2333
Motion Estimation and Retrospective Correction in 2D Cartesian Turbo Spin Echo Spine Scans1Siemens Medical Solutions USA, Boston, MA, United States, 2Siemens Healthcare GmbH, Erlangen, Germany, 3Pattern Recognition Lab, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 4Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 5Harvard Medical School, Boston, MA, United States, 6Department of Radiology, A. A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States, 7Harvard-MIT Health Sciences and Technology, Massachusetts Institute of Technology, Caimbridge, MA, United States
Synopsis
Keywords: Spinal Cord, Motion Correction, MR Value, Body, Clinical Applications, Spine
Motivation: Patient motion during spine MRI significantly degrades diagnostic utility.
Goal(s): Demonstrate the benefits of an efficient retrospective motion correction technique across clinical 2D TSE spine protocols.
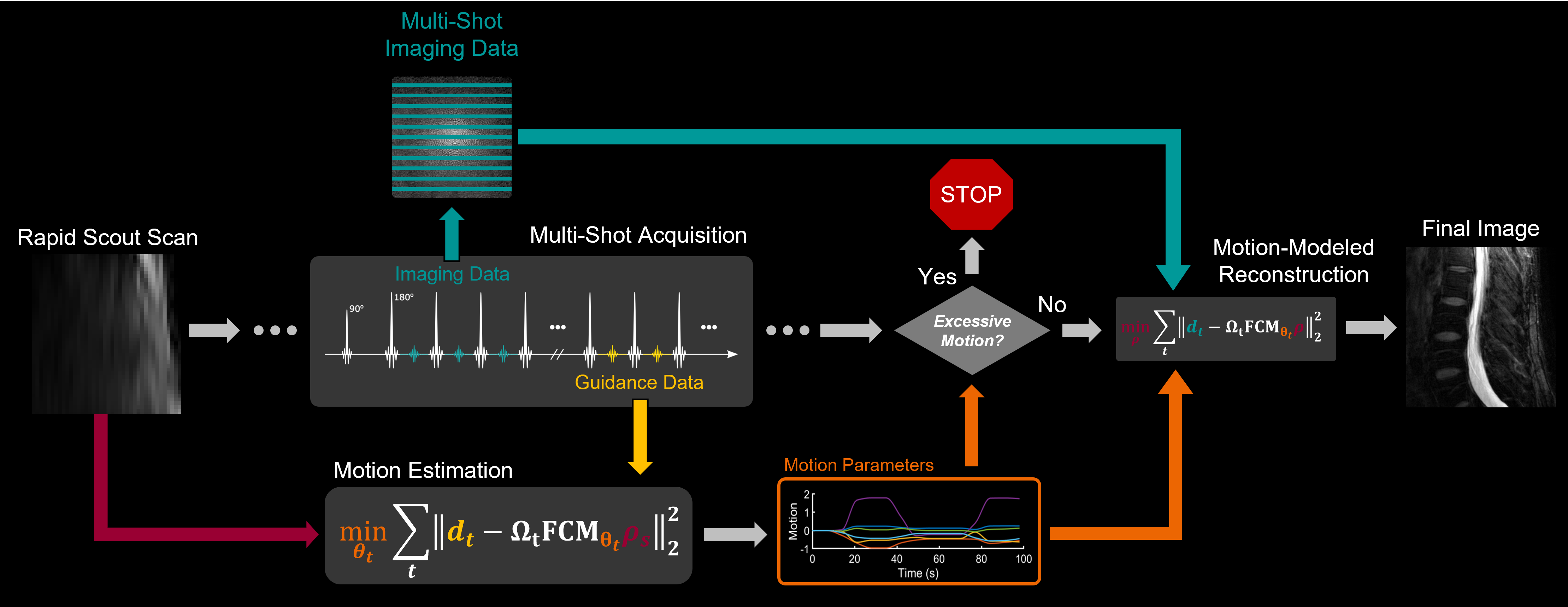
Approach: A rapid low-resolution scout scan in combination with a small number of additional calibration lines are utilized for on-the-fly bulk motion estimation. Region-targeting coil-combination methods are used to model non-rigid motion in the spine. Generalized reconstructions are performed using locally rigid motion information.
Results: Improved image quality for in vivo L- and C-spine scans utilizing partially non-rigid motion correction for instructed subject motion experiments.
Impact: A strategy for performing motion estimation and correction in TSE spine imaging is proposed. Region-targeting coil-combination methods allow for isolation of different spatial sources of non-rigid motion. Improved image quality is demonstrated in vivo under supervised motion conditions.
Purpose
Subject motion is one of the most disruptive events in MRI1 and results in poor diagnostic utility, repeated scans, patient callbacks and significant costs to patients and institutions.2 Despite the development of numerous methods for motion detection and correction,3–12 few have had wide-spread clinical adoption, especially in combination with commonly deployed 2D Cartesian sequences.Recently, the SAMER method has shown promising clinical motion correction results.13 By utilizing a rapid, low-resolution scout scan in combination with a small number of additional calibration lines, SAMER provides accurate motion estimation with minimal effect on image contrast.14,15 Although initially designed for retrospective correction of rigid-motion in 3D brain scans, it has also shown potential for detecting and correcting bulk motion in 2D TSE prostate scans.16
Here we extend SAMER to 2D TSE spine imaging and first demonstrate that the technique can detect and correct bulk motion within in vivo L- and C-spine scans (Fig. 1.). Additionally, by using coil-combination methods,17 we show how SAMER can retrospectively correct for partially non-rigid motion in the spine.
Methods
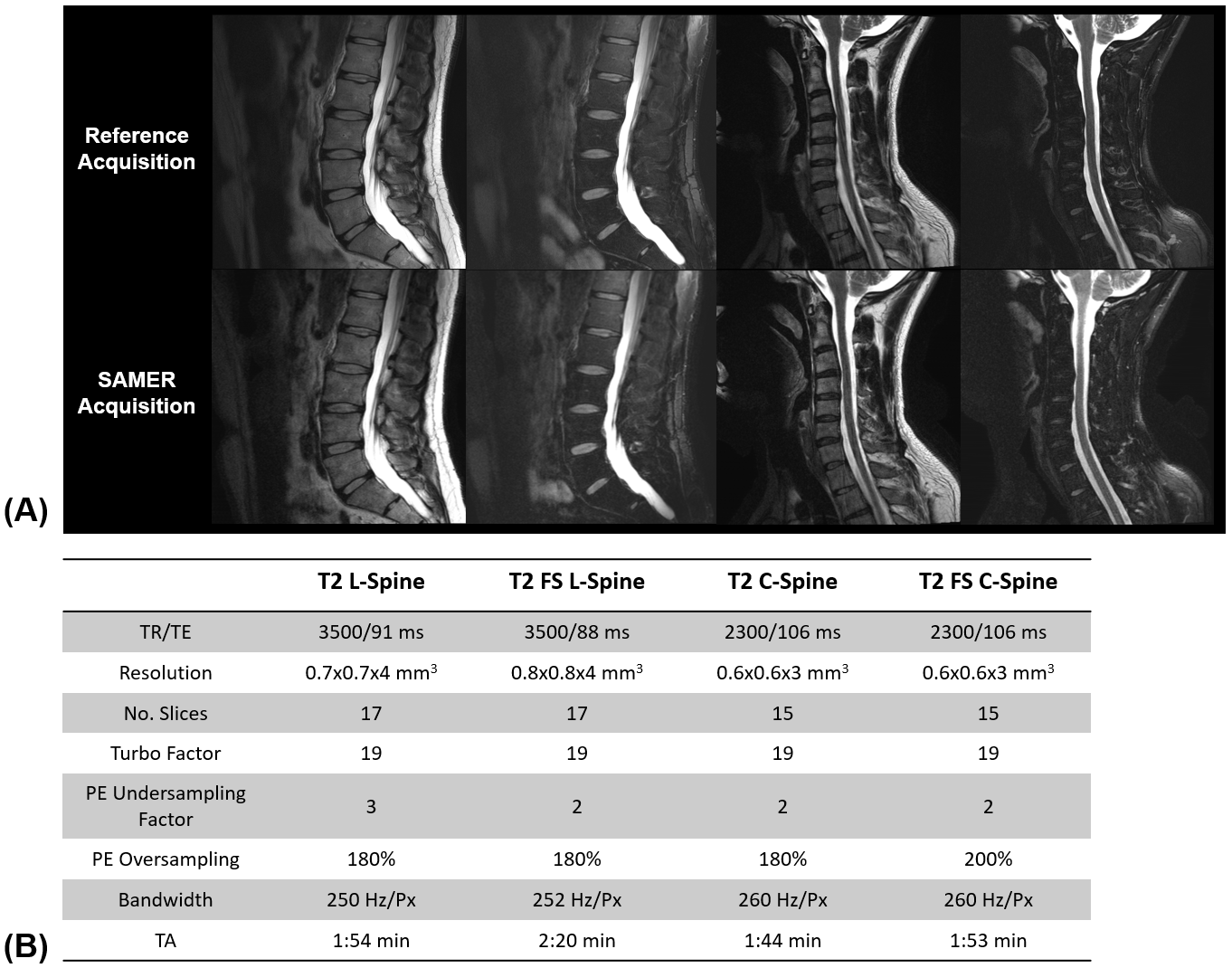
Data AcquisitionIn vivo data were acquired from a consenting healthy volunteer using 32-channel spine and 20-channel head/neck coils on a 3T system (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) with IRB approval. A research application was used to acquire a rapid scout image and guidance lines,15 at the end of each shot, in T2 and fat-saturated T2 (T2 FS) 2D TSE/FSE acquisitions (Fig. 1). Protocols for both sagittal L- and C-spine exams were used (parameters provided in Fig. 2B).
Motion Estimation and Correction
For each shot, the rigid motion parameters that minimized data-consistency between measured guidance-line data and synthetic data generated from the scout image were computed, i.e., $$\min_{\boldsymbol{\theta}}\left\|\boldsymbol{d}_t^{(\mathrm{g})}-\Omega_{\mathrm{g}}\mathrm{FCM}_{\boldsymbol{\theta}}\boldsymbol{\rho}_{\mathrm{s}}\right\|_2^2,$$where $$$\boldsymbol{\rho}_{\mathrm{s}}$$$ is the scout image vector, $$$\boldsymbol{d}_t^{(\mathrm{g})}$$$ is the guidance line data from shot $$$t$$$, $$$\mathrm{M}_{\boldsymbol{\theta}}$$$ is the motion operator for motion parameters $$$\boldsymbol{\theta}$$$, $$$\Omega_{\mathrm{g}}$$$ is the k-space sampling mask for the guidance lines, and $$$\mathrm{F}$$$ and $$$\mathrm{C}$$$ the Fourier transform and coil sensitivity operators, respectively.
Because the scout image is available at the beginning of the acquisition, the SAMER research application performed the above estimation “on-the-fly”, i.e., as soon as the guidance line data from a shot was available.
Once the motion parameters for each shot were estimated, the motion-mitigated reconstruction was computed inline on the scanner according to$$\min_{\boldsymbol{\rho}}\sum_t\left\|\boldsymbol{d}_t^{(\mathrm{i})}-\Omega_t\mathrm{FCM}_{\boldsymbol{\theta}_t}\boldsymbol{\rho}\right\|_2^2+\lambda\mathrm{R}\left(\boldsymbol{\rho}\right)$$where $$$\boldsymbol{d}_t^{(\mathrm{i})}$$$ and $$$\Omega_t$$$ are the imaging data and sampling mask for shot $$$t$$$, respectively, and $$$\mathrm{R}\left(\cdot\right)$$$ represented a Tikhonov regularization term with $$$\lambda$$$, the regularization parameter, chosen for improved conditioning.
Regional Motion Estimation
To address the non-rigid nature of motion in the body, we approximate the motion as being locally-rigid in connected regions. Specifically, we used ROVir17 to generate guidance line data from virtual coils targeting different image regions. The guidance data from different virtual coils were then used to estimate rigid-motion parameters for each region. Motion-mitigated reconstructions for each region were then combined into a single image.
Results
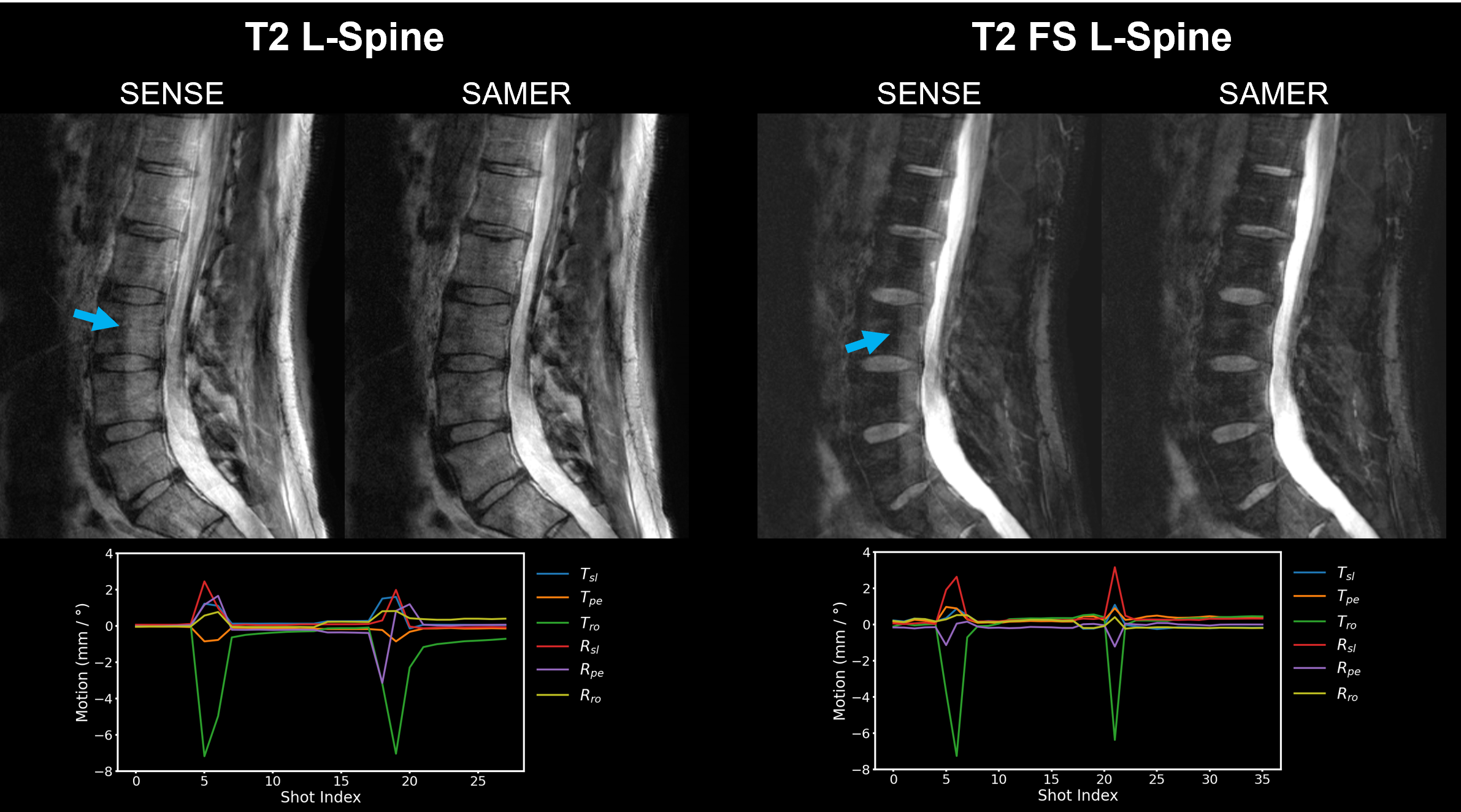
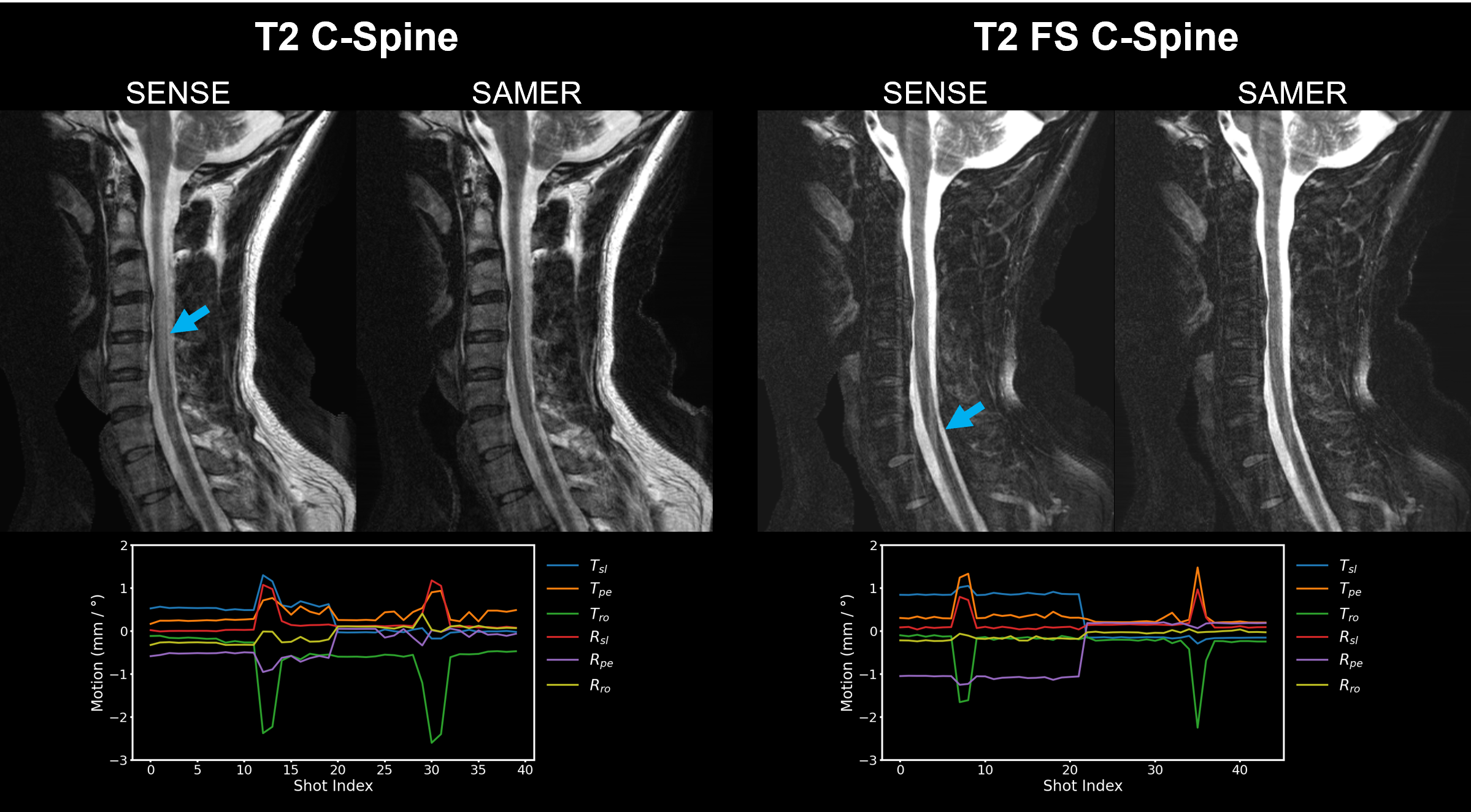
Figure 2A compares the contrast and SNR of the images produced by clinical reference scans and those acquired with the SAMER research sequence. The contrasts of each sequence are closely matched, and the SNR in the reference images is slightly higher due to the clinical use of an in-line deep-learning-based reconstruction.Figures 3 and 4 show results of in vivo motion experiments performed on a subject instructed to move once in the middle of the first and last half of L- and C-spine scans. In each case, the motion-mitigated SAMER reconstruction had reduced levels of artifacts and improved uniformity in the vertebrae and spinal cord.
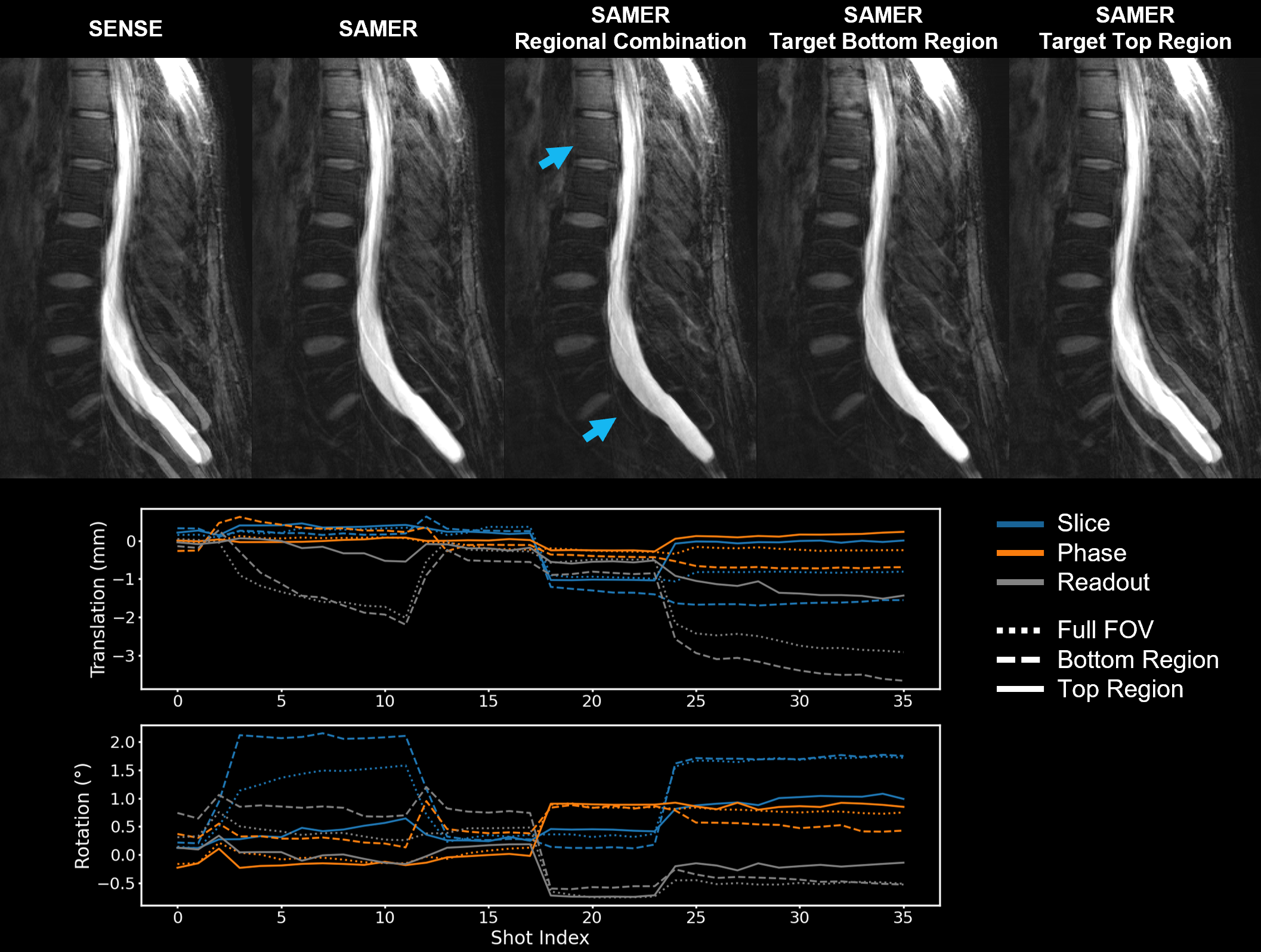
Figure 5 illustrates the potential benefits of regional motion estimation and correction on a healthy volunteer performing instructed motion. ROVir was used to generate virtual coils for the top and bottom of the field of view (FOV). Motion parameters were then estimated from these two regions and the full FOV, and motion-mitigated reconstructions were generated using each set of parameters. Note, the motion estimated for the bottom region is significantly larger than the motion of the top region. This imbalance appears in the corresponding reconstructions, with the bottom (top) region’s motion parameters leading to the largest improvement of the bottom (top) region but the worst image quality in the top (bottom) region. The largest image quality improvement is observed when combining the regional reconstructions.
Conclusions
When applied to in vivo 2D TSE spine scans, SAMER can estimate and retrospectively correct for bulk motion. Region specific coil-combination facilitates partially non-rigid motion correction. On-the-fly motion estimation could be used for real-time avoidance of full scan repeats.Acknowledgements
This work was supported in part by NIH research grants: 1P41EB030006-01, 5U01EB025121-03, and through research support provided by Siemens Medical Inc.References
1. Sadigh G, Applegate KE, Saindane AM. Prevalence of Unanticipated Events Associated With MRI Examinations: A Benchmark for MRI Quality, Safety, and Patient Experience. J Am Coll Radiol. 2017;14(6):765-772. doi:10.1016/j.jacr.2017.01.043
2. Andre JB, Bresnahan BW, Mossa-Basha M, et al. Toward Quantifying the Prevalence, Severity, and Cost Associated With Patient Motion During Clinical MR Examinations. J Am Coll Radiol. 2015;12(7):689-695. doi:10.1016/j.jacr.2015.03.007
3. Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions: Motion Artifacts and Correction. J Magn Reson Imaging. 2015;42(4):887-901. doi:10.1002/jmri.24850
4. Zaitsev M, Dold C, Sakas G, Hennig J, Speck O. Magnetic resonance imaging of freely moving objects: prospective real-time motion correction using an external optical motion tracking system. NeuroImage. 2006;31(3):1038-1050. doi:10.1016/j.neuroimage.2006.01.039
5. Maclaren J, Armstrong BSR, Barrows RT, et al. Measurement and Correction of Microscopic Head Motion during Magnetic Resonance Imaging of the Brain. Hess CP, ed. PLoS ONE. 2012;7(11):e48088. doi:10.1371/journal.pone.0048088
6. Frost R, Wighton P, Karahanoğlu FI, et al. Markerless high‐frequency prospective motion correction for neuroanatomical MRI. Magn Reson Med. 2019;82(1):126-144. doi:10.1002/mrm.27705
7. Aksoy M, Forman C, Straka M, et al. Real-time optical motion correction for diffusion tensor imaging. Magn Reson Med. 2011;66(2):366-378. doi:10.1002/mrm.22787
8. Derbyshire JA, Wright GA, Henkelman RM, Hinks RS. Dynamic scan-plane tracking using MR position monitoring. J Magn Reson Imaging. 1998;8(4):924-932. doi:10.1002/jmri.1880080423
9. White N, Roddey C, Shankaranarayanan A, et al. PROMO: Real-time prospective motion correction in MRI using image-based tracking. Magn Reson Med. 2010;63(1):91-105. doi:10.1002/mrm.22176
10. Ooi MB, Aksoy M, Maclaren J, Watkins RD, Bammer R. Prospective motion correction using inductively coupled wireless RF coils: Prospective Motion Correction Using Wireless Markers. Magn Reson Med. 2013;70(3):639-647. doi:10.1002/mrm.24845
11. Tisdall MD, Hess AT, Reuter M, Meintjes EM, Fischl B, van der Kouwe AJW. Volumetric navigators for prospective motion correction and selective reacquisition in neuroanatomical MRI: Volumetric Navigators in Neuroanatomical MRI. Magn Reson Med. 2012;68(2):389-399. doi:10.1002/mrm.23228
12. Wallace TE, Afacan O, Waszak M, Kober T, Warfield SK. Head motion measurement and correction using FID navigators. Magn Reson Med. 2019;81(1):258-274. doi:10.1002/mrm.27381
13. Lang M, Tabari A, Polak D, et al. Clinical Evaluation of Scout Accelerated Motion Estimation and Reduction Technique for 3D MR Imaging in the Inpatient and Emergency Department Settings. Am J Neuroradiol. 2023;44(2):125-133. doi:10.3174/ajnr.A7777
14. Polak D, Splitthoff DN, Clifford B, et al. Scout accelerated motion estimation and reduction (SAMER). Magn Reson Med. August 2021:mrm.28971. doi:10.1002/mrm.28971
15. Polak D, Hossbach J, Splitthoff DN, et al. Motion guidance lines for robust data-consistency based retrospective motion correction in 2D and 3D MRI. Magn Reson Med. In Press. doi:10.1002/mrm.29534
16. Clifford B, Polak D, Lo WC, et al. Motion Estimation and Retrospective Correction in 2D Cartesian Turbo Spin Echo Prostate Scans. In: ISMRM. ; 2023:1021.
17. Kim D, Cauley SF, Nayak KS, Leahy RM, Haldar JP. Region‐optimized virtual (ROVir) coils: Localization and/or suppression of spatial regions using sensor‐domain beamforming. Magn Reson Med. 2021;86(1):197-212. doi:10.1002/mrm.28706
Figures