2334
Feasibility of Multiplexed Sensitivity-Encoding diffusion tensor imaging (MUSE-DTI) in cervical spondylotic myelopathy1Tongji Hospital Affiliated to Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China, 2GE HealthCare, Beijing, China
Synopsis
Keywords: Spinal Cord, Neuro, cervical spondylotic myelopathy
Motivation: MUSE-DTI may elevate spatial resolution and image quality in cervical spine.
Goal(s): This study aimed to investigate the clinical diagnosis value of MUSE-DTI in patients with cervical spondylotic myelopathy (CSM).
Approach: Independent T-test or Mann-Whitney t test and Spearman correlation analysis was used to investigate the differences of FA and ADC values between each two different stages and the correlation to JOA scores.
Results: All MUSE-DTI derived values at MCL were correlated with the clinical JOA scores. The axial diffusivity (AD) values were most sensitive to the secondary damage of distal spinal cord.
Impact: This study presented the ability of MUSE-DTI in better display cervical spinal cord and spinal cord injury with more reliable measurements for the clinical diagnosis and treatment of CSM patients.
Introduction and Purpose
The most frequent type of spinal cord injury is cervical spondylotic myelopathy (CSM). Conventional magnetic resonance imaging (MRI) is the gold diagnosis standard for CSM. Diffusion tensor imaging (DTI) could reflect microstructural changes in the spinal cord by tracing water molecular diffusion. However, due to the complex local anatomical structure and small field of view of the spinal cord, the imaging effect of traditional DTI imaging on the spinal cord is limited. MUSE (Multiplexed Sensitivity-Encoding) achieves high-resolution diffusion imaging through multiple excitation acquisition. MUSE-DTI may improve the structure quality of spinal cord. This study aimed to investigate the clinical diagnosis value of MUSE-DTI in patients with cervical spondylotic myelopathy (CSM).Materials and Methods
From August 2021 to March 2022, a total of 60 subjects (22-71 years) were enrolled, including 51 CSM patients (22 males, 29 females) and 9 healthy subjects (4 males and 5 females). Each subject underwent a MUSE-DTI examination and a clinical Japanese Orthopedic Association (JOA) scale for clinical severity on a 3.0T MR scanner (Sina Architect, GE Healthcare). The cervical canal stenosis of subjects was classified from grade 0 to grade Ⅲ according to MRI-based grading system. Fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), and radial diffusivity (RD) maps were generated by post-processing MUSE-DTI data on the GE workstation (ADW4.5, Functool 9.4.04b, GE Healthcare). Regions of interest (ROIs) were manually drawn at maximal compression level (MCL) of the C2 vertebral body level and C2/3-C6/7 intervertebral disc levels by covering the whole spinal cord.Results
High-resolution MUSE-DTI showed a decreasing trend of FAMCL values from grade 0 to grade Ⅲ, while the MDMCL, ADMCL, and RDMCL values showed an overall increasing trend. Significant differences in MDMCL, ADMCL, and RDMCL values were found between adjacent groups among grades Ⅰ-Ⅲ (p<0.05). The ADC2 values in CSM patients (grade I-Ⅲ) were significantly lower than in healthy individuals (grade 0) (P=0.019). The clinical JOA score has a significant correlation with FAMCL (P=0.035), MDMCL (P<0.001), ADMCL (P<0.001), and RDMCL (P<0.001) values.Discussion
MUSE acquired high-spatial resolution diffusion weighted imaging, high SNR, and minimal motion-induced phase errors, via exciting more than one-time 90° radiofrequency pulse to fill-in every line in k-space with higher signal intensity and less spin dephasing at the first half of TR. MDMCL, FAMCL, ADMCL, and RDMCL values of spinal cord in CSM patients were significantly grade-dependent and all correlated with clinical JOA scores (P<0.05). AD values were more sensitive to reflect the differences between grades 0-Ⅲ. ADMCL values were lower at grade Ⅰ group than grade 0 group despite no visible deformation of the spinal cord on sagittal T2 weighted MRI at MCL of patients with grade Ⅰ but the occurrence of microstructural changes within the medulla. Compared to all the other values, AD value was the most sensitive image biomarker, indicating AD value specifically reflects the axon injury of the longitudinally-oriented fibers in cervical spinal cord.FA value gradually decreased from grade 0 to grade Ⅲ in consistence with Yang's report, but there was no significant difference in FA values between grade Ⅱ and grade Ⅲ as well as between grade I and grade Ⅱ. This may be explained by the “contamination” of gray matter within the measured regions of interest. Spinal cord gray matter with lower anisotropy than white matter was easily interfered as the spinal cord compressed. Another reason may be the increased diffusivity across the neural tracts in several experimental spinal cord damage in animal models.
There were some limitations in this study. First, the sample size of this study is relatively small, especially in grade 0 groups, for CSM is very common among adults. Second, there was no electrophysiological study in diagnosis of the central conduction deficits for comparison and supporting our findings even if a relatively objective clinical scores were collected from the recruited CSM patients at the acute stage . Third, the ROI covered the entire spinal cord and did not distinguish white matter from gray matter, since it is difficult to observe on diffusion weighted imaging, particularly when the spinal cord is compressed.
Conclusion
MUSE-DTI provided superior image quality of cervical spinal cord and its derived parameters displayed a grade dependent trend. The spinal cord changes (MD, FA, AD, and RD values) at the maximum intervertebral disc herniation in CSM patients were significantly correlated with cervical spondylosis-related symptoms. The AD values at C2 level can reflect the secondary damage of distal spinal cord. Therefore, MUSE DTI could be a reliable biomarker for clinical auxiliary diagnosis of spinal cord injury severity in cervical spondylotic myelopathy.Acknowledgements
The author thanks teachers Tang xiangyu and Liu weiyin for their guidance in scanning technology and article writing and teacher Liu Qiufeng for collecting images.References
1. Zhang, H., Wang, C., Chen, W., Wang, F., Yang, Z., Xu, S., & Wang, H. (2021). Deep learning based multiplexed sensitivity-encoding (DL-MUSE) for high-resolution multi-shot DWI. NeuroImage, 244, 118632. https://doi.org/10.1016/j.neuroimage.2021.118632
2. Chu, M. L., Chang, H. C., Chung, H. W., Truong, T. K., Bashir, M. R., & Chen, N. K. (2015). POCS-based reconstruction of multiplexed sensitivity encoded MRI (POCSMUSE): A general algorithm for reducing motion-related artifacts. Magnetic resonance in medicine, 74(5), 1336–1348. https://doi.org/10.1002/mrm.25527
3. Zhang, Z., Huang, F., Ma, X., Xie, S., & Guo, H. (2015). Self-feeding MUSE: a robust method for high resolution diffusion imaging using interleaved EPI. NeuroImage, 105, 552–560. https://doi.org/10.1016/j.neuroimage.2014.10.022
4. Daimiel Naranjo, I., Lo Gullo, R., Morris, E. A., Larowin, T., Fung, M. M., Guidon, A., Pinker, K., & Thakur, S. B. (2020). High-Spatial-Resolution Multishot Multiplexed Sensitivity-encoding Diffusion-weighted Imaging for Improved Quality of Breast Images and Differentiation of Breast Lesions: A Feasibility Study. Radiology. Imaging cancer, 2(3), e190076. https://doi.org/10.1148/rycan.2020190076
5. Kang, Y., Lee, J. W., Koh, Y. H., Hur, S., Kim, S. J., Chai, J. W., & Kang, H. S. (2011). New MRI grading system for the cervical canal stenosis. AJR. American journal of roentgenology, 197(1), W134–W140. https://doi.org/10.2214/AJR.10.5560
6. Budde, M. D., Xie, M., Cross, A. H., & Song, S. K. (2009). Axial diffusivity is the primary correlate of axonal injury in the experimental autoimmune encephalomyelitis spinal cord: a quantitative pixelwise analysis. The Journal of neuroscience : the official journal of the Society for Neuroscience, 29(9), 2805–2813. https://doi.org/10.1523/JNEUROSCI.4605-08.2009
7. Zeng, C., Xiong, J., Wang, J. C., Inoue, H., Tan, Y., Tian, H., & Aghdasi, B. (2016). The Evaluation and Observation of "Hidden" Hypertrophy of Cervical Ligamentum Flavum, Cervical Canal, and Related Factors Using Kinetic Magnetic Resonance Imaging. Global spine journal, 6(2), 155–163. https://doi.org/10.1055/s-0035-1557140
8. Muhle, C., Weinert, D., Falliner, A., Wiskirchen, J., Metzner, J., Baumer, M., Brinkmann, G., & Heller, M. (1998). Dynamic changes of the spinal canal in patients with cervical spondylosis at flexion and extension using magnetic resonance imaging. Investigative radiology, 33(8), 444–449. https://doi.org/10.1097/00004424-199808000-00004
9. Song, S. K., Sun, S. W., Ramsbottom, M. J., Chang, C., Russell, J., & Cross, A. H. (2002). Dysmyelination revealed through MRI as increased radial (but unchanged axial) diffusion of water. NeuroImage, 17(3), 1429–1436. https://doi.org/10.1006/nimg.2002.1267
10. Klawiter, E. C., Xu, J., Naismith, R. T., Benzinger, T. L., Shimony, J. S., Lancia, S., Snyder, A. Z., Trinkaus, K., Song, S. K., & Cross, A. H. (2012). Increased radial diffusivity in spinal cord lesions in neuromyelitis optica compared with multiple sclerosis. Multiple sclerosis (Houndmills, Basingstoke, England), 18(9), 1259–1268. https://doi.org/10.1177/1352458512436593
11. Yang, Y. M., Yoo, W. K., Bashir, S., Oh, J. K., Kwak, Y. H., & Kim, S. W. (2018). Spinal Cord Changes After Laminoplasty in Cervical Compressive Myelopathy: A Diffusion Tensor Imaging Study. Frontiers in neurology, 9, 696. https://doi.org/10.3389/fneur.2018.00696
12. Mamata, H., Jolesz, F. A., & Maier, S. E. (2004). Characterization of central nervous system structures by magnetic resonance diffusion anisotropy. Neurochemistry international, 45(4), 553–560. https://doi.org/10.1016/j.neuint.2003.11.014
13. Kozlowski, P., Raj, D., Liu, J., Lam, C., Yung, A. C., & Tetzlaff, W. (2008). Characterizing white matter damage in rat spinal cord with quantitative MRI and histology. Journal of neurotrauma, 25(6), 653–676. https://doi.org/10.1089/neu.2007.0462
14. Herrera, J. J., Chacko, T., & Narayana, P. A. (2008). Histological correlation of diffusion tensor imaging metrics in experimental spinal cord injury. Journal of neuroscience research, 86(2), 443–447. https://doi.org/10.1002/jnr.21481Figures
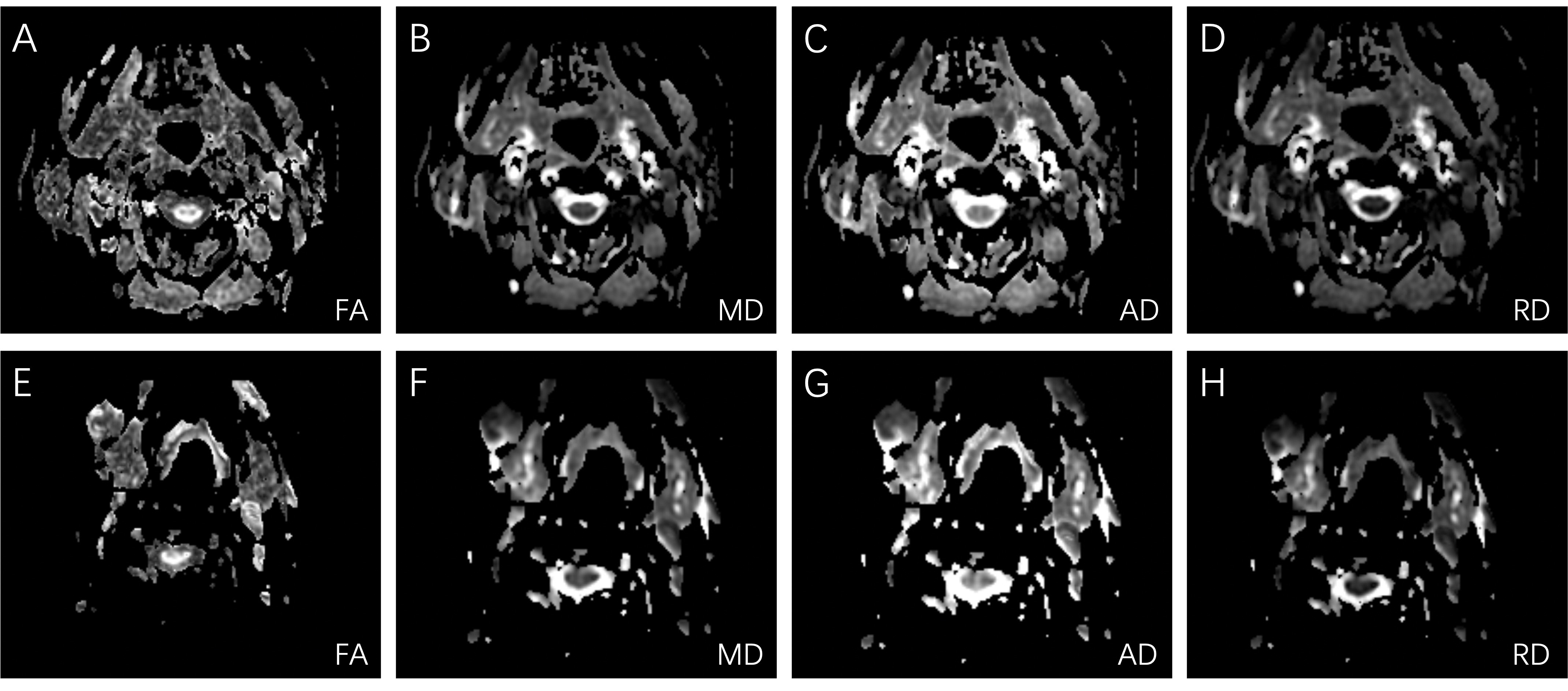
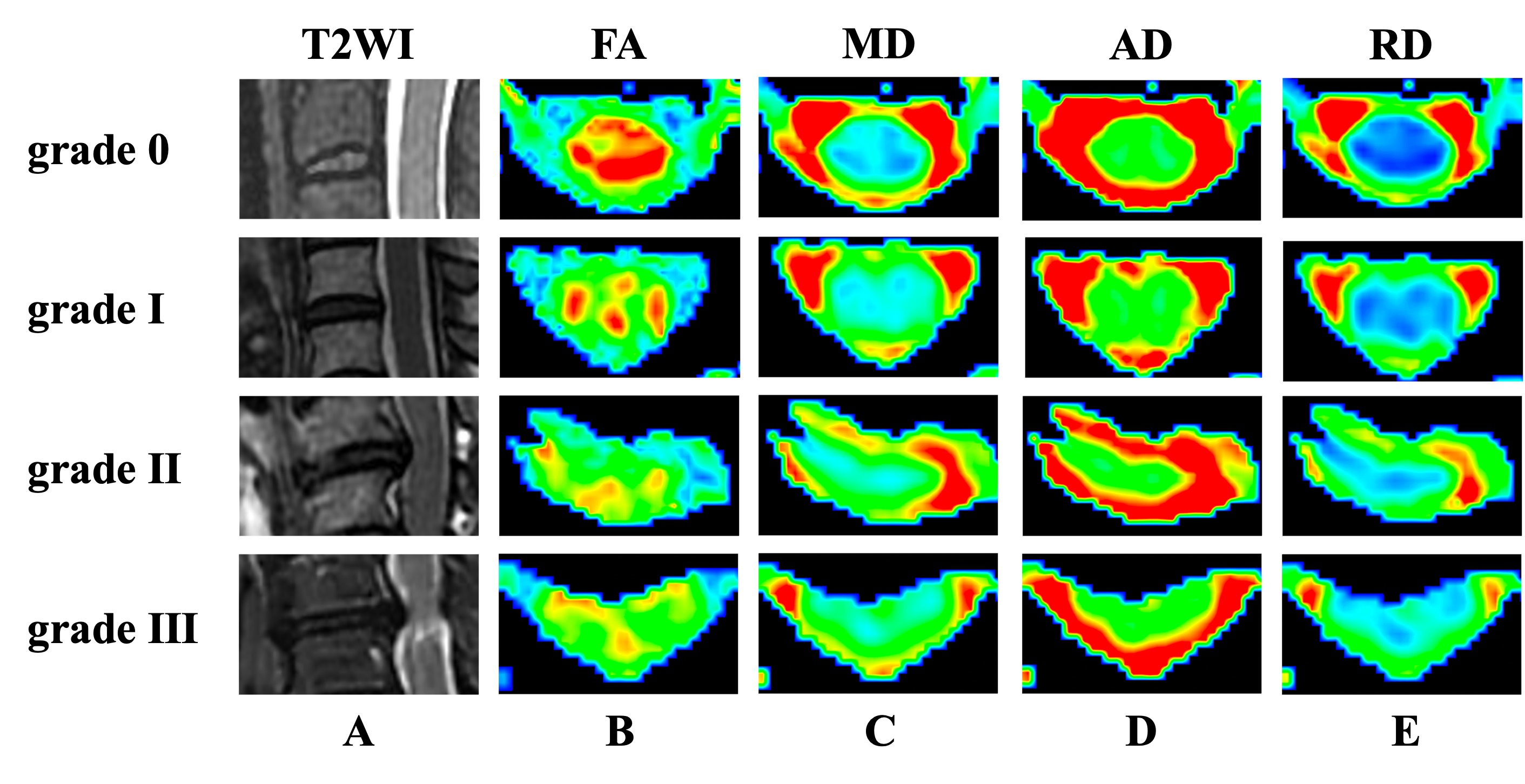
Figure 2: Sagittal T2WI (A), axial colormaps of FA (B), MD (C), AD (D), and RD (E) of the spinal cord at the different levels in grade 0-Ⅲ groups.
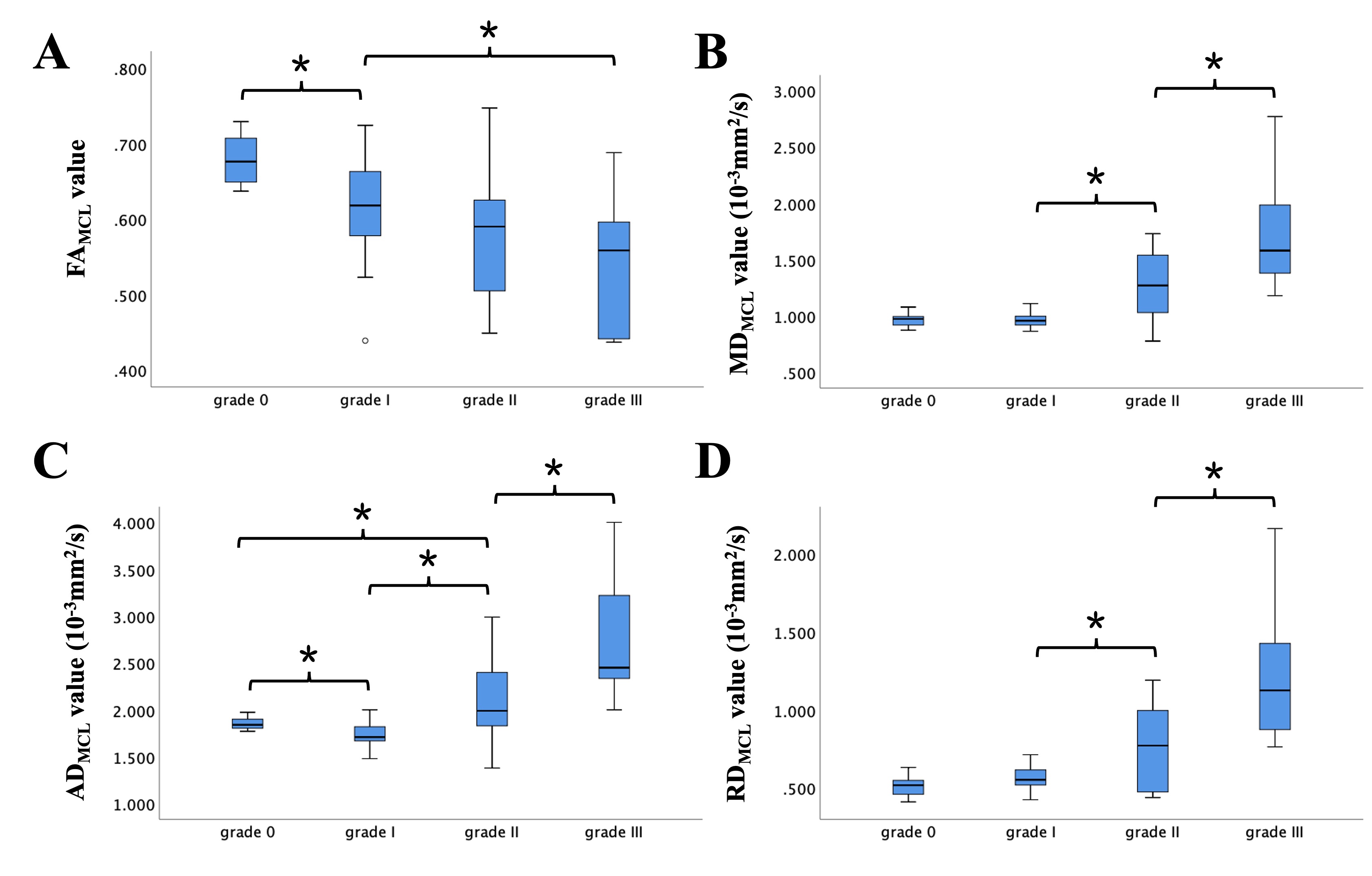
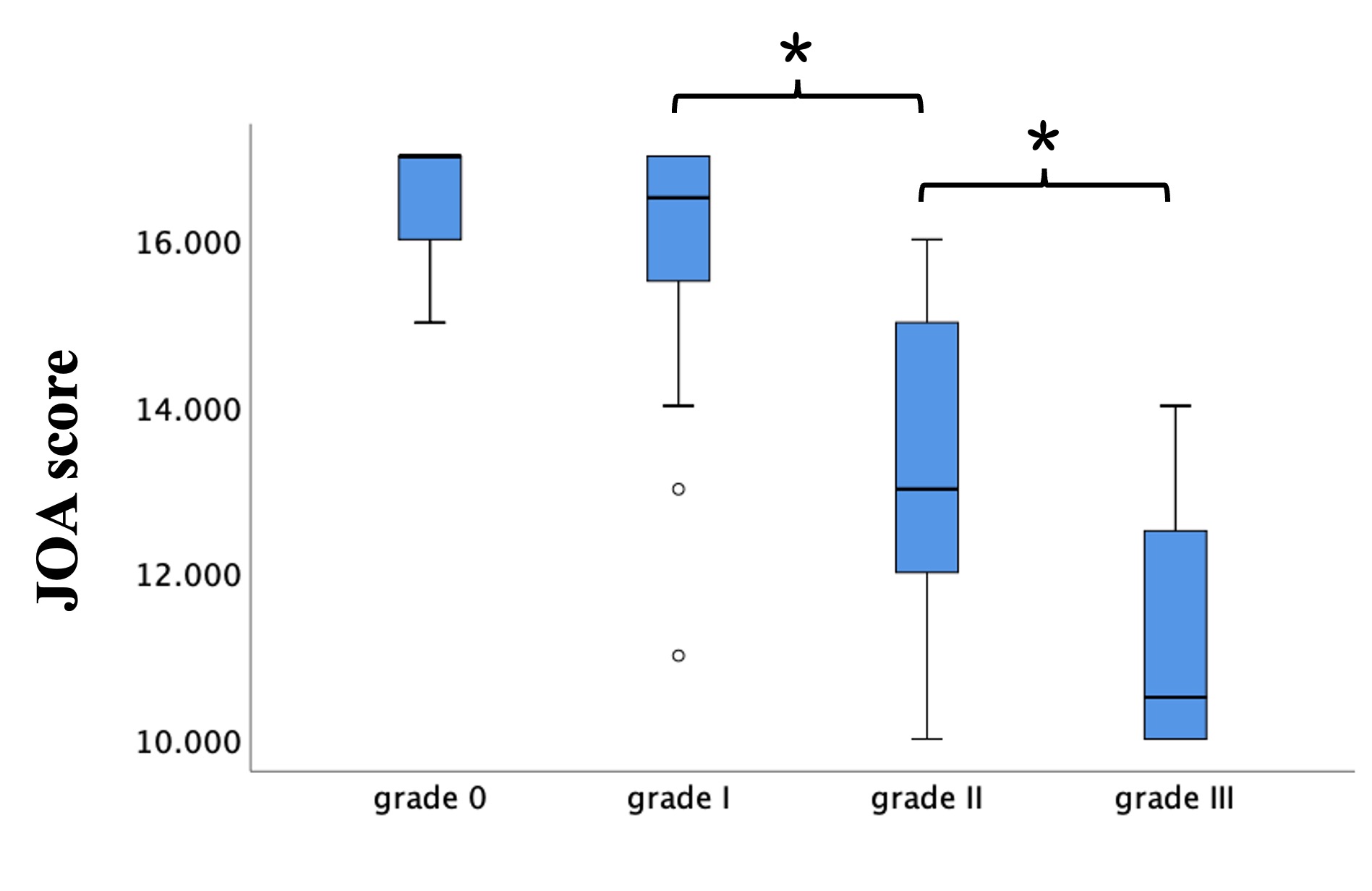
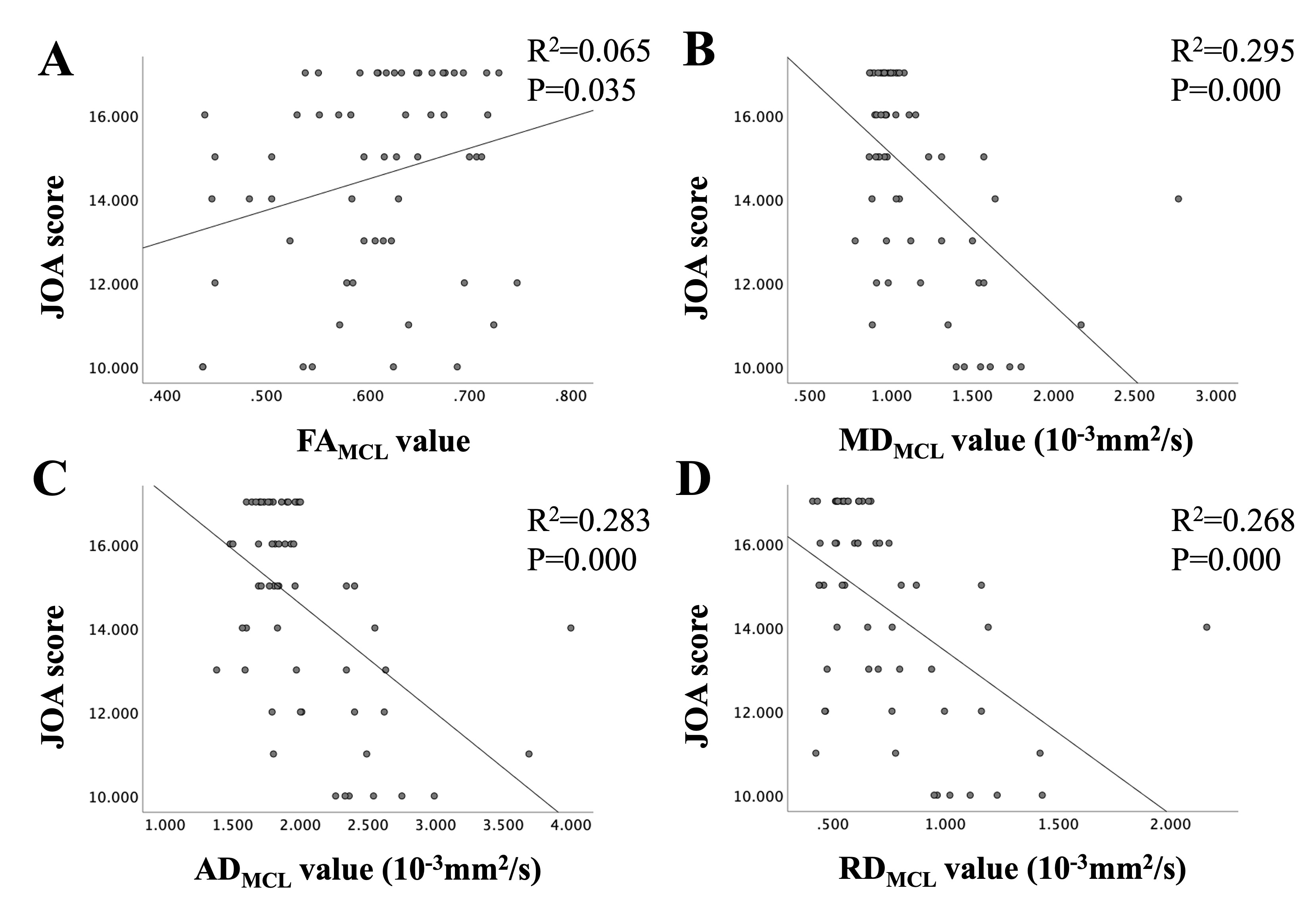
Figure 5: A: The FAMCL values were positively associated with the JOA scores. B, C and D: The MDMCL, ADMCL, and RDMCL values were negatively associated with the JOA scores.