2338
Repeatability and Reproducibility of Ultra High-Field Cervical Spinal Cord Quantitative MRI: A Dual-Center Study at 7T1University of Zurich, Zurich, Switzerland, 2Department of Neurophysics, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany, 3Aix-Marseille Univ, CNRS, CRMBM, Marseille, France, 4APHM, Hopital Universitaire Timone, CEMEREM, Marseille, France, 5Siemens Healthcare SAS, Saint-Denis, France, 6Department of Physics, Norwegian University of Science and Technology, Trondheim, Norway
Synopsis
Keywords: Spinal Cord, High-Field MRI, UHF 7T, Spinal Cord, qMRI, reproducibility
Motivation: Conducting multi-center 7T quantitative MRI studies on the spinal cord requires acquisition protocols with high reliability.
Goal(s): To provide a consensus cervical cord qMRI protocol with high reliability by means of determining its repeatability and reproducibility across a dual center test-retest study.
Approach: Six healthy controls underwent a multiparametric protocol back-to-back 3 times with a break, which include T1-MP2RAGE and T2*-weighted on two 7T scanners.
Results: T1 values and spinal cord area (on C1-C5 level) show high repeatability (CoV<2%; Cov <1.2% respectively and high reproducibility (Cov<2.6%; <9.9% respectively) within and between subjects.
Impact: This work represents an important step towards the adoption of UHF MRI protocol for various neurological pathologies affecting the spinal cord. It empowers neurologists and scientists investigating neurodegenerative diseases with high reliability and robustness.
Introduction
Ultra-high field (UHF) MRI such as 7T MP2RAGE and T2*-weighted MRI recently proposed in the cervical cord (SC)with increased SNR, resolution and high reproducibility 1,2. These sequences provide quantitative parameters with higher sensitivity to tract-specific macro- and microstructural changes (atrophy, demyelination, and axonal degeneration). They consequently enable us to determine the spatiotemporal underlying pathophysiology of the neurodegeneration in different pathologies impacting the cervical cord with higher accuracy. In theory, qMR readouts are insensitive to differences in MR software and hardware and thereby increase the comparability across different time points and sites3–7. Thus, qMRI is considered as a potential biomarker in multi-center clinical trials8. Yet, 7T SC qMRI is challenging, demanding a reproducible and standardized protocol. Our study therefore establishes a consensus protocol for a 7T SC qMRI, focusing on tissue macro and microstructure, while assessing repeatability and reproducibility via a dual-center test-retest study. This can result in a major contribution to the diagnostic workup of the patients with pathologies impacting SC.Materials and Methods
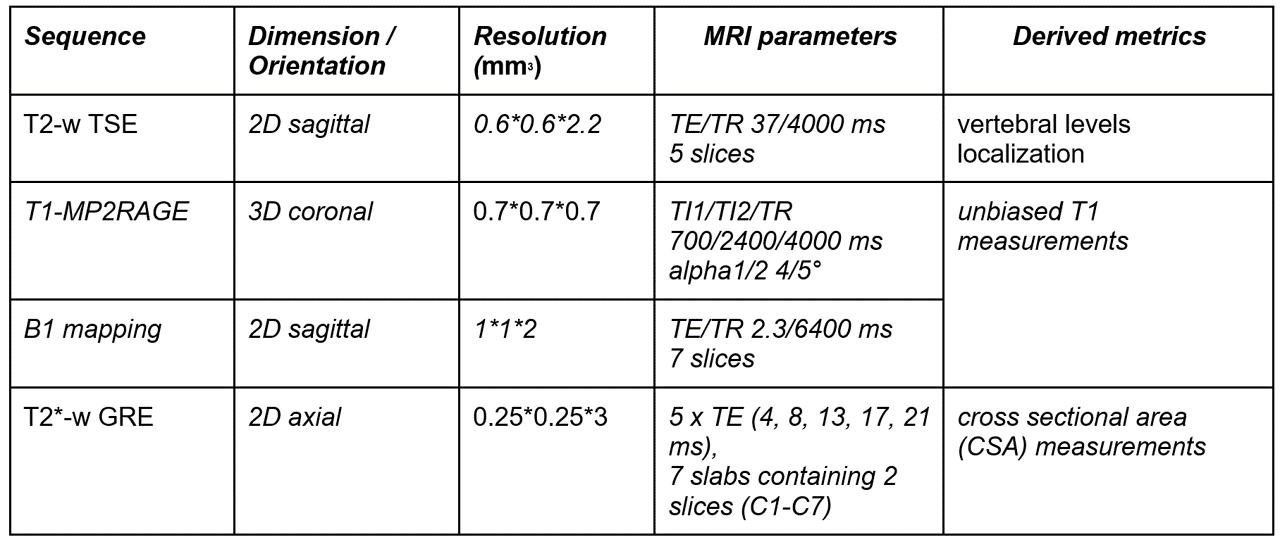
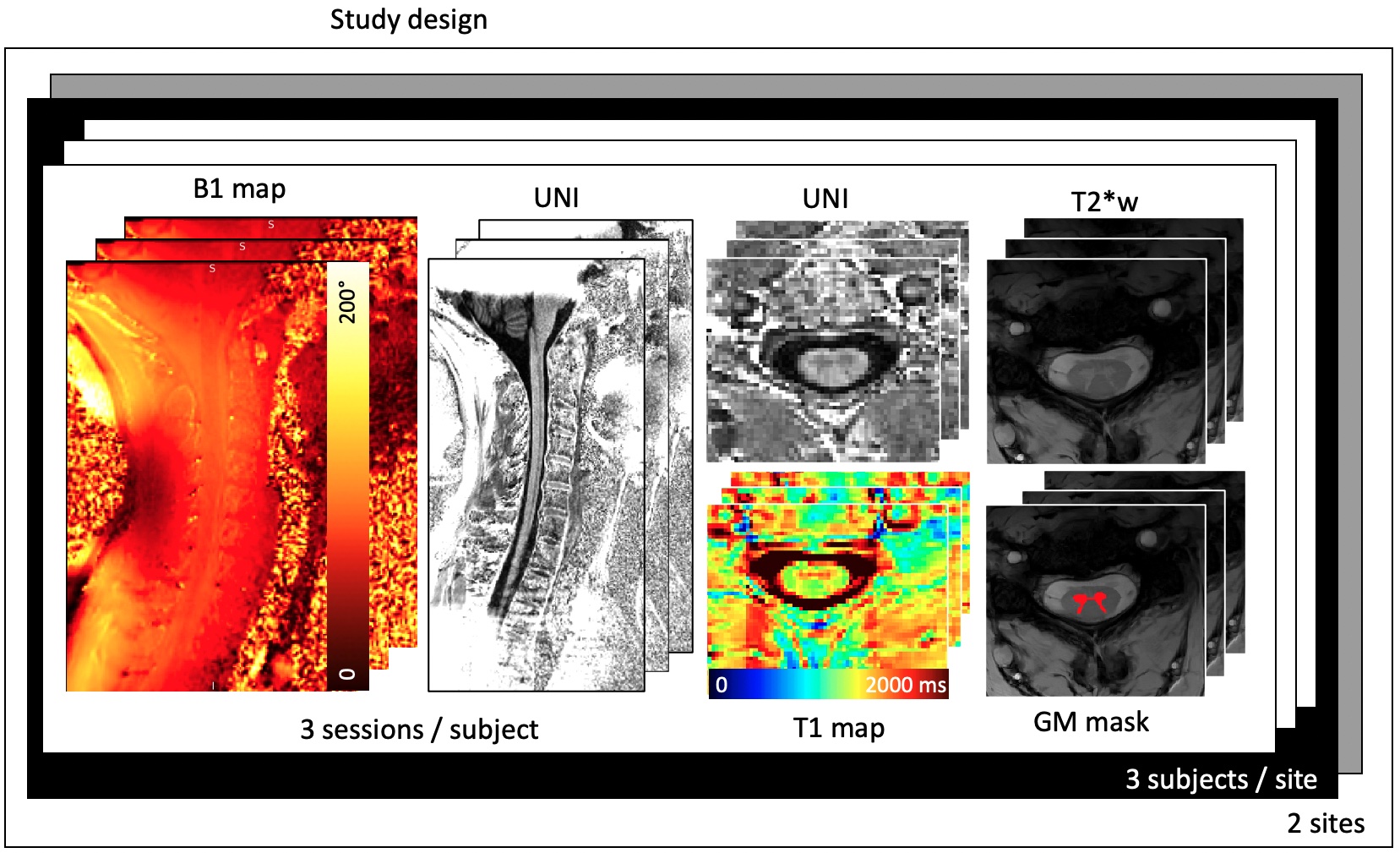
MRI measurements: A multiparametric qMRI protocol was tailored including B1-map, 3D MP2RAGE, and multi slab axial T2*-weighted GRE based on previous work1 Fig(1). Acquisitions were conducted on two 7T MR systems (Terra, VE12U, Siemens Healthcare) at two different centers in France and Switzerland, using an 8Tx/8Rx cervical spinal cord coil array (Rapid Biomedical), with the 8Tx channels combined into a single Tx mode. In total 6 healthy subjects (3 subjects per site (age mean±SD 29.5±3.1, 2 females) underwent the qMRI protocol for 3 times with a break in the range of 1 hour to one week.Image processing: Data processing was performed using an in-house pipeline. Unbiased T1 maps were generated using B1+ correction method proposed by1, cord segmentation and registration to the PAM50 template9 were performed to extract T1 values from different white matter tracts (e.g., corticospinal tract, dorsal column, lateral sensory tract) and gray matter horns (e.g. dorsal horn and ventral horns). White and gray matter (WM/GM) automatic segmentations for Cross Sectional Area (CSA) measurements were performed on the T2*-weighted images using a recently developed approach dedicated to 7T SC with high spatial resolution (sct_deepseg –task seg_gm_sc_7t_t2star) [Medina et al., 2022]. Statistical analysis: Repeatability (intra-subject variability) was estimated using the coefficient of variation (COV%), for each MRI metric, per cord level (C1-C7). Within-subject COV was calculated by the standard deviation over the mean across the three scanning sessions for each subject. Reproducibility (inter-subject variability) was assessed by calculating the COV across 6 subjects for the total spinal cord (averaged across levels). Statistical analysis was performed using R software (version 4.3.1)Results
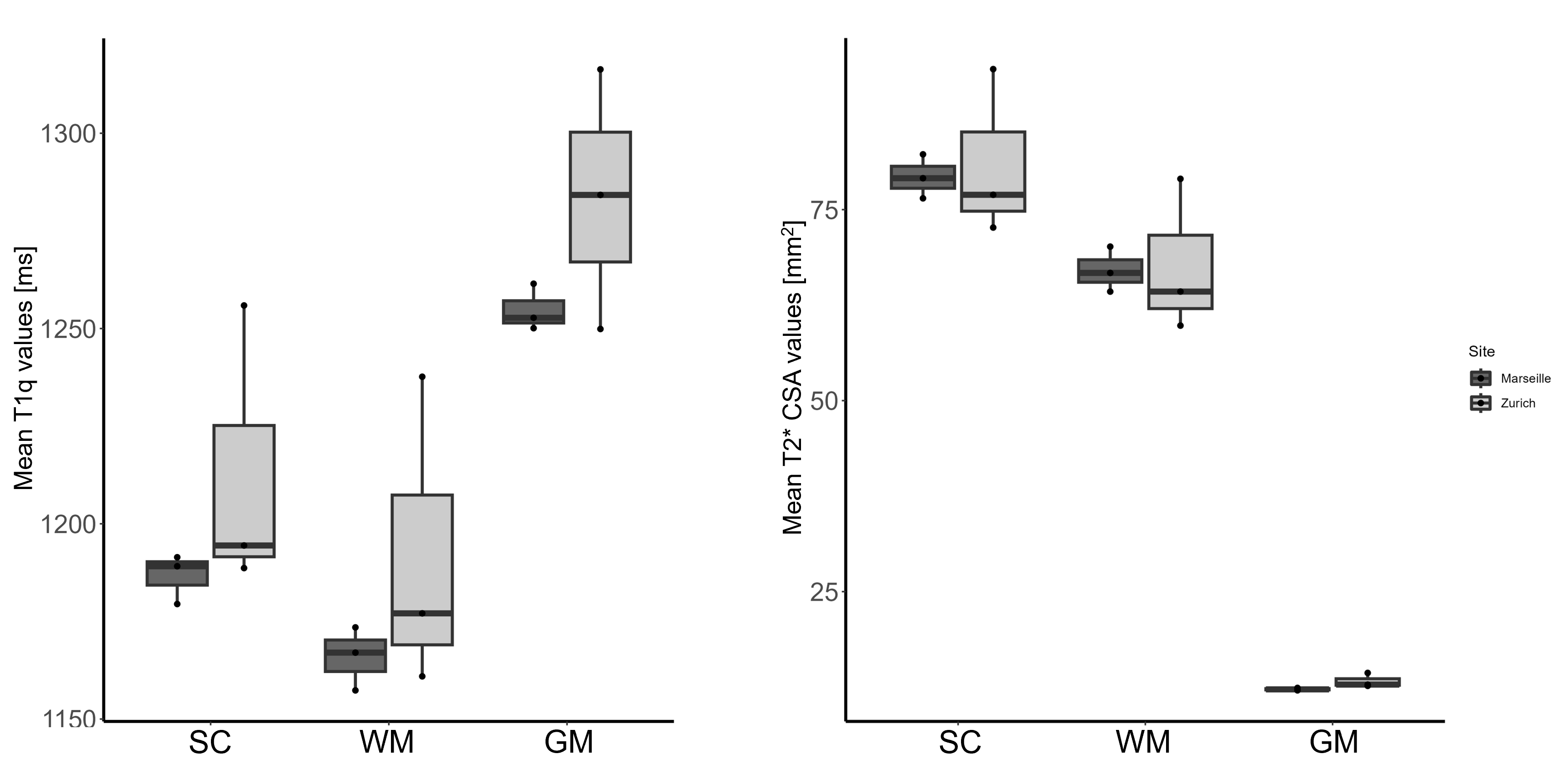
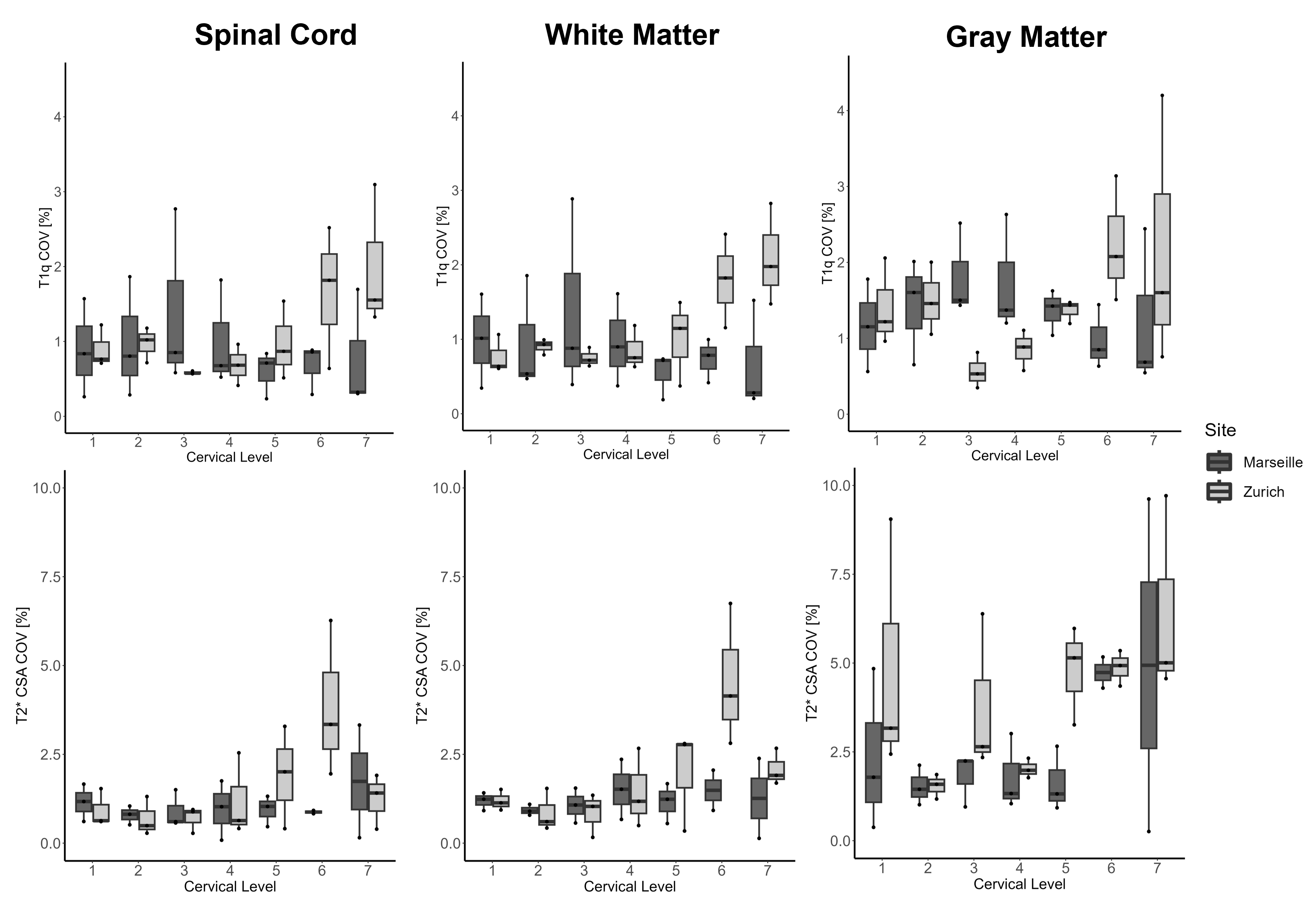
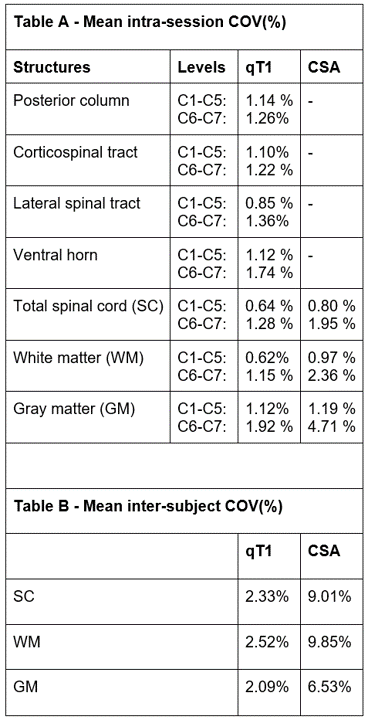
The study design and representative B1 and T1 maps, MP2RAGE-UNI images, as well as axial T2*-w images are shown in (Fig. 2). Figure 3&4 show the mean T1 and CSA values across levels and the box plots of the repeatability COVs of the T1 and CSA values per level (C1-C7) respectively per site. Figure 5 reports the COVs of repeatability (within-subject variability) averaged per levels (upper, C1-C5) and (lower, C6-C7) for each of the ROI (Table A) and the mean COVs for reproducibility (between-subjects variability) across 6 subjects averaged across levels (table B). One subject in Zurich presented with SAR limitatio, accidentally scanned using maximal voltage setup for RF power (reaching clipping values for all of the 3 sessions). Consequently, true B1 map could not be determined, which resulted in biased T1 map meaning higher T1 values, hence reducing the inter-subject reproducibility (Fig. 5B) while keeping a high repeatability, (Fig.4).Discussion and Conclusion
This dual-center study resulted in to a robust 7T SC qMRI consensus protocol that enables to generate T1 and CSA measures sensitive to macro and microstructural tissue integrity with high repeatability and good reproducibility (<1.1% and <2.5%, respectively, for T1 values, and <2.5% and <10% for CSA). Mean values and intra/inter-subject COVs were in line with previous reports applying similar qMRI techniques in a single center1. Mean intra-subject T1 COVs of the lower part of the cord (C6-C7) were found higher than upper part (C1-C5 levels) due to shimming quality and physiological motion. The higher COVs in CSA (at C1, and C6-C7) are sourced in slice positioning (anatomical variations are greater on these levels). This protocol will be provided to on-going international multi-center study with pioneers in the field. This work represents an important step towards the adoption of UHF MRI protocol for future studies investigating the microstructural underlying mechanism with high resolution and reliability in different neurodegenerative pathologies impacting spinal cord.Acknowledgements
We would like to thank all the healthy volunteers for their time and all the people involved on the on-going multicentre trial. This work is based on methodological developments performed at the Centre de Résonance Magnétique Biologique et Médicale, CRMBM, Aix-Marseille University/CNRS, Marseille, France, and experiments performed at the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zürich and at the Centre d’Exploration Métabolique par Résonance Magnétique, CEMEREM, APHM, Timone Hospital, Marseille, France. A special thank goes to Olivier Girard for his help with sequence management.
Funding: MS received grants from Wings For Life Charity (No. WFL-CH-19/20), grants from International Foundation for Research (IRP-158), and Hurka Foundation 2022-2024. VC received grants from ARSEP (Fondation pour l’Aide à la Recherche sur le Sclérose en Plaques), ANR (Agence Nationale de la Recherche) and CNRS (Centre National de la Recherche Scientifique).PF received funding from Eccellenza fellowship/181362 by SNSF.
References
1- Massire, A. et al. High-resolution multi-parametric quantitative magnetic resonance imaging of the human cervical spinal cord at 7T. Neuroimage 143, 58–69 (2016).
2. Massire, A., Rasoanandrianina, H., Guye, M. & Callot, V. Anterior fissure, central canal, posterior septum and more: New insights into the cervical spinal cord gray and white matter regional organization using T1 mapping at 7T. Neuroimage205, 116275 (2020).
3. Weiskopf, N., Edwards, L. J., Helms, G., Mohammadi, S. & Kirilina, E. Quantitative magnetic resonance imaging of brain anatomy and in vivo histology. Nature Reviews Physics vol. 3 570–588 Preprint at https://doi.org/10.1038/s42254-021-00326-1 (2021).
4. Edwards, L. J., Kirilina, E., Mohammadi, S. & Weiskopf, N. Microstructural imaging of human neocortex in vivo. Neuroimage (2018) doi:10.1016/j.neuroimage.2018.02.055.
5. Freund, P. et al. MRI in traumatic spinal cord injury: from clinical assessment to neuroimaging biomarkers. Lancet Neurol (2019) doi:10.1016/S1474-4422(19)30138-3.
6. Voelker, M. N. et al. The traveling heads 2.0: Multicenter reproducibility of quantitative imaging methods at 7 Tesla. Neuroimage 232, (2021).
7. Seif, M. et al. Reliability of multi-parameter mapping (MPM) in the cervical cord: A multi-center multi-vendor quantitative MRI study. Neuroimage 264, 119751 (2022).
8. Seif, M., Gandini Wheeler-Kingshott, C. A., Cohen-Adad, J., Flanders, A. E. & Freund, P. Guidelines for the conduct of clinical trials in spinal cord injury: Neuroimaging biomarkers. Spinal Cord 57, 717–728 (2019).
9. De Leener, B. et al. PAM50: Unbiased multimodal template of the brainstem and spinal cord aligned with the ICBM152 space. Neuroimage 165, 170–179 (2018).
Figures