of 51 observed CMBs in six MCI/AD patients, 48 CMBs were located in lobar regions (Table 1). We found a significant correlation between the number of lobar CMBs and the Aβ PET SUVR levels in AD/MCI patients. This improved SWI at 7T for visualization of CMBs may lead to the detection of a larger number of CMBs and consequently provide a more precise correlation. This study needs to be assessed with a larger cohort to provide precise statistical analysis.Conclusion
Improved visualization of CMBs with CLEAR SWI sequences at 7T may contribute to more accurate identification of MCI and AD patients, who typically present a lobar distribution of CMBs.Acknowledgements
The authors would like to thank research coordinator Aislinn Diaz for helping with the recruitment. This study was supported by a Developmental Project award from Mount Sinai ADRC (P30 AG066514) NIA/NIH, R21AG071179, and K01 AG075178-01 NIA/NIH grants.References
1. Greenberg SM, Vernooij MW, Cordonnier C, et al. Cerebral microbleeds: a guide to detection and interpretation. Lancet Neurol 2009;8:165–174.
2. Cordonnier C, van der Flier WM (2011) Brain microbleeds and Alzheimer’s disease: Innocent observation or key player? Brain 134, 335-344.
3. Vernooij MW, Ikram MA, Wielopolski PA, Krestin GP, Breteler MM, van der Lugt A. Cerebral microbleeds: accelerated 3D T2*-weighted GRE MR imaging versus conventional 2D T2*-weighted GRE MR imaging for detection. Radiology. 2008 Jul;248(1):272-7. doi: 10.1148/radiol.2481071158. Epub 2008 May 19. PMID: 18490493.
4. Nandigam RN, Viswanathan A, Delgado P, et al. MR imaging detection of cerebral microbleeds: effect of susceptibility- weighted imaging, section thickness, and field strength. AJNR Am J Neuroradiol 2009; 30: 338–343.
5. Brundel M, Heringa SM, de Bresser J, Koek HL, Zwanenburg JJ, Jaap Kappelle L, Luijten PR, Biessels GJ. High prevalence of cerebral microbleeds at 7Tesla MRI in patients with early Alzheimer's disease. J Alzheimers Dis. 2012;31(2):259-63. doi: 10.3233/JAD-2012-120364. PMID: 22531417.
6. Ladd ME, Bachert P, Meyerspeer M, Moser E, Nagel AM, Norris DG, Schmitter S, Speck O, Straub S, Zaiss M. Pros and cons of ultra-high-field MRI/MRS for human application. Prog Nucl Magn Reson Spectrosc. 2018 Dec;109:1-50. doi: 10.1016/j.pnmrs.2018.06.001. Epub 2018 Jun 8. PMID: 30527132.
7. Eckstein K, Bachrata B, Hangel G, Widhalm G, Enzinger C, Barth M, Trattnig S, Robinson SD. Improved susceptibility weighted imaging at ultra-high field using bipolar multi-echo acquisition and optimized image processing: CLEAR-SWI. Neuroimage. 2021 Aug 15;237:118175. doi: 10.1016/j.neuroimage.2021.118175. Epub 2021 May 15. PMID: 34000407; PMCID: PMC7612087.
8. Robinson S, Grabner G, Witoszynskyj S, Trattnig S. Combining phase images from multi-channel RF coils using 3D phase offset maps derived from a dual-echo scan. Magn Reson Med. 2011 Jun;65(6):1638-48. doi: 10.1002/mrm.22753. Epub 2011 Jan 19. PMID: 21254207.
Figures