2344
Distinct progression patterns of white matter microstructure in Parkinson’s disease associated with REM sleep behavior disorder1zhejiang university school of medicine, Hangzhou, China, 2GE Healthcare, Shanghai, China
Synopsis
Keywords: Parkinson's Disease, Neurodegeneration, Rapid eye movement sleep behavior disorder
Motivation: Rapid eye movement sleep behavior disorder (RBD) significantly impacts clinical outcomes in Parkinson's disease (PD).
Goal(s): Our goal was to investigates the neurophysiological mechanisms related to motor and cognitive decline longitudinally in PD with RBD (PD-RBD).
Approach: We used diffusion tensor imaging and clinical assessments on 83 PD patients over 2 years, two groups were formed: PD-RBD and PD without RBD (PD-nonRBD).
Results: PD-RBD experienced widespread decline in white matter microstructure which are associated with motor symptoms aggravation, while PD-nonRBD patients showed limited changes.
Impact: The presence of RBD suggests more extensive white matter degeneration in PD, particularly affecting motor symptoms.
Purpose
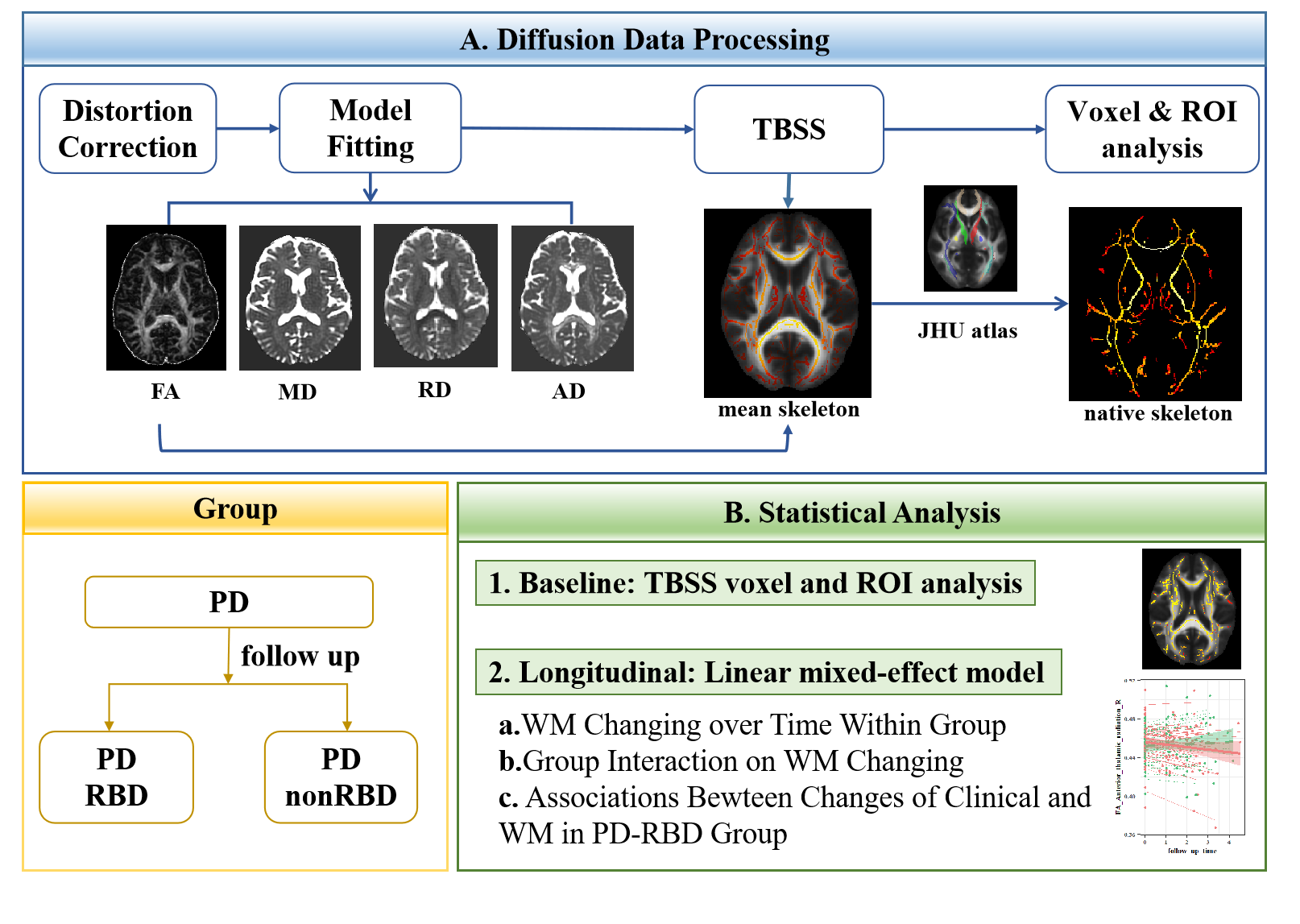
In Parkinson's disease (PD), the presence of rapid eye movement (REM) sleep behavior disorder (RBD) is strongly associated with poor clinical prognosis. However, no study to date has investigated the longitudinal white matter (WM) microstructure changes underlying RBD. The aim of the study was to investigate the longitudinal progression of WM microstructure associated with RBD in PD.Materials and Methods
83 PD patients underwent clinical assessments and diffusion tensor image scans with a follow-up time of a mean of 2 years (1-4.5 years). Patients were grouped by (1) PD with RBD (PD-RBD, n=43), (2) PD without RBD (PD-nonRBD, n=40). Tract-based spatial statistics was used to extract the diffusion tensor metrics of WM including fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD). We performed linear mixed-effects (LME) models to examine WM microstructure evolution in PD-RBD and PD-nonRBD, and whether RBD modified WM progression. We additionally explored longitudinal associations between the changes of WM and the progression of clinical symptoms in PD-RBD group.Results
At baseline, clinical information and WM microstructure did not differ significantly between PD-RBD and PD-nonRBD. Longitudinally, PD-RBD showed significantly declined FA metrics over time across numerous regions (PFDR < 0.05). RD and MD metrics within PD-RBD increased within the other broader regions as well (PFDR < 0.05). By contrast, PD-nonRBD experienced decreased FA metrics in more localized regions. Interaction analysis revealed that variations of WM over time significantly differed between PD-RBD and PD-nonRBD for FA metrics in a multitude of regions (PFDR < 0.05), but not AD, RD, and MD. Meanwhile, PD-RBD displayed faster rates of progression within left inferior longitudinal fasciculus (ILF) and uncinate fasciculus (UF) compared with PD-nonRBD. Changes of DTI metrics in some regions were associated with motor symptoms severity (Poriginal < 0.05) in PD-RBD.Conclusions
The presence of RBD may indicate a wider degeneration of WM in PD brain and a faster rate of degeneration in left ILF and UF, and these regions may closely associate with the progression of motor symptoms. These findings provide a better understanding of the impact of RBD on the pathophysiological mechanisms of PD.Acknowledgements
The authors would like to thank all study participants in the current research project.References
1. Hogl, B., A. Stefani, and A. Videnovic, Idiopathic REM sleep behaviour disorder and neurodegeneration - an update. Nat Rev Neurol, 2018. 14(1): p. 40-55.2. Gagnon, J.F., et al., REM sleep behavior disorder and REM sleep without atonia in Parkinson's disease. Neurology, 2002. 59(4): p. 585-9.
3. Pavelka, L., et al., Body-First Subtype of Parkinson's Disease with Probable REM-Sleep Behavior Disorder Is Associated with Non-Motor Dominant Phenotype. J Parkinsons Dis, 2022.
4. Gong, Y., et al., Clinical manifestations of Parkinson disease and the onset of rapid eye movement sleep behavior disorder. Sleep Medicine, 2014. 15(6): p. 647-653.
5. Liu, Y., et al., Longitudinal Changes in Parkinson's Disease Symptoms with and Without
Rapid Eye Movement
Sleep Behavior Disorder: The Oxford Discovery Cohort Study. Movement Disorders, 2021. 36(12): p. 2821-2832.
6. Postuma, R.B., et al., Rapid eye movement sleep behavior disorder and risk of dementia in Parkinson's disease: A prospective study. Movement Disorders, 2012. 27(6): p. 720-726.
7. Fereshtehnejad, S.M., et al., Clinical criteria for subtyping Parkinson's disease: biomarkers and longitudinal progression. Brain, 2017. 140(7): p. 1959-1976.
8. Boeve, B.F., et al., Pathophysiology of REM sleep behaviour disorder and relevance to neurodegenerative disease. Brain, 2007. 130(Pt 11): p. 2770-88.
9. McKenna, D. and J. Peever, Degeneration of rapid eye movement sleep circuitry underlies rapid eye movement sleep behavior disorder. Mov Disord, 2017. 32(5): p. 636-644.
10. Sommerauer, M., et al., Evaluation of the noradrenergic system in Parkinson's disease: an 11C-MeNER PET and neuromelanin MRI study. Brain, 2018. 141(2): p. 496-504.
11. García-Lorenzo, D., et al., The coeruleus/subcoeruleus complex in rapid eye movement sleep behaviour disorders in Parkinson's disease. Brain, 2013. 136(Pt 7): p. 2120-9.
12. Matzaras, R., et al., Brain Neuroimaging of Rapid Eye Movement Sleep Behavior Disorder in Parkinson's Disease: A Systematic Review. J Parkinsons Dis, 2022. 12(1): p. 69-83.
13. Lim, J.S., et al., Neural substrates of rapid eye movement sleep behavior disorder in Parkinson's disease. Parkinsonism Relat Disord, 2016. 23: p. 31-6.
14. Kamps, S., et al., Smaller subcortical volume in Parkinson patients with rapid eye movement sleep behavior disorder. Brain Imaging and Behavior, 2018. 13(5): p. 1352-1360.
15. Yoon, E.J. and O. Monchi, Probable REM sleep behavior disorder is associated with longitudinal cortical thinning in Parkinson's disease. NPJ Parkinsons Dis, 2021. 7(1): p. 19.
16. Filley, C.M., White matter and human behavior. Science, 2021. 372(6548): p. 1265-1266.
17. Ford, A.H., et al., Rapid eye movement sleep behavior disorder in Parkinson's disease: magnetic resonance imaging study. Mov Disord, 2013. 28(6): p. 832-6.
18. Ghazi Sherbaf, F., et al., Microstructural Changes in Patients With Parkinson's Disease Comorbid With REM Sleep Behaviour Disorder and Depressive Symptoms. Frontiers in Neurology, 2018. 9.
19. Mole, J.P., et al., Increased fractional anisotropy in the motor tracts of Parkinson's disease suggests compensatory neuroplasticity or selective neurodegeneration. European Radiology, 2016. 26(10): p. 3327-3335.
20. Kamagata, K., et al., White matter alteration of the cingulum in Parkinson disease with and without dementia: evaluation by diffusion tensor tract-specific analysis. AJNR Am J Neuroradiol, 2012. 33(5): p. 890-5.
21. Minett, T., et al., Longitudinal diffusion tensor imaging changes in early Parkinson’s disease: ICICLE-PD study. Journal of Neurology, 2018. 265(7): p. 1528-1539.
22. Hughes, A.J., et al., Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry, 1992. 55(3): p. 181-4.
23. Katzman, R., et al., A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol, 1988. 41(10): p. 971-8.
24. Shen, S.S., et al., Validation study of REM sleep behavior disorder questionnaire-Hong Kong (RBDQ-HK) in east China. Sleep Med, 2014. 15(8): p. 952-8.
25. Schiess, M.C., et al., Parkinson's disease subtypes: clinical classification and ventricular cerebrospinal fluid analysis. Parkinsonism Relat Disord, 2000. 6(2): p. 69-76.
26. Espay, A.J., Mirror movements in parkinsonism: evaluation of a new clinical sign. Journal of Neurology, Neurosurgery & Psychiatry, 2005. 76(10): p. 1355-1359.
27. Smith, S.M., et al., Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage, 2006. 31(4): p. 1487-1505.
28. Koch, K., et al., Diffusion tensor imaging (DTI) studies in patients with obsessive-compulsive disorder (OCD): a review. J Psychiatr Res, 2014. 54: p. 26-35.
29. Harsan, L.A., et al., Brain dysmyelination and recovery assessment by noninvasive in vivo diffusion tensor magnetic resonance imaging. J Neurosci Res, 2006. 83(3): p. 392-402.
30. Song, S.K., et al., Demyelination increases radial diffusivity in corpus callosum of mouse brain. Neuroimage, 2005. 26(1): p. 132-40.
31. Hua, K., et al., Tract probability maps in stereotaxic spaces: Analyses of white matter anatomy and tract-specific quantification. NeuroImage, 2008. 39(1): p. 336-347.
32. Postuma, R.B., et al., REM sleep behavior disorder and neuropathology in Parkinson's disease. Mov Disord, 2015. 30(10): p. 1413-7.
33. Ansari, M., et al., Brain pathway differences between Parkinson's disease patients with and without REM sleep behavior disorder. Sleep Breath, 2017. 21(1): p. 155-161.
34. Ghazi Sherbaf, F., et al., Microstructural changes in patients with Parkinson disease and REM sleep behavior disorder: depressive symptoms versus non-depressed. Acta Neurol Belg, 2018. 118(3): p. 415-421.
35. Patriat, R., et al., White matter microstructure in Parkinson's disease with and without elevated rapid eye movement sleep muscle tone. Brain Commun, 2022. 4(2): p. fcac027.
36. Bugalho, P. and M. Viana-Baptista, REM sleep behavior disorder and motor dysfunction in Parkinson's disease – A longitudinal study. Parkinsonism & Related Disorders, 2013. 19(12): p. 1084-1087.
37. Niida, R., et al., Aberrant Anterior Thalamic Radiation Structure in Bipolar Disorder: A Diffusion Tensor Tractography Study. Front Psychiatry, 2018. 9: p. 522.
38. Radwan, A.M., et al., An atlas of white matter anatomy, its variability, and reproducibility based on constrained spherical deconvolution of diffusion MRI. Neuroimage, 2022. 254: p. 119029.
39. Almairac, F., et al., The left inferior fronto-occipital fasciculus subserves language semantics: a multilevel lesion study. Brain Struct Funct, 2015. 220(4): p. 1983-95.
40. Ye, G., et al., Evolution patterns of probable REM sleep behavior disorder predicts Parkinson's disease progression. NPJ Parkinsons Dis, 2022. 8(1): p. 36.
41. Bach, M., et al., Methodological considerations on tract-based spatial statistics (TBSS). Neuroimage, 2014. 100: p. 358-69.
42. Raffelt, D.A., et al., Connectivity-based fixel enhancement: Whole-brain statistical analysis of diffusion MRI measures in the presence of crossing fibres. Neuroimage, 2015. 117: p. 40-55.
Figures
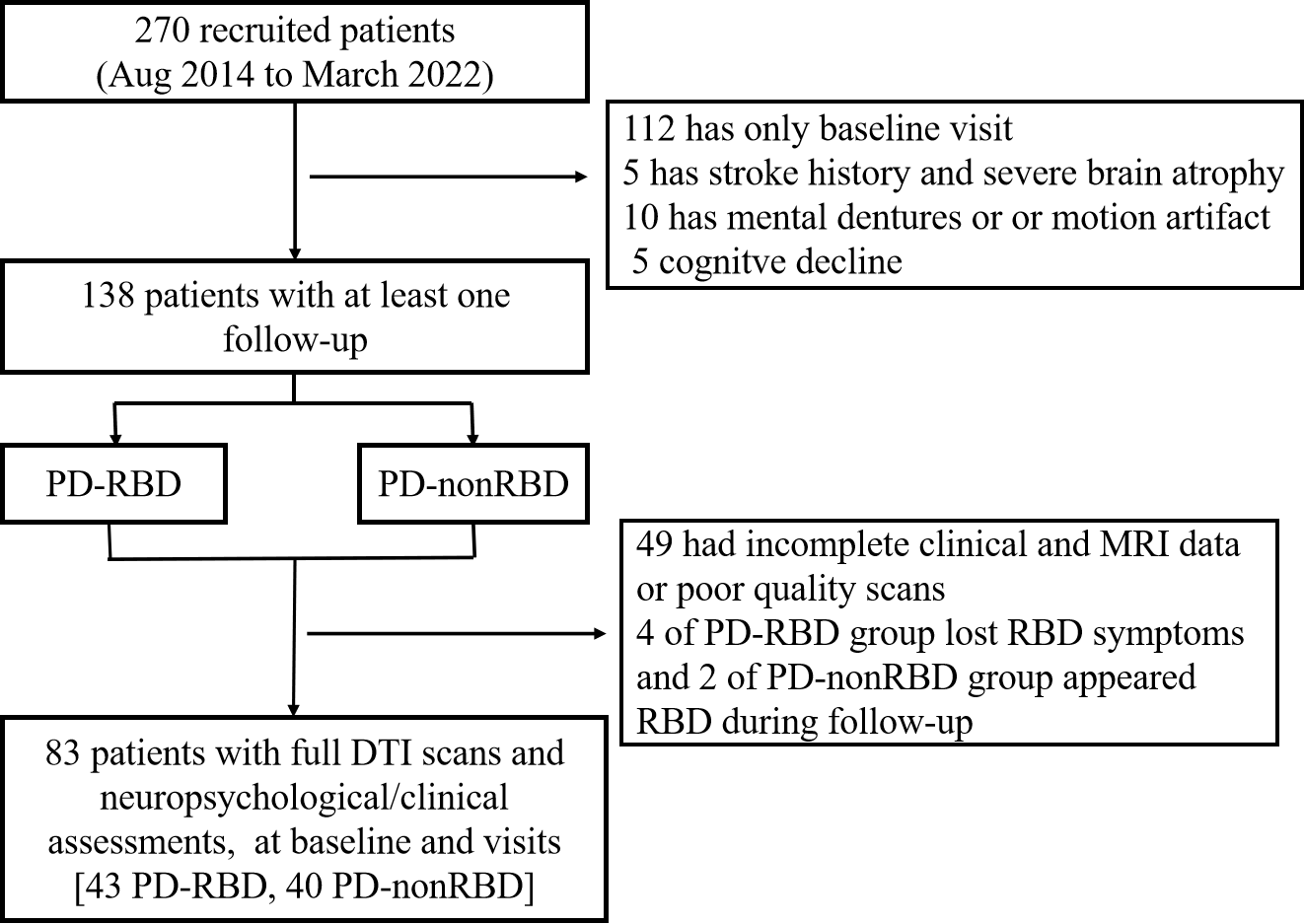
Figure 1. Participants recruitment and selection.
Abbreviations: PD = Parkinson’s disease; RBD = rapid eye movement sleep behavior disorder; PD-nonRBD = PD without RBD; PD-RBD = PD with RBD.
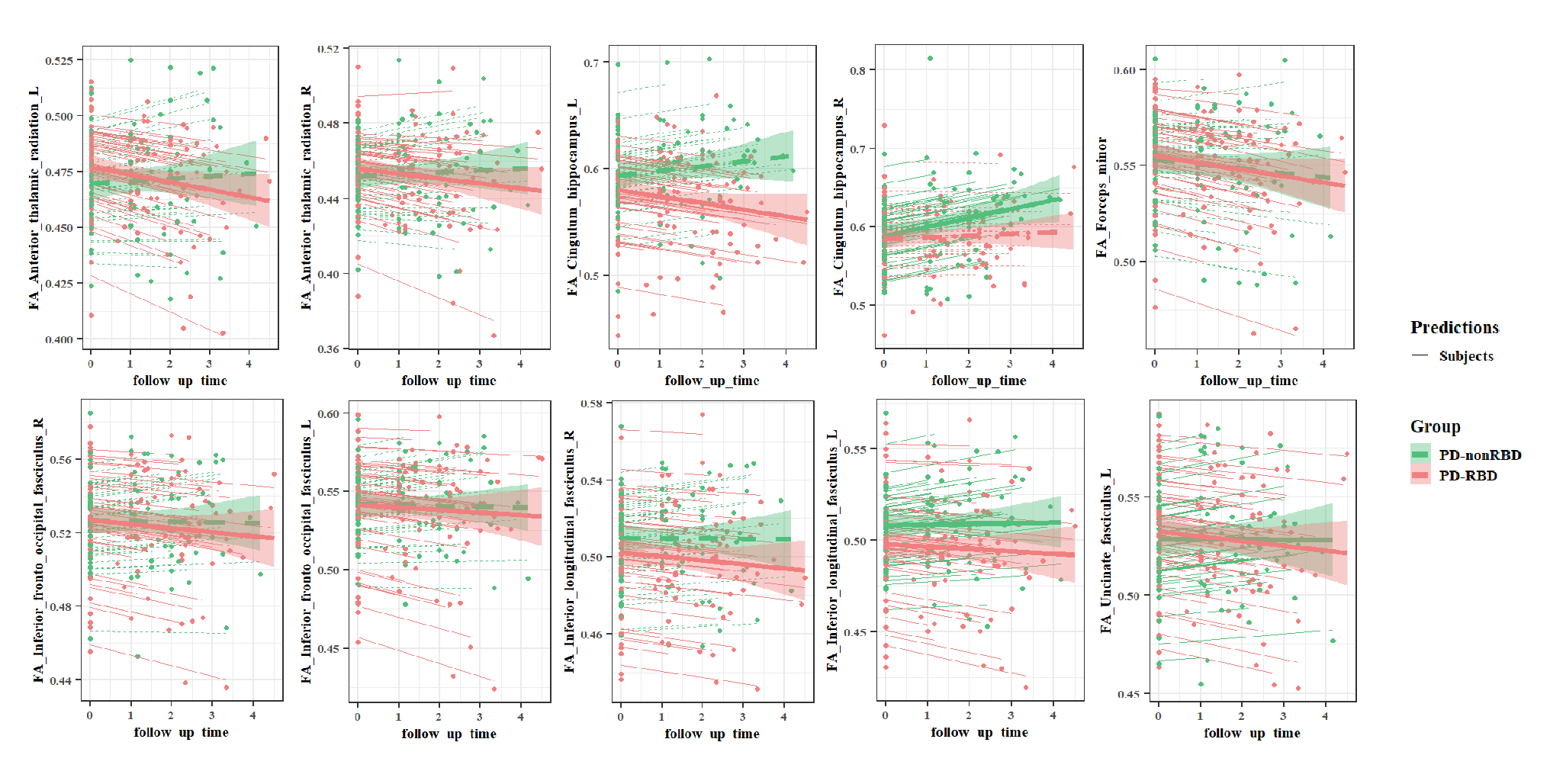
Figure 2. Longitudinal changes of WM regions in FA over time in PD-RBD and PD-nonRBD group and the interaction effect between groups.
Red lines and red dots represent PD-RBD; green lines and green dots represent PD-nonRBD. Bold lines represent the group level. Thin lines represent the individual level based on fit of linear mixed model. Dotted line means no significant effects of time on follow-up time. Abbreviations: WM = white matter microstructure; tp = temporal lobe part;FA = fractional anisotropy.
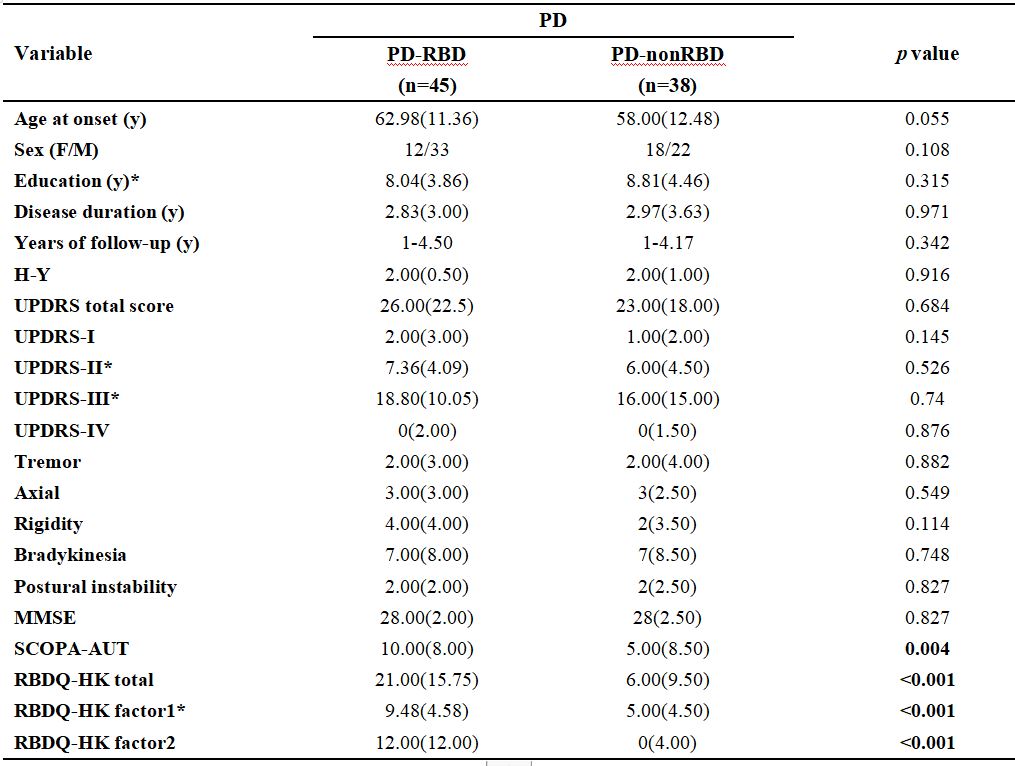
Table 1. Demographic and clinical data of Parkinson’s disease patients at baseline.
Values are expressed as mean (standard deviation) for continuous variables and numbers for gender. *: Except for variables marked with an asterisk,other variables with non-Gaussian distribution are expressed as median (interquartile range). Significant results are indicated in bold.
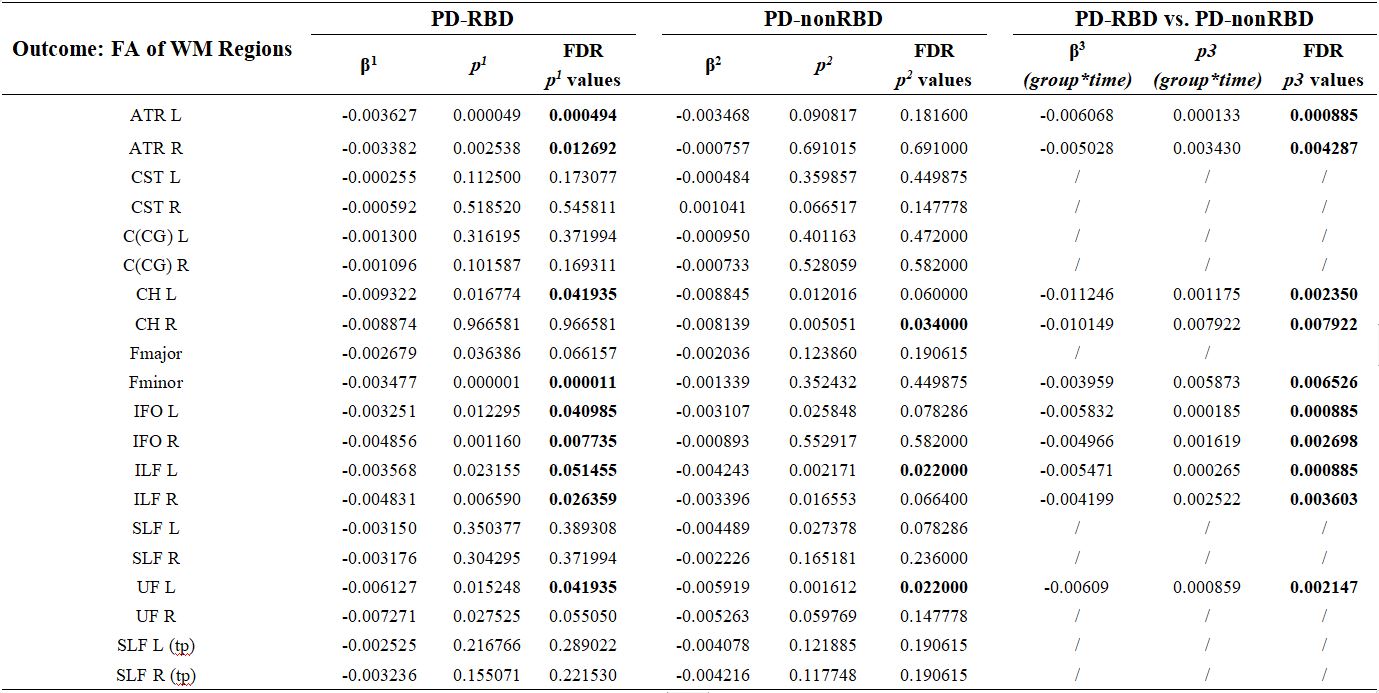
Table 2. Longitudinal changes of WM regions in FA over time in PD-RBD and PD-nonRBD group and the interaction effect between groups.
The table shows longitudinal changes of FA in WM regions in PD-RBD and PD-nonRBD and interaction between groups by linear mixed effects model (LME). Group*time means the effect of time on different WM regions depending on groups.
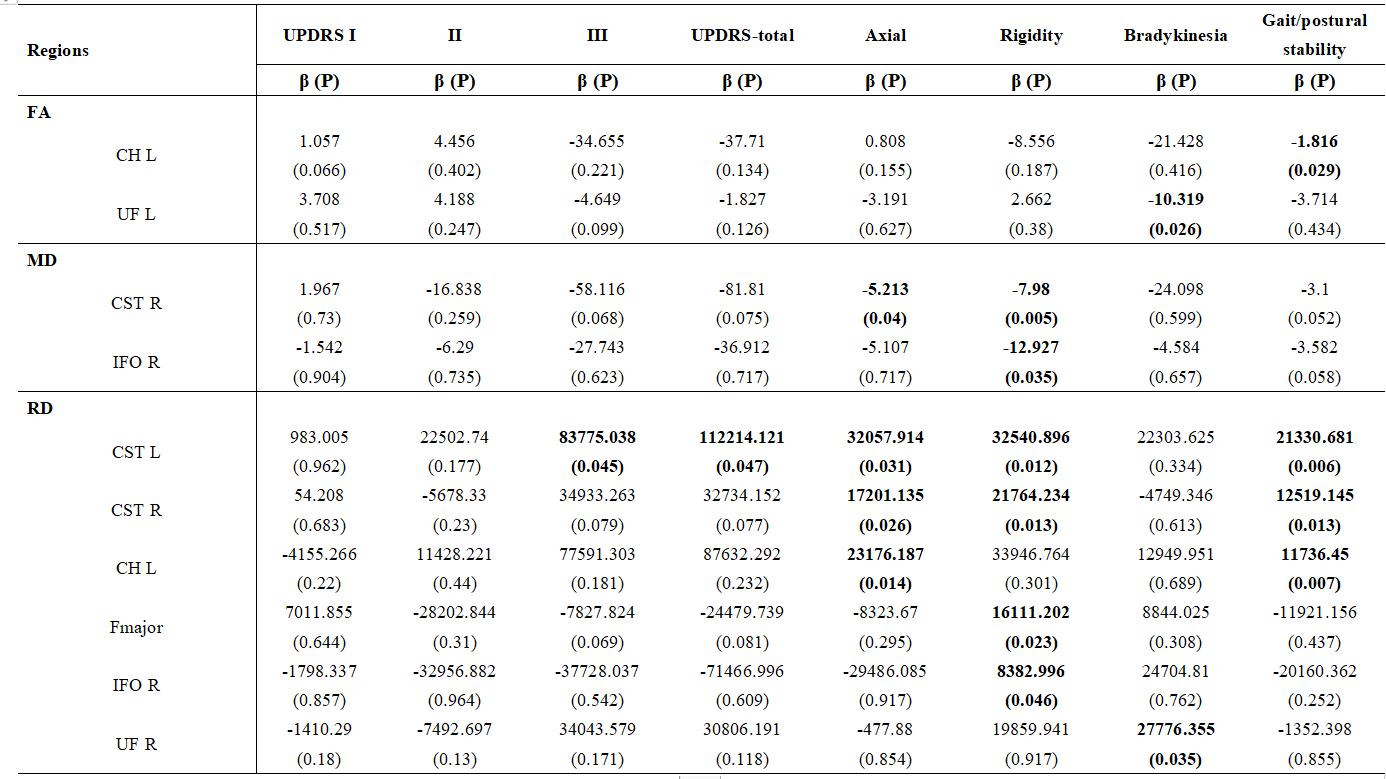
Table 3. Longitudinal associations between changes of progressive clinical data and WM regions in PD-RBD group.
The table shows the associations between the changes of progressive clinical data and WM regions over follow-up time in PD-RBD group. Values are expressed as β (P). Significant results are indicated in bold.