2337
Correction of breathing-induced dynamic field changes in the cervical cord using FID navigators at 3T1Spinal Cord Injury Center, Balgrist University Hospital, Zurich, Switzerland, 2Radiology, Harvard Medical School, Boston, MA, United States, 3Computational Radiology Laboratory, Boston Children's Hospital, Boston, MA, United States, 4Siemens Medical Solutions USA Inc., Boston, MA, United States, 5Advanced Clinical Imaging Technology Group, Siemens Healthcare International AG, Lausanne, Switzerland, 6Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 7LTS5, Ecole Polytechnique Fédérale de Lausanne, Lausanne, Switzerland, 8Department of Neurophysics, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany
Synopsis
Keywords: Spinal Cord, Spinal Cord
Motivation: To correct breathing-induced field fluctuations and ensuing artifacts on T2*-weighted MRI of the cervical cord to improve T2* mapping.
Goal(s): To characterize B0 field changes caused by respiration within the cervical cord and to retrospectively compensate for those spatiotemporal fluctuations using a FID navigator-based correction technique.
Approach: B0 field coefficients up to second order were measured using FID navigators and a multi-channel low-resolution reference image. Retrospective correction was performed using measured field coefficients during an iterative image reconstruction.
Results: The FIDnav framework characterized the B0 field changes and improved the quality of T2*-weighted MRI and T2* maps by correcting respiratory-induced artifacts.
Impact: Improved quality of T2*-weighted images, obtained after correction of respiration-induced field changes, holds promise for improving MRI techniques relying on T2* contrast (BOLD fMRI, QSM) and clinical applications in neurological diseases of the cervical cord.
Introduction
Breathing-induced dynamic B0 field inhomogeneities hinder spatial encoding and lead to blurring, ghosting, and image distortion on T2*-weighted MRI [1]. Spatiotemporal B0 field changes thereby pose a main challenge for reliable MR imaging of the cervical cord, due to its close vicinity with the lungs [2], [3]. One approach to characterize B0 field fluctuations is to insert an additional free induction decay navigator (FIDnav) module during the acquisition, as this does not require gradient encoding and can be easily incorporated into a sequence without increasing scan time [4]–[6]. FIDnav have been previously applied successfully in the brain to measure and compensate for spatiotemporal field changes [7]. In this work, a FIDnav correction framework was used to correct for breathing-induced field fluctuations and to improve T2*-weighted image quality in the cervical cord.Methods
Theory and sequence designA 2D FLASH sequence was modified to acquire an FIDnav module after each slice-selective RF excitation before the imaging readout. Two low-resolution scans with inverted gradient polarities were acquired and combined to form a multi-channel reference image, later used to build a forward model of the complex FIDnav signals. In-plane B0 field changes were estimated with up to second-order spherical harmonics (SH) coefficients. SH coefficients were included in the retrospective correction, achieved using an iterative reconstruction algorithm (NUFFT[8]), as described in [7].
In vivo MR data acquisition
Data were acquired on three healthy controls on a 3T MRI system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64-channel head/neck coil. The imaging protocol included two low-resolution calibration scans (with TR: 878ms, TE: 3.20ms, FA: 44°, matrix size: 32 × 32, in-plane resolution: 6.0×6.0mm2, slice thickness: 5.0mm, 16 slices, BW: 1000 Hz/Px) and one high-resolution FID-navigated structural GRE scan (with TR: 878ms, 5TEs: [6.86, 11.34, 15.34, 19.34, 23.34]ms, FA: 44°, matrix size: 384 × 384, resolution: 0.5×0.5mm2, slice thickness: 5.0mm, 16 slices, BW: 260 Hz/Px). Scans were acquired without acceleration. Image acquisition was conducted in two conditions, where volunteers were instructed to 1) breathe in following a regular breathing pattern (“normal breathing”) and 2) breathe in deeply (“deep breathing”) to produce respiratory-induced spatiotemporal field fluctuations. All scans were centered at C2/C3 cervical level.
Data processing
The deep breathing images (corrected and uncorrected) were registered to the reference image (normal breathing) using the Spinal Cord Toolbox [9], on a slice-by-slice basis, employing a rigid algorithm and a mask of the spinal cord created manually in FSLeyes [10]. Quantitative assessment was achieved using the normalized root mean square error (NRMSE) within the spinal cord mask between the reference image and images reconstructed with and without correction. Finally, voxel-wise T2* maps were generated by fitting a mono-exponential function to the 5 echoes using the nlopt library (version 2.7.1) [11], [12].
Results
The five 0th-, 1st-, and 2nd-order spherical harmonics coefficients are shown for normal breathing and deep breathing conditions in Figure 1. Deep breathing induced fluctuations in B0 field and resulted in ghosting artifacts, mimicking a loss of T2* signal at later echo time. After field correction, image quality was visibly improved, with a reduction in artifacts, as shown in a representative example in Figure 2. Quantitatively, NRMSE values, averaged across echoes and subjects, were reduced after retrospective correction, compared to uncorrected images (NRMSE = 17.33%), with the 2nd-order correction resulting in lower NRMSE values (15.44%) compared to the 1st-order correction (17.31%) (Fig. 3). Severe artifacts on the uncorrected T2* maps were visibly reduced on the 2nd-order corrected T2* maps, whereas the difference between uncorrected and 1st-order corrected was less pronounced (Fig. 4).Discussion
T2*-weighted MRI and T2* maps quality were improved after FIDnav-based correction of breathing-related dynamic field changes. Retrospective correction of second-order phase errors resulted in higher image and maps quality compared to first-order correction. The current model assumes linearity of FIDnav signal change in relation to the field inhomogeneity coefficients. In the presence of irregular or excessively deep breathing pattern, this assumption might be violated, which could explain in part the residual artifacts observed after correction [7]. Future research will investigate real-time shimming, as described in [13] and expand to using FIDnav for motion correction [6], resulting from subject’s motion or physiological fluctuations (swallowing, respiration).Conclusion
In this work, a FIDnav-based framework successfully estimated the spatiotemporal field changes occurring during deep breathing and retrospective correction could compensate for those dynamic changes on a slice-by-slice basis. FIDnavs do not require additional specialized hardware or coil, making them a promising tool for integration into clinical routine protocols aiming at conducting T2* mapping in different pathologies affecting the cervical cord.Acknowledgements
This research was supported in part by NIH grant R01NS121657. MS received grants from Wings For Life Charity (No. WFL-CH-19/20), grants from International Foundation for Research (IRP-158), and Hurka Foundation 2022-2024.
References
[1] S. J. Vannesjo, S. Clare, L. Kasper, I. Tracey, and K. L. Miller, “A method for correcting breathing‐induced field fluctuations in T2*‐weighted spinal cord imaging using a respiratory trace,” Magn Reson Med, vol. 81, no. 6, pp. 3745–3753, Jun. 2019, doi: 10.1002/mrm.27664.
[2] S. J. Vannesjo, K. L. Miller, S. Clare, and I. Tracey, “Spatiotemporal characterization of breathing-induced B0 field fluctuations in the cervical spinal cord at 7T,” Neuroimage, vol. 167, pp. 191–202, Feb. 2018, doi: 10.1016/j.neuroimage.2017.11.031.
[3] T. Verma and J. Cohen‐Adad, “Effect of respiration on the B 0 field in the human spinal cord at 3T,” Magn Reson Med, vol. 72, no. 6, pp. 1629–1636, Dec. 2014, doi: 10.1002/mrm.25075.
[4] J. Pfeuffer, P. Van de Moortele, K. Ugurbil, X. Hu, and G. H. Glover, “Correction of physiologically induced global off‐resonance effects in dynamic echo‐planar and spiral functional imaging,” Magn Reson Med, vol. 47, no. 2, pp. 344–353, Feb. 2002, doi: 10.1002/mrm.10065.
[5] P. Dyverfeldt, V. S. Deshpande, T. Kober, G. Krueger, and D. Saloner, “Reduction of motion artifacts in carotid MRI using free‐induction decay navigators,” Journal of Magnetic Resonance Imaging, vol. 40, no. 1, pp. 214–220, Jul. 2014, doi: 10.1002/jmri.24389.
[6] T. E. Wallace, O. Afacan, M. Waszak, T. Kober, and S. K. Warfield, “Head motion measurement and correction using <scp>FID</scp> navigators,” Magn Reson Med, vol. 81, no. 1, pp. 258–274, Jan. 2019, doi: 10.1002/mrm.27381.
[7] T. E. Wallace, O. Afacan, T. Kober, and S. K. Warfield, “Rapid measurement and correction of spatiotemporal B 0 field changes using FID navigators and a multi‐channel reference image,” Magn Reson Med, vol. 83, no. 2, pp. 575–589, Feb. 2020, doi: 10.1002/mrm.27957.
[8] J. A. Fessler, “On NUFFT-based gridding for non-Cartesian MRI,” Journal of Magnetic Resonance, vol. 188, no. 2, pp. 191–195, Oct. 2007, doi: 10.1016/j.jmr.2007.06.012.
[9] B. De Leener et al., “SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data,” Neuroimage, vol. 145, pp. 24–43, Jan. 2017, doi: 10.1016/j.neuroimage.2016.10.009.
[10] P. McCarthy, “FSLeyes,” https://zenodo.org/records/8376979.
[11] Steven G. Johnson, “The NLopt nonlinear-optimization package,” http://github.com/stevengj/nlopt. 2007.
[12] J. A. Nelder and R. Mead, “A Simplex Method for Function Minimization,” Comput J, vol. 7, no. 4, pp. 308–313, Jan. 1965, doi: 10.1093/comjnl/7.4.308.
[13] T. E. Wallace, T. Kober, J. P. Stockmann, J. R. Polimeni, S. K. Warfield, and O. Afacan, “Real‐time shimming with FID navigators,” Magn Reson Med, vol. 88, no. 6, pp. 2548–2563, Dec. 2022, doi: 10.1002/mrm.29421.
Figures
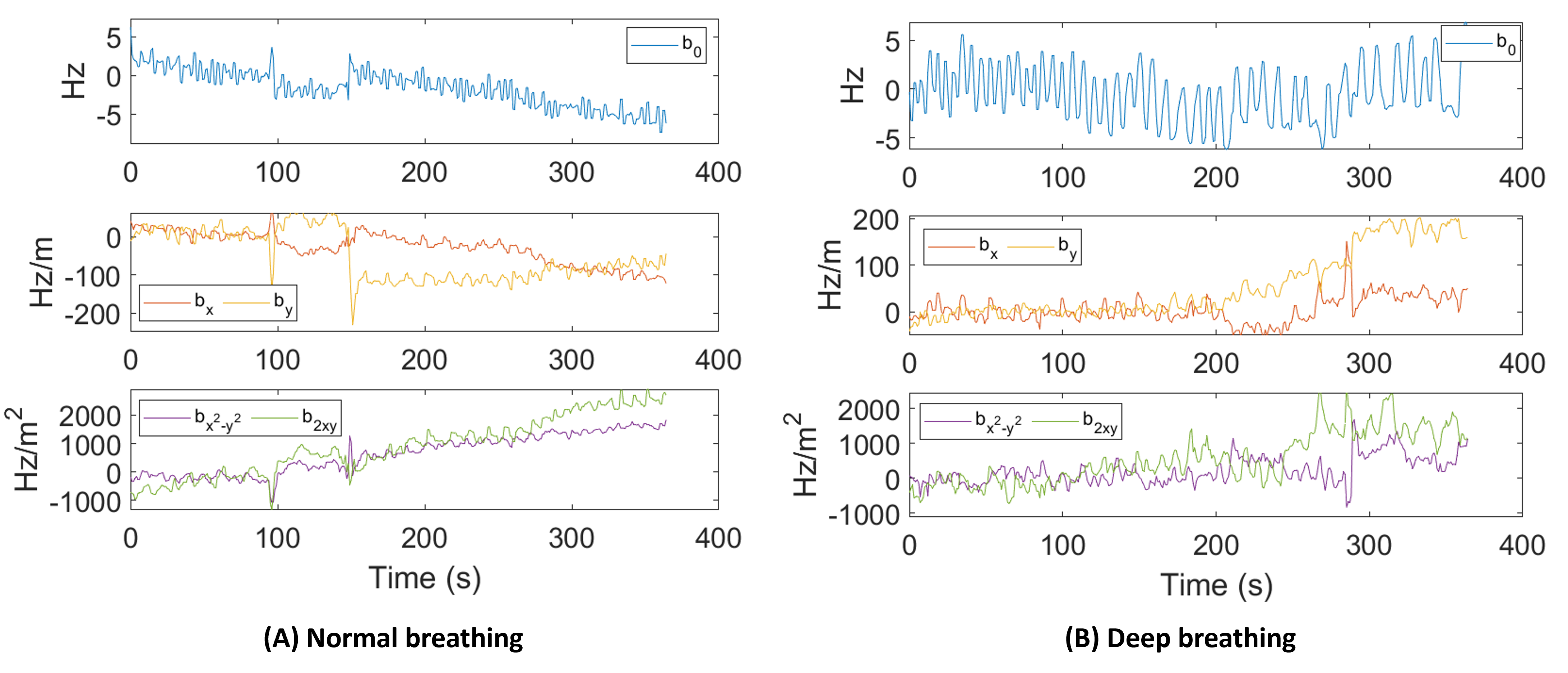
Figure 1: In-plane zeroth- (b0), first- (bx and by), and second-order (bx2y2 and b2xy) dynamic shim coefficients estimated in one slice in one volunteer using the FIDnav framework during (A) normal breathing and (B) deep breathing. Deep breathing leads to modulation of shim coefficients, clearly visible on the zeroth-order shim coefficients (frequency b0).
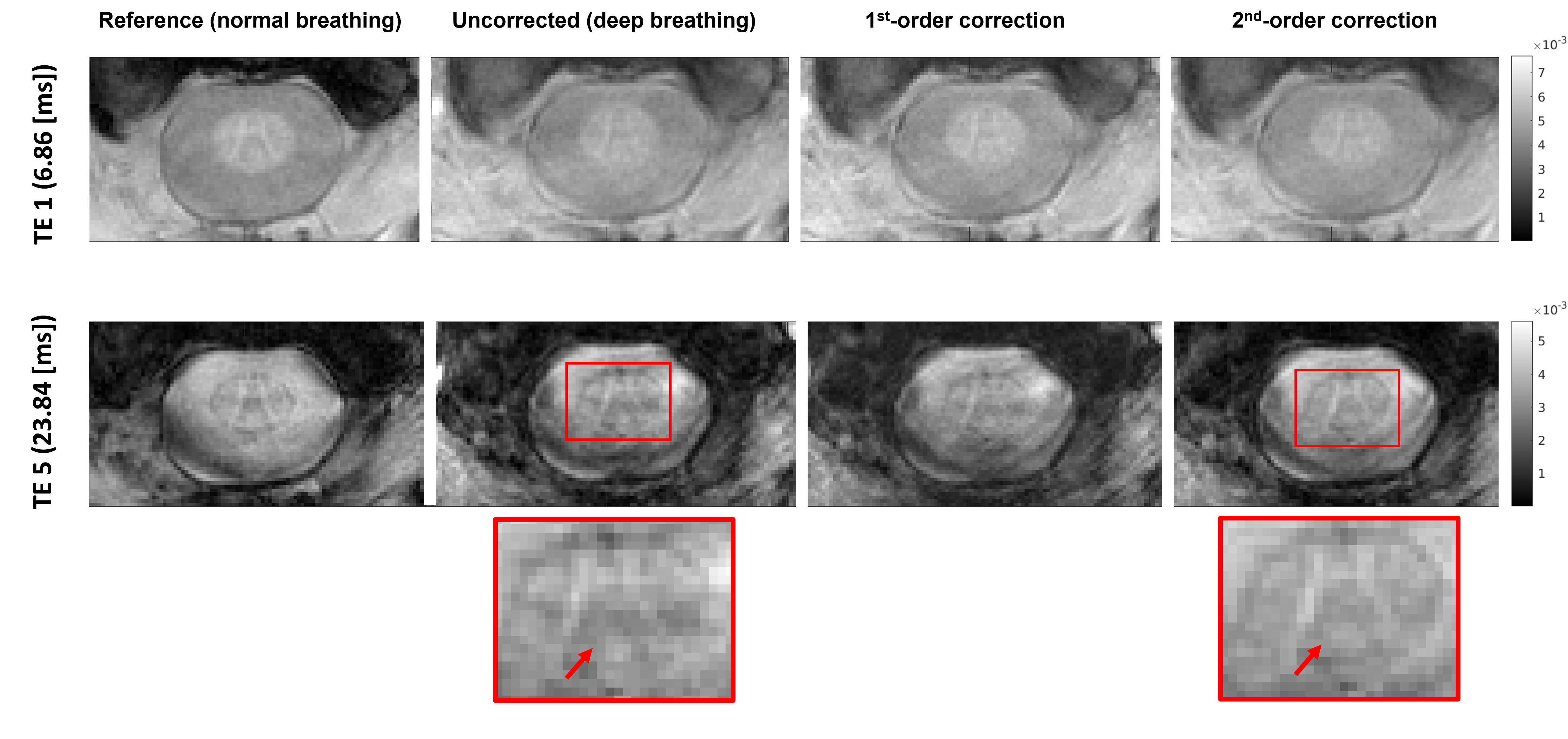
Figure 2: Reference, uncorrected and corrected (first order and second order correction) images for one slice of one volunteer at the first echo (TE1: 6.86 ms) and latest echo (TE5: 23.84 ms). Deep breathing induced ghosting artifacts, more severe at latest echoes. Ghosting was visibly reduced at latest echo after the 2nd-order correction (red arrows).
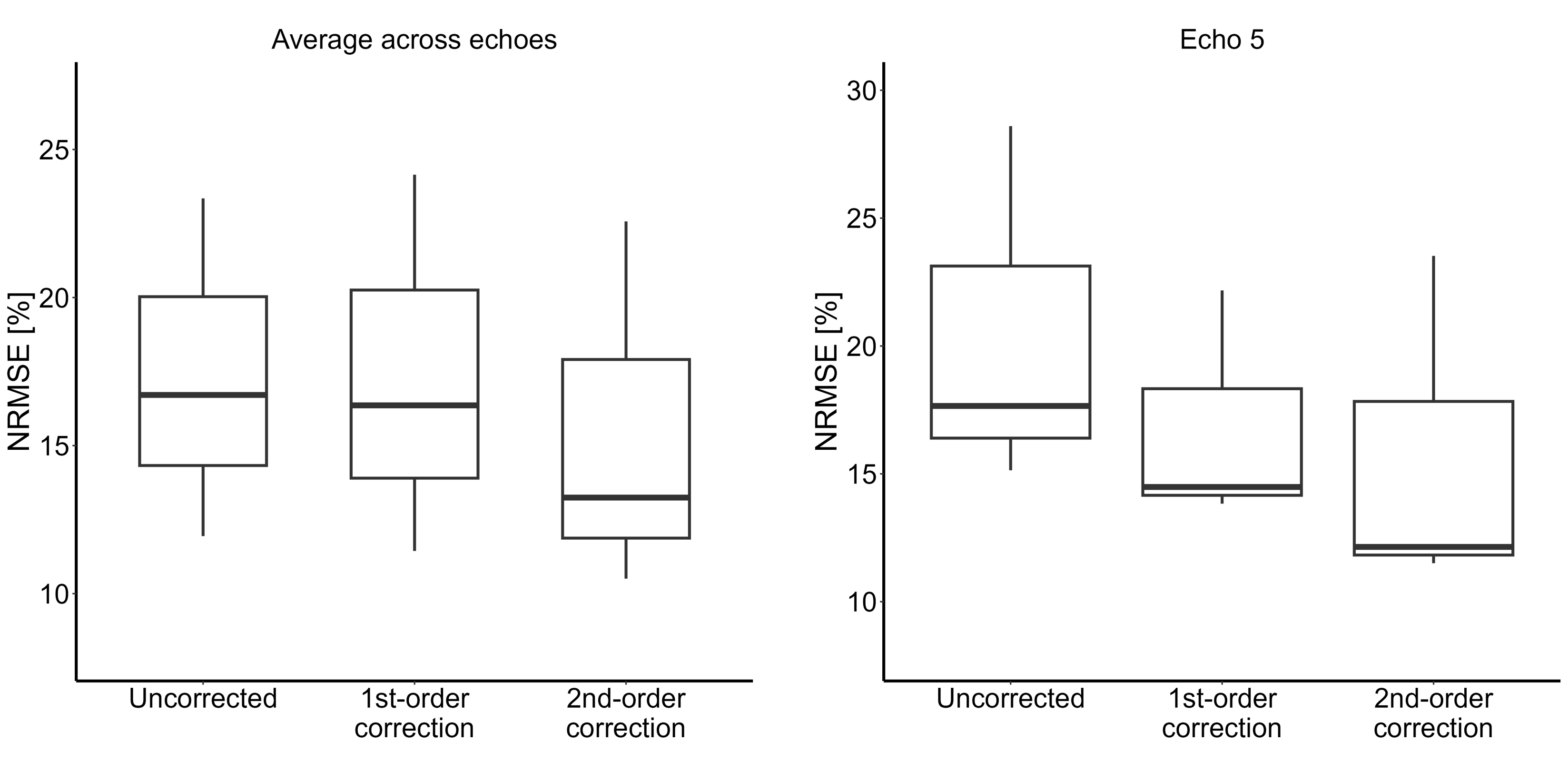
Figure 3: Box and whisker plots of the normalized root mean square error (NRMSE) values of the uncorrected, 1st-order corrected and 2nd-order corrected images with respect to the reference image across the three subjects. Average NRMSE values across echoes and subjects: uncorrected: 17.33%, 1st-order corrected: 17.31%, and 2nd-order corrected: 15.44%. Boxplots are shown for NRMSE values averaged across all five echoes and for the latest echo (Echo 5).
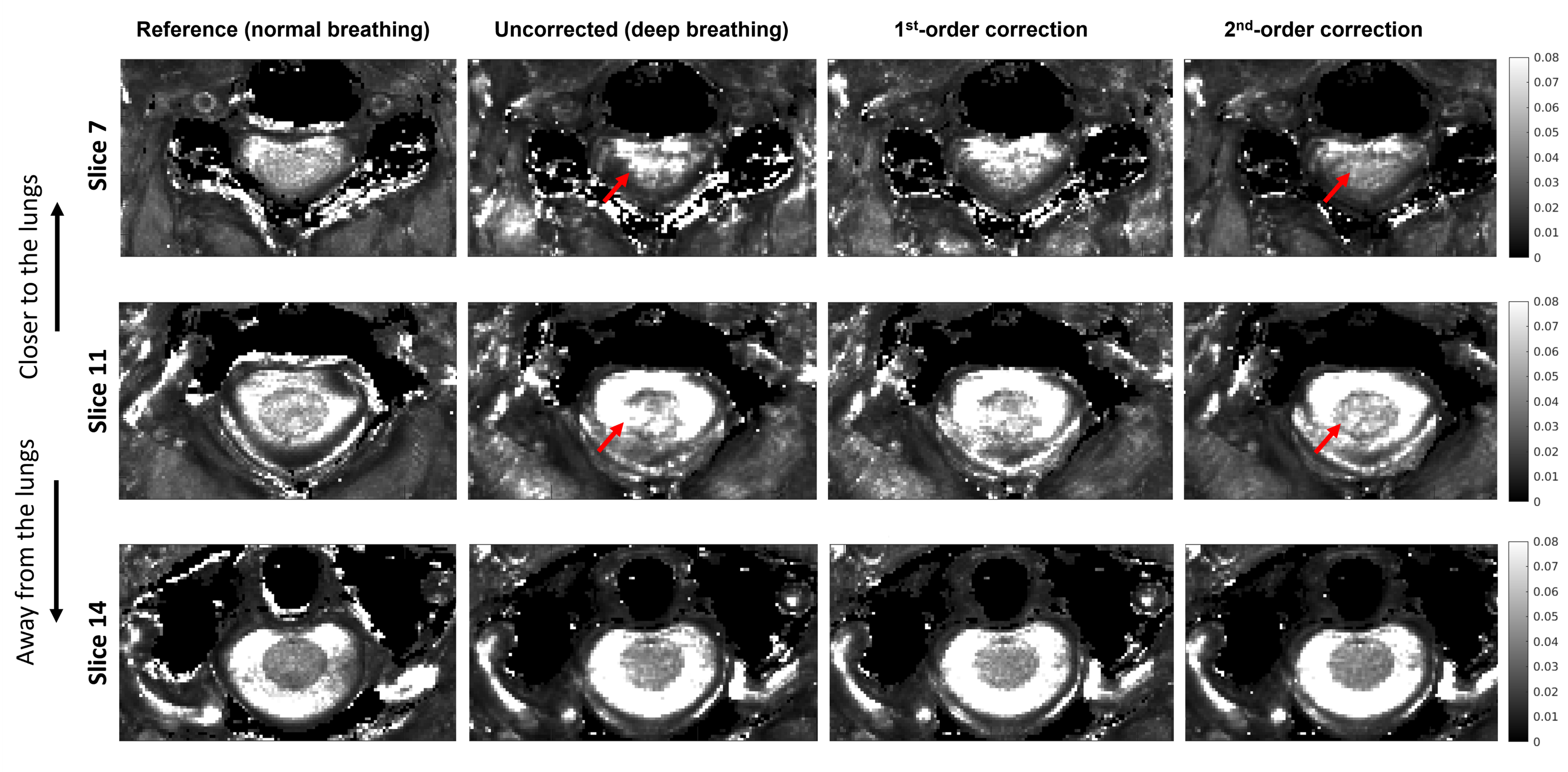
Figure 4: T2* maps of one volunteer obtained from fitting the signal of the reference image, uncorrected image, 1st-order, and 2nd-order corrected images. Hyperintense artifacts were visibly reduced on slices closer to the lungs (slices 7 and 11) with the 2nd-order retrospective correction, as indicated by the red arrows, whereas slices further away from the lungs were less affected (slice 14).

Figure 5: T2* maps of another volunteer obtained from fitting the signal of the reference image, uncorrected image, 1st-order, and 2nd-order corrected images. Hyperintense artifacts were visibly reduced with the 1st- and 2nd-order retrospective correction compared to the uncorrected T2* maps, as indicated by the red arrows.