2332
Intravoxel incoherent motion (IVIM) MRI in the cervical cord: application to traumatic spinal cord injury1Spinal Cord Injury Center, Balgrist University Hospital, Zurich, Switzerland, 2High Field MR Center, Medical University of Vienna, Vienna, Austria, 3MR Research Collaborations, Siemens Healthcare Pty Ltd, Melbourne, Australia, 4CNRS, CRMBM, Aix-Marseille Univ, Marseille, France, 5CEMEREM, APHM, Hôpital Universitaire Timone, Marseille, France, 6Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany
Synopsis
Keywords: Spinal Cord, Spinal Cord
Motivation: Traumatic spinal cord injury (SCI) leads to a perfusion deficit in the cervical cord, a factor that significantly contributes to neurodegeneration. Characterizing changes in perfusion after injury holds potential to better understand progressive SCI-induced neurodegeneration.
Goal(s): To determine blood perfusion changes in the cervical cord of tetraplegic SCI patients using intravoxel incoherent motion (IVIM) MRI.
Approach: Cardiac-gated IVIM MRI was applied to the cervical cord in 21 SCI patients and 38 healthy controls (HC).
Results: SCI patients showed significant changes in IVIM parameters in the grey matter of the cervical cord compared to HC, indicating remote perfusion deficit above the injury site.
Impact: The characterization of spinal cord perfusion changes in SCI provides valuable insights into tissue-specific changes which can serve as a foundation for the development of targeted treatment strategies.
Introduction
Traumatic spinal cord injury (SCI) results in perfusion impairment at and remote from the lesion site, which contributes to neuronal damage following the injury and may hinder functional recovery1–4. However, the spatial profile of perfusion changes remote to a traumatic injury in vivo remains understudied due to the lack of non-invasive tools sensitive to perfusion. Intravoxel incoherent motion (IVIM) is a diffusion-based MRI technique indirectly sensitive to tissue perfusion5. In this study, IVIM was applied to the cervical cord (C1-C3) of chronic tetraplegic SCI patients and healthy controls (HC) to assess perfusion alteration in the grey and white matter (GM/WM) rostral to the injury.Methods
In vivo image acquisitionMRI data were acquired in 21 SCI patients (mean age: 48.1±15.1 years, 15 males) and 38 HC (mean age: 49.0±16.0 years, 18 males) on a 3T scanner (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) with a 64-channel head/neck RF coil. The protocol consisted of a sagittal T2-weighted TSE sequence for cervical level localization, an axial T2*-weighted 3D multi-echo GRE sequence6 for WM/GM segmentation and cross-sectional areas (CSA) calculation, and an optimized cardiac-gated IVIM protocol7 based on axial 2D-RF spin-echo EPI ZOOMit sequences with 0.9×0.9 mm2 in-plane resolution, 5mm-slice thickness, 34×108 matrix size, and 14 b-values ([0;50;100;150;200;250;300;350;400;450;500;550;600;650] s/mm2). All scans were centered at C2/C3 disk, covering C1-C3 levels. The nominal acquisition time was ca. 39 minutes.
Data processing and fitting
The processing pipeline was conducted with the IVIM toolbox8 to generate the IVIM maps, and included denoising9, Gibbs artefacts removal10,11 (DIPY12), motion (sct_dmri_moco13) and distortion correction (FSL topup14). Voxel-wise fitting of the MR signal was based on the biexponential IVIM model5:
$$S(b) = S_0 e^{-bD}(Fe^{-bD^*}+1-F)$$
Parameters of the IVIM model indirectly provide information on microvascular volume fraction ($$$F$$$), blood velocity ($$$D^*$$$), and tissue diffusion ($$$D$$$), whereas $$$F·D^*$$$has been shown to be sensitive to blood flow15. IVIM images and maps were registered to template16/atlas17, based on T2*-weighted images. IVIM parameters were extracted slice-wise in subject space across C1-C3 levels, in the WM/GM. ROIs were eroded at the cord periphery to prevent possible partial volume effect. Cervical cord atrophy was determined using CSAs obtained from the T2*-weighted image segmentations. IVIM parameters and CSAs were compared between SCI patients and HC with two-sample t-tests in R (version 4.3.1)18.
Results
The optimized IVIM protocol was successfully conducted on cervical data of 21 chronic (6 months-38 years post-injury) tetraplegic SCI patients, with similar image quality and SNR compared to healthy controls. CSAs were significantly lower in the WM of SCI patients compared to HC (mean±SD: SCI: 47.22±10.53 mm2; HC: 67.04±9.21 mm2, Δ=-29.6 %, p<0.001) and in the GM (SCI: 11.45±1.84 mm2, HC: 14.51±1.05 mm2, Δ=-21.1 %, p<0.001) (Figure 1).Perfusion mean maps showed a visual decrease in microvascular volume fraction ($$$F$$$) and increase in blood velocity-related parameter ($$$D^*$$$) in SCI patients compared to HC (Figure 2). Quantitatively, in the GM, a significant reduction in $$$F$$$ (Δ=-24.68%, p<0.01, range: HC: 6.06%-14.07%, SCI: 3.75%-12.82%) and increase in $$$D^*$$$ (Δ=+33.11%, p<0.01, range: HC: 9.58%-22.30%, SCI: 4.29%-30.91%) of SCI patients compared to HC was observed, while no statistical difference in blood flow index ($$$F·D^*$$$) was detected (p=0.22). Diffusion coefficient was significantly increased in SCI patients (Table 1). No statistical difference was observed in perfusion-related parameters in WM comparing SCI to HC, except for a significant increase in diffusion coefficient in SCI (Figure 3).
Discussion
Cervical cord atrophy was in the range of reported literature values (10-30%)19–21. Differences observed in blood volume and velocity-related parameters indicated perfusion changes rostral to the injury in the GM region. This aligns with our hypothesis that microvasculature in the GM is particularly sensitive to trauma22. Interestingly, no significant difference in blood flow-related parameter was observed, suggesting possible compensation mechanisms to maintain constant blood flow over C1-C3. Of note, the differences observed between the two groups were greater than the test-retest differences measured in a reliability study (16.98% and 12.77% for $$$F$$$ and $$$D^*$$$, respectively, in the GM), giving us confidence in the reported differences. Therefore, perfusion alteration may contribute to ongoing neurodegeneration, as detected with the increase in diffusion coefficient, and ultimately impact recovery trajectories23.Conclusion
The current study provides novel insights into injury-induced spinal cord perfusion impairment, indicating that IVIM parameters are sensitive to perfusion compromise in the cervical cord at the group level. Future research will focus on characterizing perfusion longitudinally in the subacute phase following a traumatic injury to study the temporal profile of changes in perfusion and shed light on processes occurring in the acute and subacute SCI.Acknowledgements
The authors would like to thank all the participants for their time. This work is based on experiments performed at the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zurich, and methodological developments performed at the Centre de Résonance Magnétique Biologique et Médicale, CRMBM-CEMEREM, Aix-Marseille University/CNRS, Marseille, France. This project has received funding from the Wings for Life charity (No WFL-CH-19/20) and Balgrist Stiftung 2021.References
1. Tator CH, Fehlings MG. Review of the secondary injury theory of acute spinal cord trauma with emphasis on vascular mechanisms. J Neurosurg. 1991;75(1):15-26. doi:10.3171/jns.1991.75.1.0015
2. Fassbender JM, Whittemore SR, Hagg T. Targeting Microvasculature for Neuroprotection after SCI. Neurotherapeutics. 2011;8(2):240-251. doi:10.1007/s13311-011-0029-1
3. Roolfs L, Hubertus V, Spinnen J, Shopperly LK, Fehlings MG, Vajkoczy P. Therapeutic Approaches Targeting Vascular Repair After Experimental Spinal Cord Injury: A Systematic Review of the Literature. Neurospine. 2022;19(4):961-975. doi:10.14245/ns.2244624.312
4. Li Y, Lucas-Osma AM, Black S, et al. Pericytes impair capillary blood flow and motor function after chronic spinal cord injury. Nat Med. 2017;23(6):733-741. doi:10.1038/nm.4331
5. Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168(2):497-505. doi:10.1148/radiology.168.2.3393671
6. Büeler S, Yiannakas MC, Damjanovski Z, Freund P, Liechti MD, David G. Optimized multi-echo gradient-echo magnetic resonance imaging for gray and white matter segmentation in the lumbosacral cord at 3 T. Sci Rep. 2022;12(1):16498. doi:10.1038/s41598-022-20395-1
7. Lévy S, Freund P, Callot V, Seif M. Spinal cord perfusion mapping using Intra-Voxel Incoherent Motion at 3T in healthy individuals and Degenerative Cervical Myelopathy patients. In: International Society for Magnetic Resonance in Medicine (ISMRM). ; 2021:3462.
8. Lévy S, Rapacchi S, Massire A, et al. Intravoxel Incoherent Motion at 7 Tesla to quantify human spinal cord perfusion: limitations and promises. Magn Reson Med. 2020;84(3):1198-1217. doi:10.1002/mrm.28195
9. Manjón J V., Coupé P, Concha L, Buades A, Collins DL, Robles M. Diffusion Weighted Image Denoising Using Overcomplete Local PCA. PLoS One. 2013;8(9):e73021. doi:10.1371/journal.pone.0073021
10. Kellner E, Dhital B, Kiselev VG, Reisert M. Gibbs-ringing artifact removal based on local subvoxel-shifts. Magn Reson Med. 2016;76(5):1574-1581. doi:10.1002/mrm.26054
11. Perrone D, Aelterman J, Pižurica A, Jeurissen B, Philips W, Leemans A. The effect of Gibbs ringing artifacts on measures derived from diffusion MRI. Neuroimage. 2015;120:441-455. doi:10.1016/j.neuroimage.2015.06.068
12. Garyfallidis E, Brett M, Amirbekian B, et al. Dipy, a library for the analysis of diffusion MRI data. Front Neuroinform. 2014;8:1-17. doi:10.3389/fninf.2014.00008
13. De Leener B, Lévy S, Dupont SM, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017;145:24-43. doi:10.1016/j.neuroimage.2016.10.009
14. Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. Neuroimage. 2003;20(2):870-888. doi:10.1016/S1053-8119(03)00336-7
15. Le Bihan D, Turner R. The capillary network: a link between ivim and classical perfusion. Magn Reson Med. 1992;27(1):171-178. doi:10.1002/mrm.1910270116
16. De Leener B, Fonov VS, Collins DL, Callot V, Stikov N, Cohen-Adad J. PAM50: Unbiased multimodal template of the brainstem and spinal cord aligned with the ICBM152 space. Neuroimage. 2018;165:170-179. doi:10.1016/j.neuroimage.2017.10.041
17. Lévy S, Benhamou M, Naaman C, Rainville P, Callot V, Cohen-Adad J. White matter atlas of the human spinal cord with estimation of partial volume effect. Neuroimage. 2015;119:262-271. doi:10.1016/j.neuroimage.2015.06.040
18. R Core Team. R: A Language and Environment for Statistical Computing. https://www.r-project.org/
19. Seif M, David G, Huber E, Vallotton K, Curt A, Freund P. Cervical Cord Neurodegeneration in Traumatic and Non-Traumatic Spinal Cord Injury. J Neurotrauma. 2020;37(6):860-867. doi:10.1089/neu.2019.6694
20. David G, Pfyffer D, Vallotton K, et al. Longitudinal changes of spinal cord grey and white matter following spinal cord injury. J Neurol Neurosurg Psychiatry. 2021;92(11):1222-1230. doi:10.1136/jnnp-2021-326337
21. Huber E, David G, Thompson AJ, Weiskopf N, Mohammadi S, Freund P. Dorsal and ventral horn atrophy is associated with clinical outcome after spinal cord injury. Neurology. 2018;90(17):e1510-e1522. doi:10.1212/WNL.0000000000005361
22. Smith NJ, Doody NE, Štěpánková K, et al. Spatiotemporal microvascular changes following contusive spinal cord injury. Front Neuroanat. 2023;17. doi:10.3389/fnana.2023.1152131
23. Callot V, Duhamel G, Laurin J, Maus de Paula A, Cozzone PJ. Intra Voxel Incoherent Motion (IVIM) MRI: An Alternative Method to Get Spinal Cord (SC) Vascular Description. Preliminary Results in Healthy and Injured Mice. In: International Society for Magnetic Resonance in Medicine (ISMRM). ; 2012:1037.
Figures
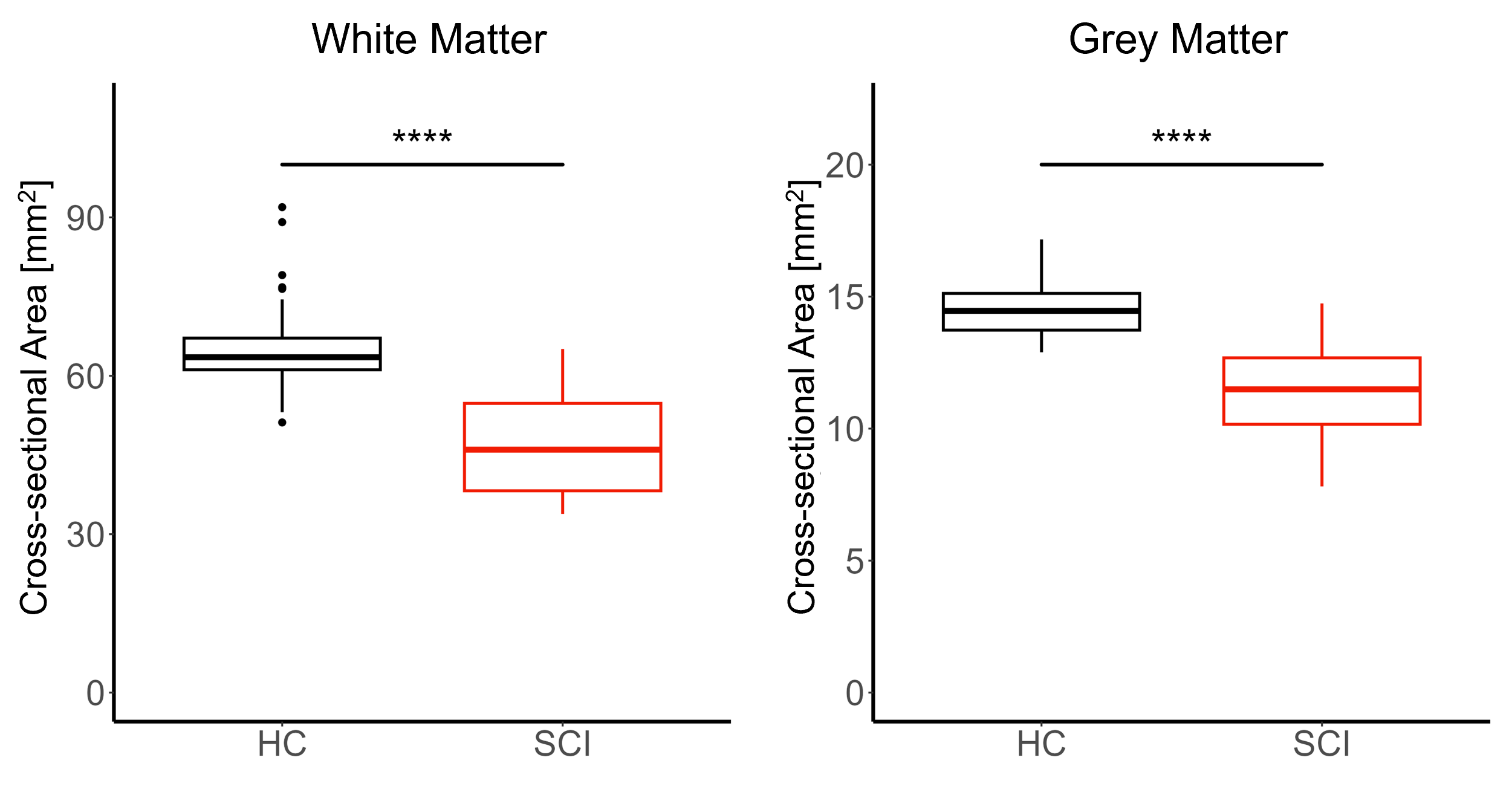
Figure 1: Cervical cord atrophy in SCI patients. Box and whisker plots of the cross-sectional areas of the white and grey matter in the cervical cord of healthy controls (HC) and SCI patients, averaged across C1-C3 levels. ****p < 0.001.
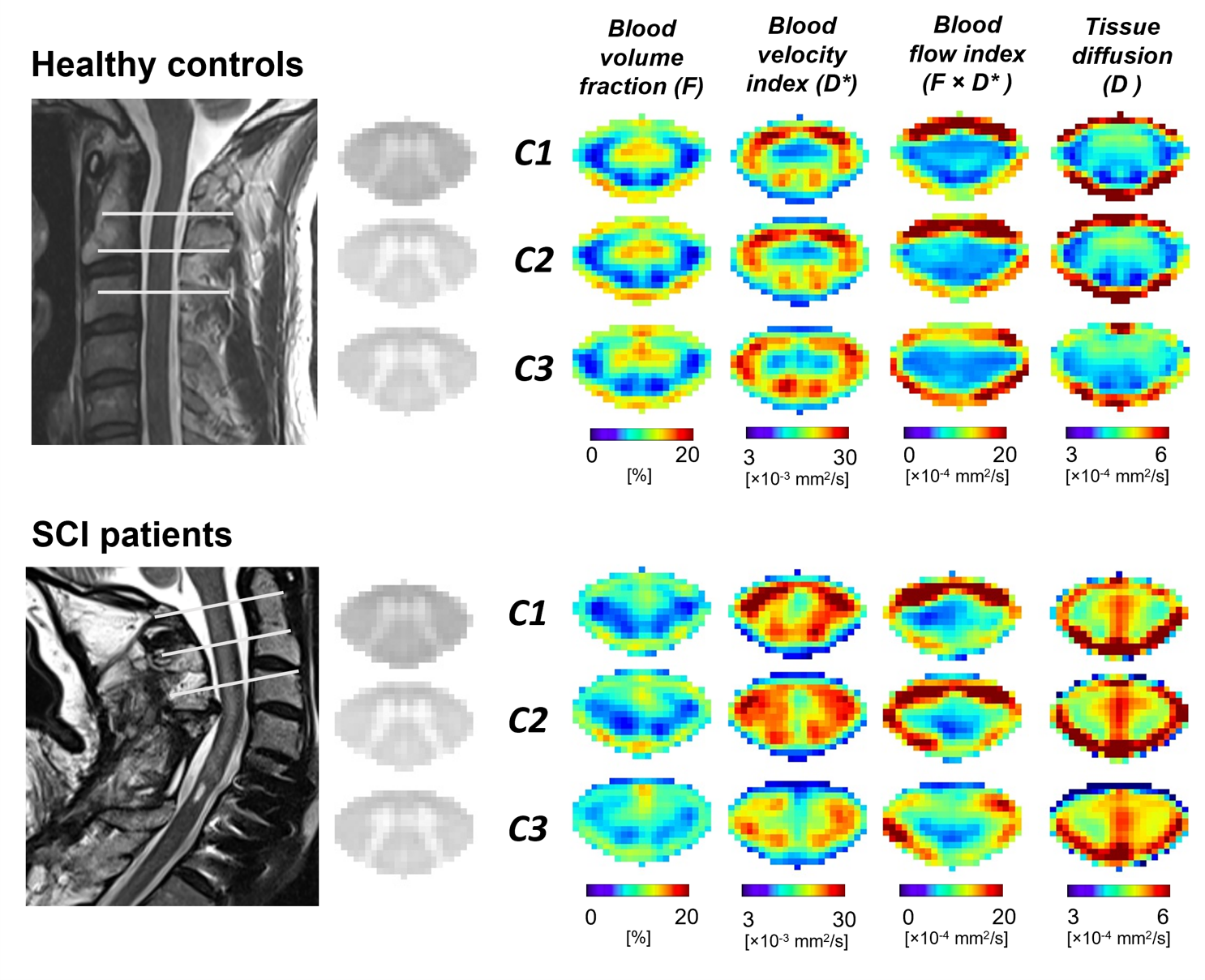
Figure 2: IVIM maps healthy controls and SCI patients represented in the PAM50 space. Sagittal T2-weighted image (of a representative subject of each group), axial T2*-weighted images, and IVIM maps (averaged across subjects), including microvascular volume fraction $$$F$$$ [%], blood velocity-related parameter $$$D^*$$$ [mm2/s], blood flow-related parameter $$$F·D^*$$$ [mm2/s], and tissue diffusion coefficient $$$D$$$ [mm2/s] at C1-C3 levels. Maps were averaged across diffusion-encoding directions and subjects in healthy controls and SCI patients.
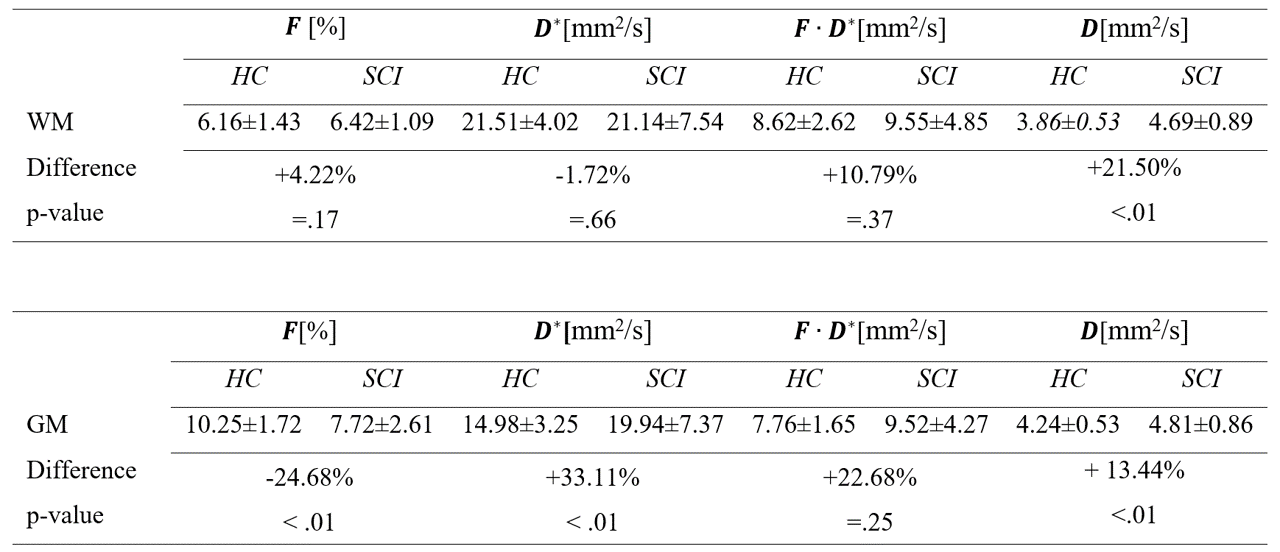
Table 1: IVIM parameters (mean and standard deviations across subjects) in the white matter (WM) and grey matter (GM) of spinal cord injury (SCI) patients and healthy controls (HC), along with the relative differences between the two groups and p-value of the statistical t-tests. IVIM parameters were extracted in subject space slice-wise and averaged across slices covering C1-C3 levels.
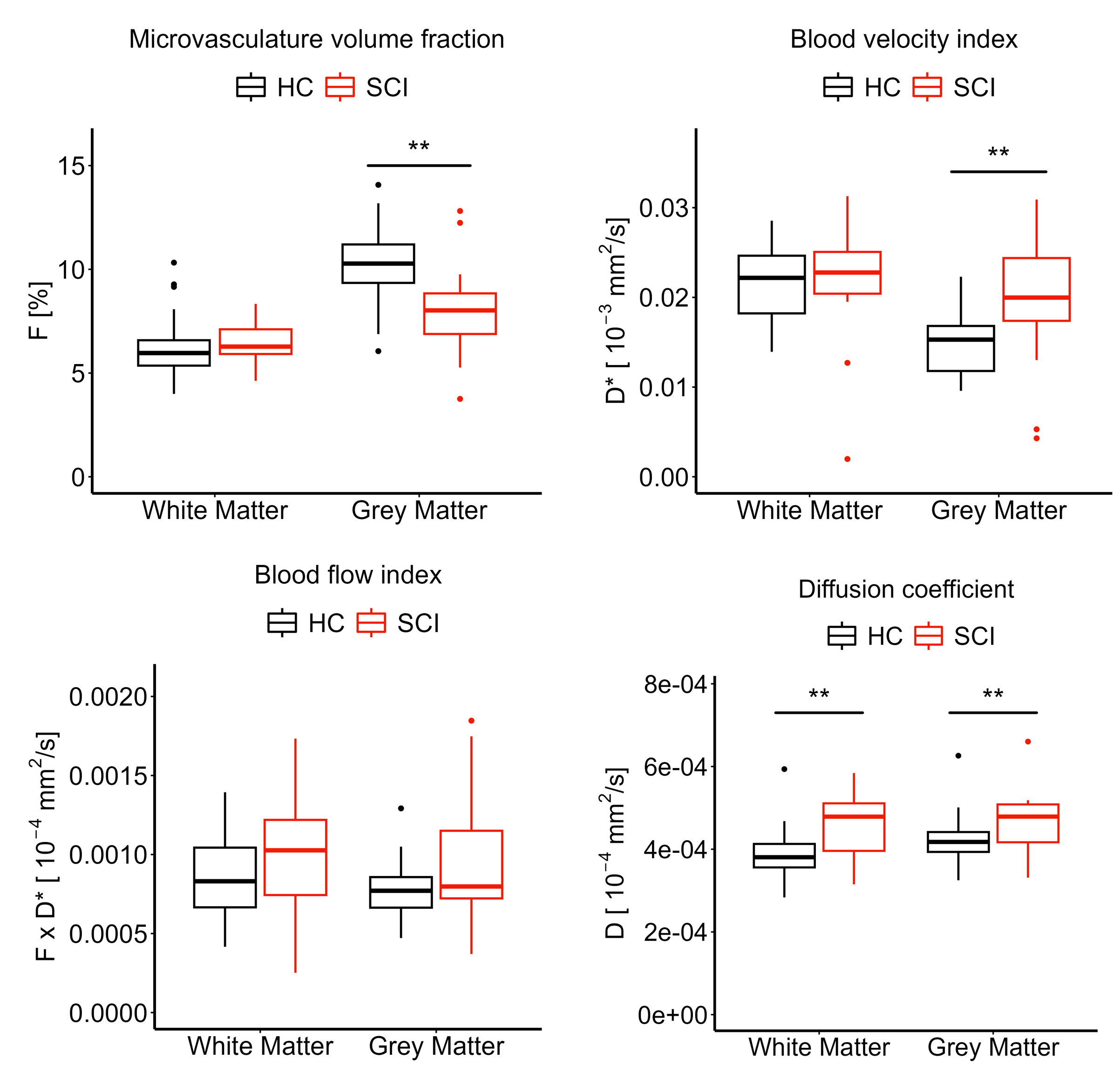
Figure 3: Comparing IVIM parameters in SCI patients and healthy controls (HC). Box and whisker plots of IVIM parameters (microvascular volume fraction $$$F$$$ [%], blood velocity-related parameter $$$D^*$$$ [mm2/s], blood flow-related parameter $$$F·D^*$$$ [mm2/s], and tissue diffusion coefficient $$$D$$$ [mm2/s]) averaged across slices over C1-C3 levels in HC and SCI groups. **p < 0.01.