2341
Measuring tract specific intramedullary damage level with 3D lesion segmentations following spinal cord injury1Spinal Cord Injury Center, Balgrist University Hospital, University of Zurich, Zurich, Switzerland, 2Department of Information Technology and Electrical Engineering, ETH Zurich, Zurich, Switzerland, 3Department of Neurophysics, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany, 4Wellcome Trust Centre for Neuroimaging, UCL Institue of Neurology, University College, London, United Kingdom
Synopsis
Keywords: Spinal Cord, Spinal Cord, Clinical Trial
Motivation: Assessing the extent of intramedullary lesion after traumatic spinal cord injury (tSCI) has been shown to correlate with the severity of tSCI. We expand this approach, by understanding the injury's impact on individual spinal tracts and evaluating its connection to clinical severity.
Goal(s): To fully characterize the extent of injury to the ascending and descending tracts on T2-weighted sagittal scans.
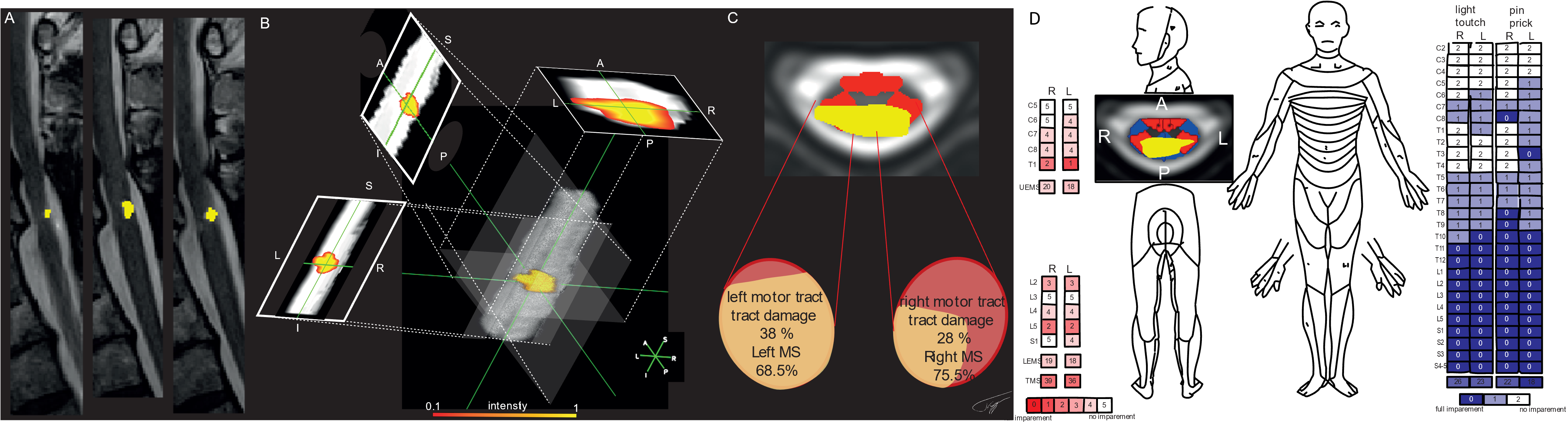
Approach: We achieve this by manually delineating the lesion based on T2w-sagittal scans, projecting it into three planes, enabling 3D-visualization.
Results: Significant correlations between damage to the left- and right-descending tracts, right-ascending tract and tract-associated clinical scores were found, indicating clinical validity.
Impact: 3D-lesion characterization allows tract-specific analysis in traumatic SCI patients. It allows a precise assessment of injury to specific tracts on both sides of the spinal cord. This approach can inform tailored treatment and rehabilitation strategies.
Introduction
Traumatic spinal cord injury (tSCI) has devastating clinical consequences1. SCI leads to irreversible axonal fiber degeneration, demyelination, and cellular apoptosis in the spinal tracts2. Spontaneous regeneration of interrupted fiber tracts remains limited due to the complex underlying mechanisms of pathophysiology and degeneration. Therefore, there is a growing demand for clinically accurate biomarkers to assess the injury severity and reveal the impact of injury induced damage. MRI is a commonly used method to assess the extent of the lesion formed after injury3. Thus far most neuroimaging biomarkers for tSCI e.g., Midsagittal Tissue Bridges (TB)4–7 or BASIC8 score have involved two-dimensional evaluations of the lesion conducted on sagittal and axial MRI scans. TB defined as the spared-tissue which combines ventral and dorsal white-matter (WM) tracts, revealed correlations with motor and sensory clinical scores However, motor tracts are largely located in the lateral WM columns while sensory tracts are located in the dorsal and lateral WM columns. TB therefore lack lateral specificity, thus failing to provide a complete representation of the injury's impact on the patient’s sensory and motor skills. WM tracts can be categorized as ascending (for sensory information) and descending (for motor information)9. This classification aligns with the International Standards for Neurological Classification of SCI (ISNCSCI) Worksheet, a standard clinical assessment of sensory and motor function post-tSCI. The method presented here offers a comprehensive approach to a specific analysis of ascending and descending WM tracts affected by the injury. It provides a three-dimensional assessment of the lesion, enhancing our understanding of the injury extent without the need for additional MRI scans.Methods
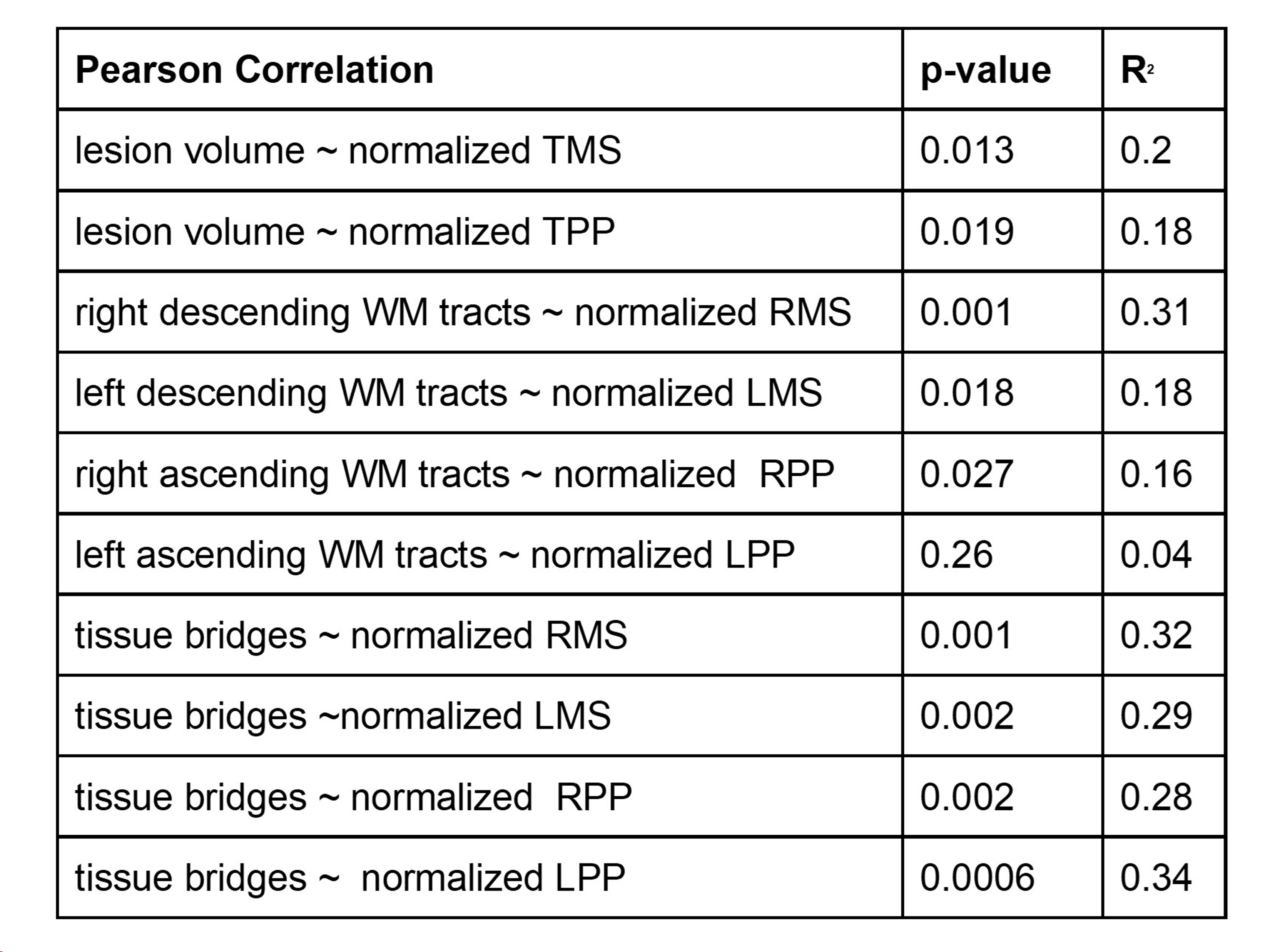
Thirty-three SCI patients, from the double-blind, placebo-controlled Nogo Inhibition in Spinal Cord Injury trial (NISCI), with cervical tSCI, underwent sagittal T2w-MRI 6 months post-injury10. Patients included in this analysis were part of the placebo-treated group recruited in eight European Trauma centers. To gain a comprehensive understanding of the lesion's influence on spinal cord WM tracts, we projected the binary lesion volume segmentation into axial, coronal, and sagittal planes, resulting in a glass-spine view with spatial shadowing of the lesion. Voxel values denote the lesion's extent in the third dimension through-plane. To evaluate the specific WM tract damage (i.e. percentage of overlap of lesion and WM tracts) in the axial plane, we created masks of the left and right ascending and descending WM tracts from the PAM50 atlas. The lesion volume was assessed manually by blinded rater using Jim (version 7.0) on each sagittal slice11. The spinal cord was automatically segmented using a deep learning algorithm, the model_seg_sci algorithm12. Lesion volume, spinal cord and WM-tract masks were analyzed in the PAM50 space after coregistration with the PAM50 template. Data analysis was performed using bespoke Matlab (2020b)13. We performed a Pearson correlation analysis with normalized clinical scores to assign the correlations. Normalization was done by dividing the patient’s clinical scores below the lesion level by the maximum possible score.Results
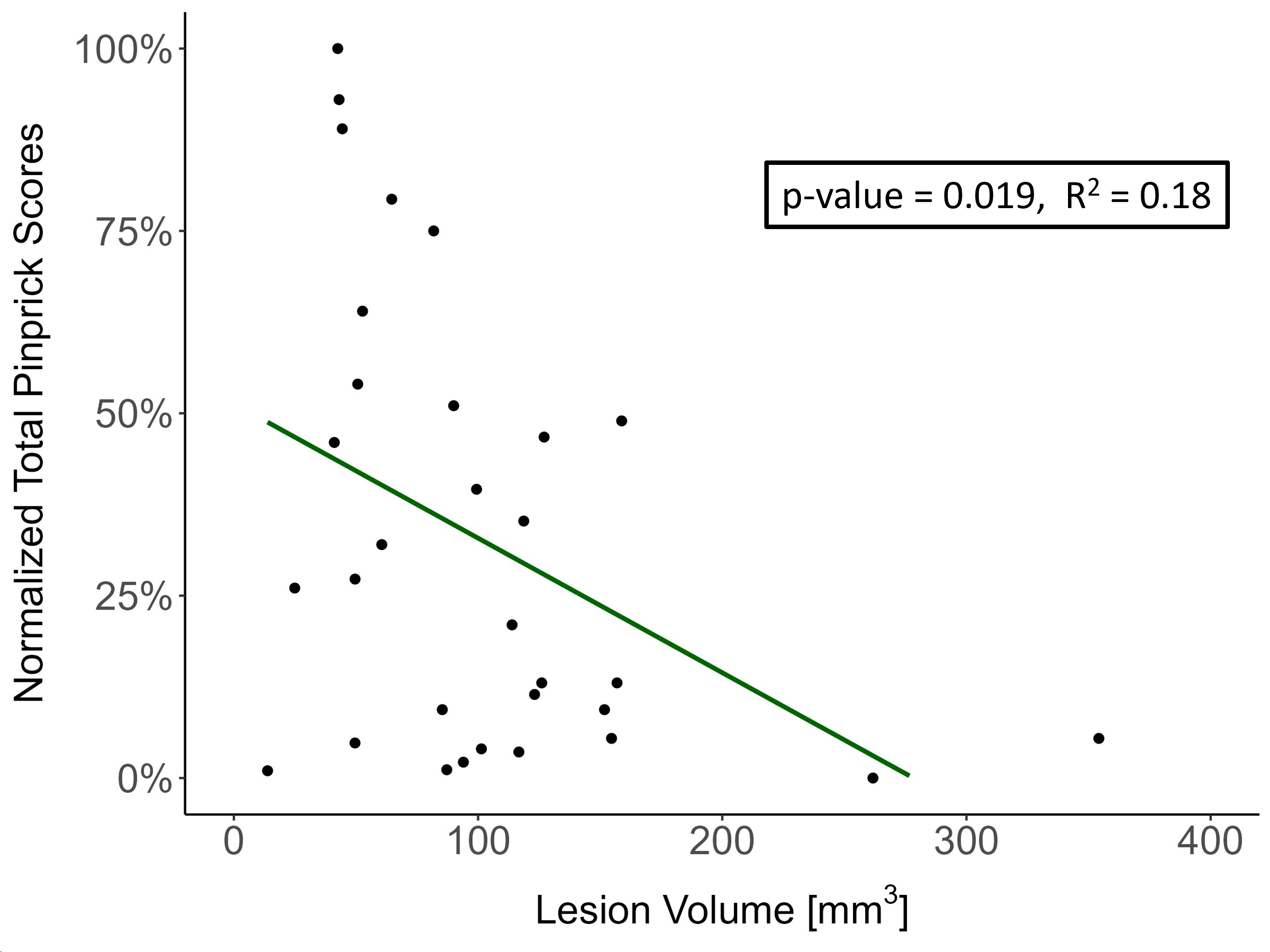
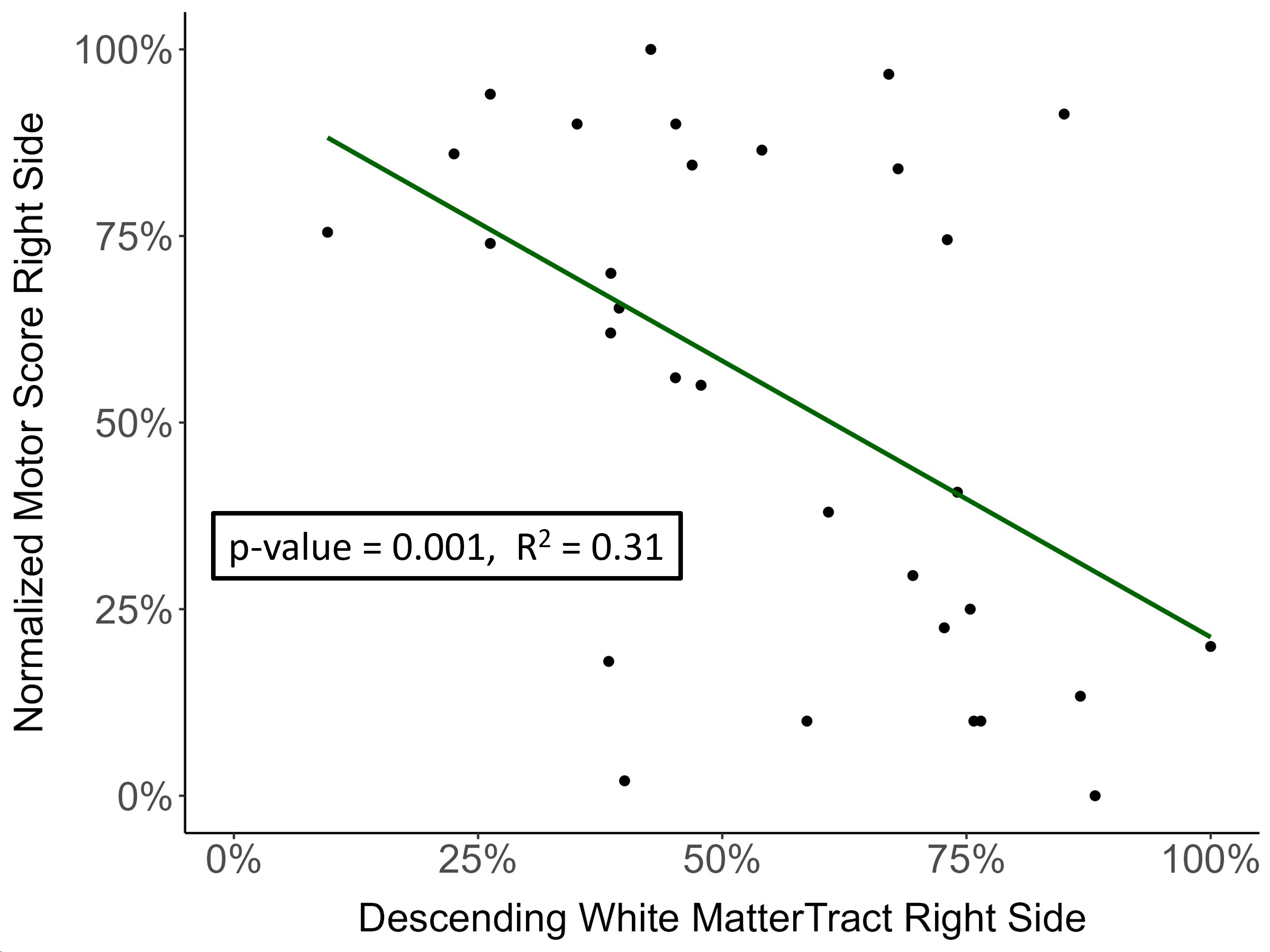
Figure 1 shows a patient example and the glass-spine view with a spatial shadowing of the lesion projected into the sagittal, axial and coronal planes. The Pearson correlation analysis can be found in Table 1 and Figure 1&2.Discussion
The 3D-lesion assessment, with its information on sagittal, axial and coronal planes, provides unique insights into the expansion of the lesion. Our findings indicate lesion volume to be a valid biomarker for SCI, as it correlates with commonly assessed clinical scores. Additionally, we've demonstrated that projecting sagittal lesion segmentations into the axial plane allows analysis of ascending and descending WM tracts without the need for extra MRI scans. This can provide crucial information for patients and physicians at no additional inconvenience for the patient. However, TB remain a more effective factor in explaining the variance in the correlation analysis compared to the WM tract analysis. However, it's important to note that unlike the method described herein, TB encompass both left and right motor and sensory tracts measured on one midsagittal slice. As a result, it fails to capture the complete extent of the lesion and lacks specificity. In the acute phase, the assumption of 2D-lesion analysis of an ovoid shape becomes inadequate. Future work will focus on the early stage following SCI where 3D-WM tract-specific analysis may yield more clinically relevant insights e.g. correlation of damage extent and location and recovery potential.Conclusion
We introduced a 3D-lesion assessment based on T2w-sagittal MRI as a potential biomarker for SCI. The WM tract-specific analysis revealed significant correlations with clinical scores. This method holds promise for enabling individualized treatment options for spinal cord injury patients.Acknowledgements
We thank all collaborating radiologists and radiographers and clinicians at the clinical and research sites across this multicenter study for their help and contribution to the current study. Moreover thanks to patients for their time and contribution.
Funding: This project has received funding from the European Union's Horizon 2020 research and innovation programme under the grant agreement No 681094 and is supported by the Swiss State Secretariat for Education, Research and Innovation (SERI) under contract number 15.0137. PF received funding from Eccellenza fellowship/181362 by SNSF. Moreover, MS receives funds from Wings for life charity (No WFL-CH-19/20) and grants from International Foundation for Research (IRP-2022-01-158).
References
1. Ahuja, C. S. et al. Traumatic spinal cord injury. Nature Reviews Disease Primers vol. 3 Preprint at https://doi.org/10.1038/nrdp.2017.18 (2017).
2. Cadotte, D. W. & Fehlings, M. G. Spinal cord injury: A systematic review of current treatment options. in Clinical Orthopaedics and Related Research vol. 469 732–741 (2011).
3. Freund, P. et al. MRI in traumatic spinal cord injury: from clinical assessment to neuroimaging biomarkers. The Lancet Neurology vol. 18 1123–1135 Preprint at https://doi.org/10.1016/S1474-4422(19)30138-3 (2019).
4. Pfyffer, D., Vallotton, K., Curt, A. & Freund, P. Tissue bridges predict neuropathic pain emergence after spinal cord injury. J Neurol Neurosurg Psychiatry 91, 1111–1117 (2020).
5. Pfyffer, D., Huber, E., Sutter, R., Curt, A. & Freund, P. Tissue bridges predict recovery after traumatic and ischemic thoracic spinal cord injury. Neurology 93, E1550–E1560 (2019).
6. Huber, E., Lachappelle, P., Sutter, R., Curt, A. & Freund, P. Are Midsagittal Tissue Bridges Predictive of Outcome After Cervical Spinal Cord Injury? doi:10.1002/ana (2017).
7. Smith, A. C. et al. Lateral Corticospinal Tract Damage Correlates With Motor Output in Incomplete Spinal Cord Injury. Arch Phys Med Rehabil 99, 660–666 (2018).
8. Talbott, J. F. et al. The Brain and Spinal Injury Center score: A novel, simple, and reproducible method for assessing the severity of acute cervical spinal cord injury with axial T2-weighted MRI findings. J Neurosurg Spine 23, 495–504 (2015).
9. Craven, J. Major ascending and descending tracts in the spinal cord (2010).
10. Kucher, K. et al. First-in-man intrathecal application of neurite growth-promoting anti-nogo- a antibodies in acute spinal cord injury. Neurorehabil Neural Repair 32, 578–589 (2018).
11. Jim 7.0; Leicester, UK; http://www.xinapse.com
12. model_seg_sci, https://github.com/ivadomed/model_seg_sc
13. MATLAB. (2020b). Natick, Massachusetts: The MathWorks Inc
Figures