2327
The effect of long label duration on hybrid multi-delay PCASL of time-encoded and variable-TR schemes in Moyamoya disease1Department of Molecular Imaging & Diagnosis, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Philips Japan, Tokyo, Japan, 3Division of Radiology, Department of Medical Technology, Kyushu University Hospital, Fukuoka, Japan, 4Department of Clinical Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 5Department of Radiological Technology, Faculty of medical sciences, Kyoto College of Medical Science, Kyoto, Japan, 6C.J. Gorter MRI Center, Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 7Philips Healthcare, Best, Netherlands
Synopsis
Keywords: Stroke, Arterial spin labelling
Motivation: Accurate quantification of cerebral perfusion in Moyamoya disease using ASL is challenging.
Goal(s): To investigate the effect of long LD in hybrid multi-delay PCASL of time-encoded and variable TR schemes.
Approach: Patients with Moyamoya disease were scanned with hybrid schemes with respectively 12 delays obtained with LD of 2s (LD2s) and 9 delays obtained with LD of 3s (LD3s).
Results: The tSNR of LD3s was significantly higher than that of LD2s, especially in the regions with prolonged ATT. CBF measured by both methods showed a strong correlation, but the differences in CBF became larger for longer ATT.
Impact: The use of a long LD of 3s for hybrid multi-delay PCASL provides higher SNR compared to that of 2s, and may be useful for assessing cerebral perfusion with prolonged ATT as often seen in Moyamoya disease.
Introduction
Cerebral perfusion status in Moyamoya disease can be assessed non-invasively using ASL, with a multi-delayed ASL approach being advantageous in Moyamoya due to the associated long arterial transit times (ATT)1. There are two time-efficient approaches for multi-delay ASL: the first is time-encoded PCASL, which can provide a high SNR, but the temporal flexibility for labelling duration (LD) and post-labelling delay (PLD) is limited due to the sub-bolus constraints; the second is variable-TR PCASL that allows arbitrary combinations of LD and PLD, which has proven to be useful for assessing cerebral perfusion in this disease2, 3; however, variable-TR PCASL is less SNR-efficient than time-encoded PCASL. By combining the time-encoded and variable-TR approaches into a hybrid scheme, the advantages of both approaches can be achieved, thereby featuring both high SNR and temporal flexibility4. To date, the typical longest LD is around 2 seconds. However, a previous study has shown that time-encoded-PCASL combined with a long-label long-delay acquisition (LD 4s, PLD 3s) is useful for accurate ATT and CBF measurements5. The aim of the present study is to investigate in Moyamoya disease the utility of a long LD of 3s within the hybrid scheme and to compare it to an LD of 2s.Methods
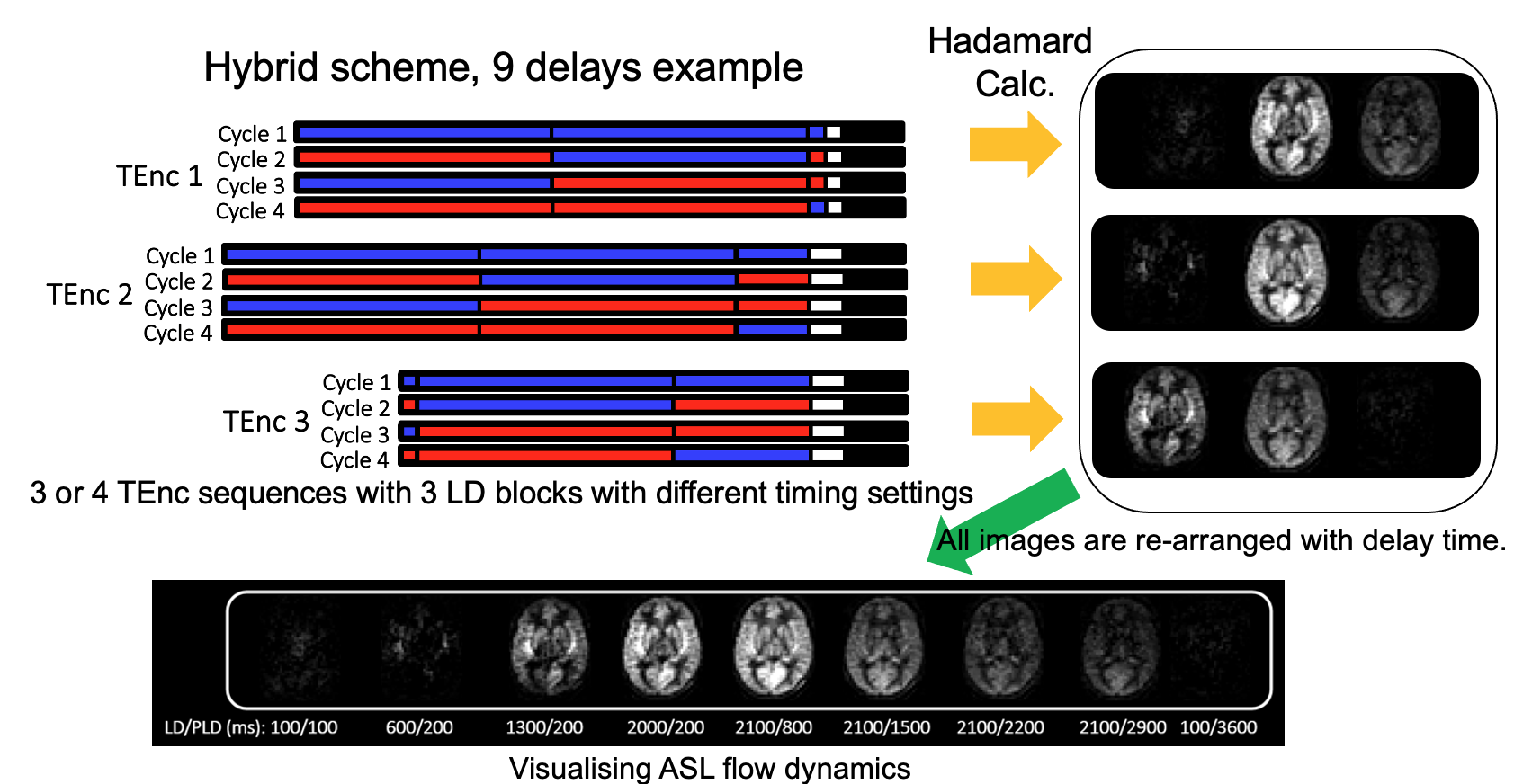
Subjects: Six consecutive inpatients with Moyamoya disease (19.0±15.4-year-old, three females) were included.Hybrid PCASL Scheme: The schematic drawings of the hybrid scheme are shown in Figure 1. The hybrid scheme comprises three or four time-encoded schemes with three LD blocks. For displaying purpose, the ASL maps are rearranged. In the first half, the LD is lengthened while the PLD is shortened and fixed, and in the second, the LD is fixed at the maximum, and the PLD is lengthened. The final phase is only meant for noise measurements.
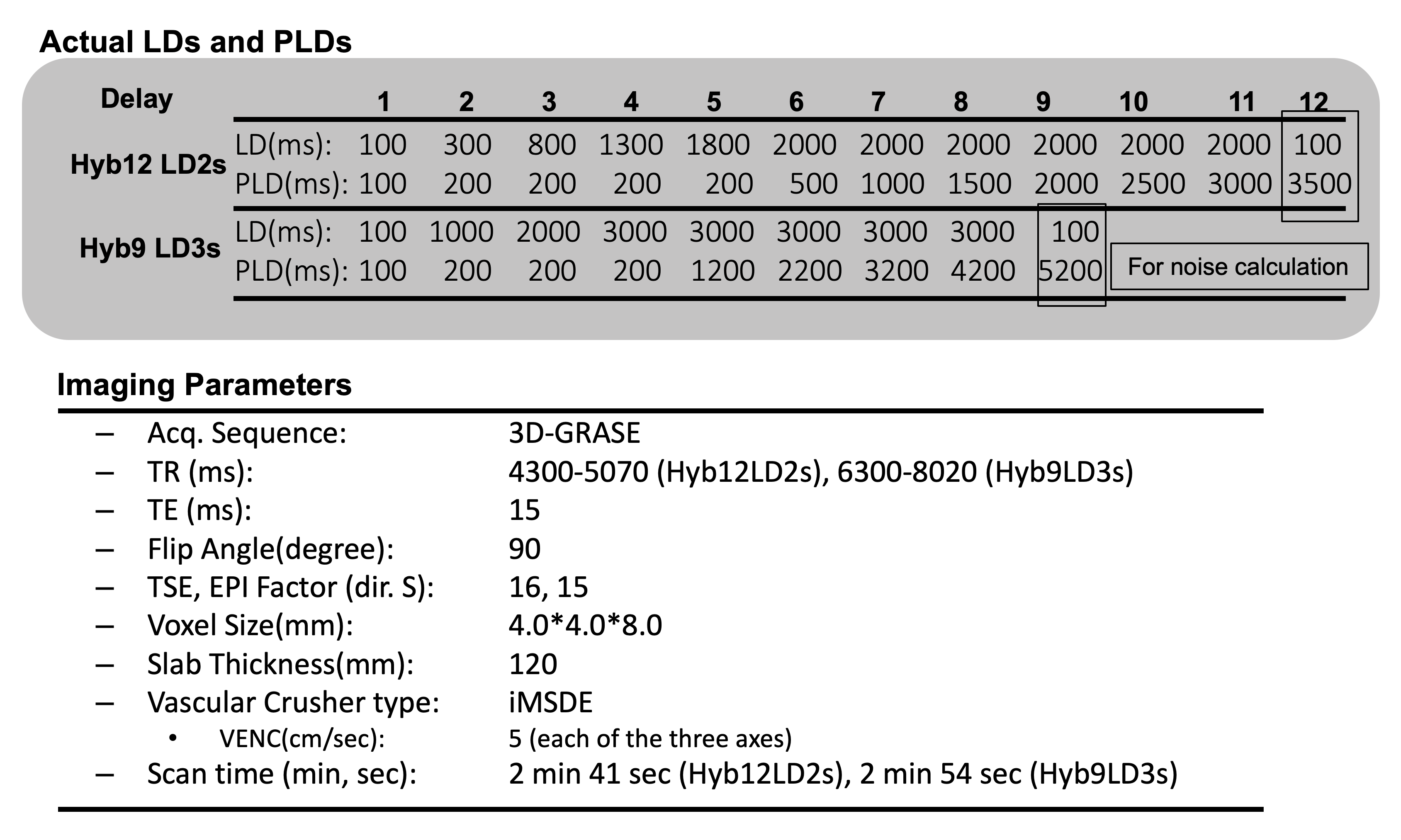
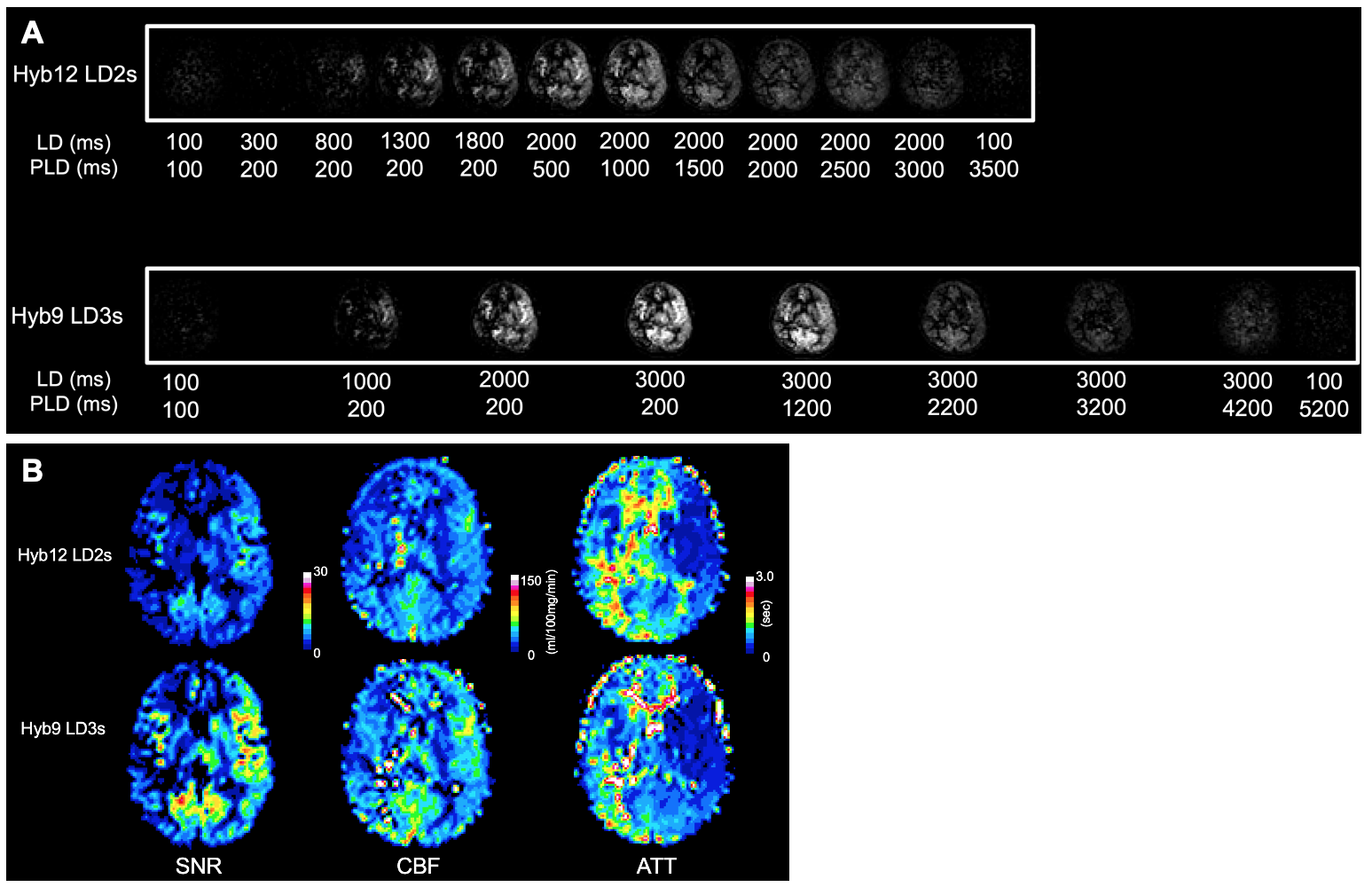
MRI: A 3T scanner (Ingenia Elition, Philips) with a 32-channel head coil was used. The MRI-protocol included: hybrid with 4x3 (12) delays obtained with LD 2s (Hyb12-LD2s), and hybrid scheme with 3x3 delays obtained with LD of 3s (Hyb9-LD3s). The actual LDs, PLDs, and other imaging parameters are summarized in Figure 2.
Quantification: CBF and ATT were calculated using a Buxton general kinetic model.
Image Analysis: All maps were normalized to the MNI space template. The SNR, CBF, and ATT in the gray matter region were measured. Temporal-SNR (tSNR), the SNR divided by the square root of the scan time, was used for fair comparison. Volumes-of-interest were obtained from a vascular territory atlas template. The measurements were performed in the anterior, middle, and posterior cerebral artery territories—with subdivision into proximal, middle and distal regions—for both left and right hemisphere.
Results
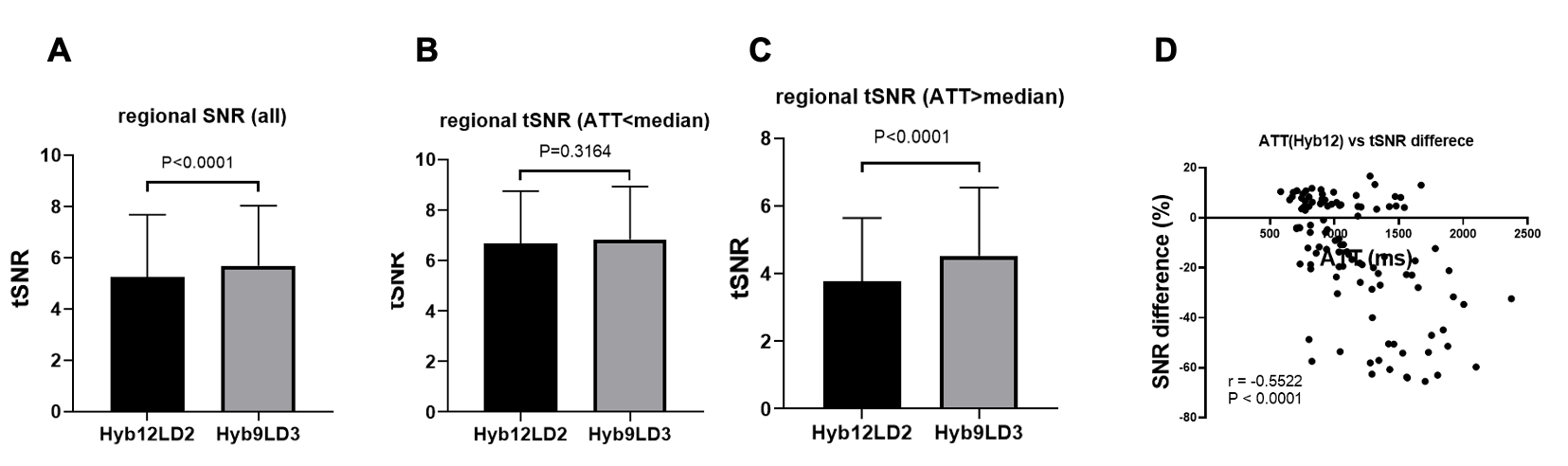
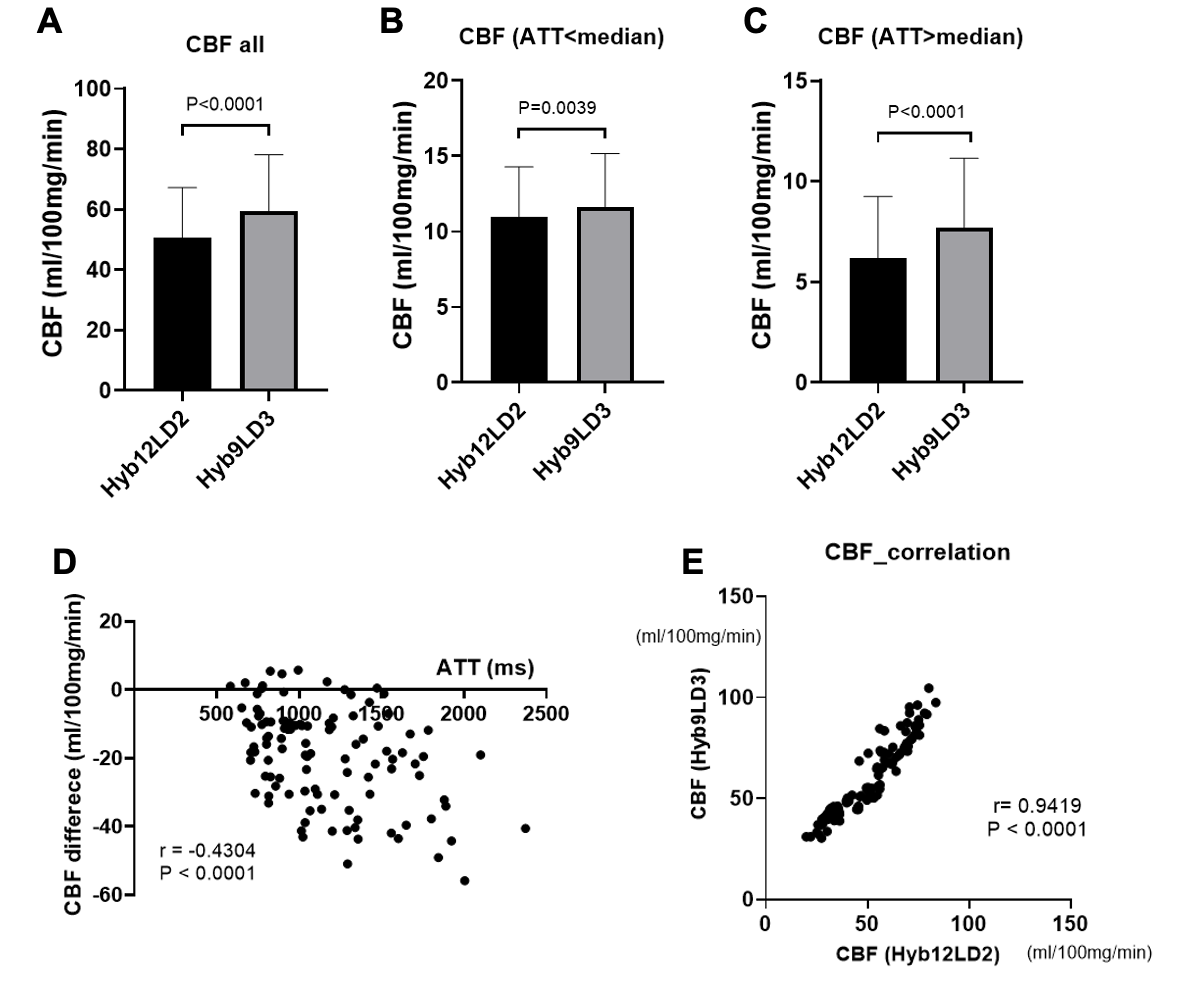
In all volumes-of-interest, the tSNR of Hyb9-LD3s was significantly higher than that of Hyb12-LD2s (P<0.0001, Figure 3). In regions where ATT was shorter than the median (1045.0ms), the tSNR was not significantly different between the two methods (P=0.32). In regions where ATT was longer than the median (1045.0ms), the tSNR of Hyb9-LD3s was significantly higher than that of Hyb12-LD2s (P<0.0001). Differences in tSNR are larger for longer ATT (correlation r=-0.55, P<0.0001). The CBF of Hyb9-LD3s was significantly higher than that of Hyb12-LD2s in all volumes-of interest (P<0.0001, Figure 4), in the volumes with shorter ATT (P=0.0039), and in the volumes with longer ATT (P<0.0001). The differences in CBF became larger with longer ATT (correlation r=-0.43, P<0.0001). The CBF measured by both methods showed a strong correlation (r=0.94; P<0.0001). Figure 5 shows a representative case of Moyamoya disease. In this patient, SNR of the whole brain is higher for Hyb9-LD3s than Hyb12-LD2s. Note that signal in the brain is better depicted in the latest time points by Hyb9-LD3s.Discussion
The results of the present study show that tSNR was increased by using the long LD of 3s. The increase in tSNR was significant in regions where ATT is longer than the median, indicating the usefulness of this scheme for application in subjects with slow flow, such as Moyamoya disease. There was a significant difference in CBF measured by both methods. The higher SNR obtained with the long LD might have resulted in more accurate fitting.Conclusion
The hybrid scheme with a long LD provides higher SNR, especially in the brain tissues where ATT is prolonged. The hybrid scheme with long LD is therefore preferred for accurate assessment of cerebral perfusion status in Moyamoya disease.Acknowledgements
No acknowledgement found.References
1. Setta K, Matsuda T, Sasaki M, et al. Diagnostic Accuracy of Screening Arterial Spin-Labeling MRI Using Hadamard Encoding for the Detection of Reduced CBF in Adult Patients with Ischemic Moyamoya Disease. AJNR Am J Neuroradiol 2021;42:1403-14092.
2. Obara M, Togao O, Wada T, et al. Pseudo-continuous arterial spin labeling using multiple label- and post-label duration with dynamically optimized background suppression. Proc Int Soc Magn Reson Med 2021:8703.
3. Togao O, Obara M, Kikuchi K, et al. Assessment of cerebral perfusion in Moyamoya disease with dynamic pCASL using a variable-TR scheme with optimized background suppression. Proc Int Soc Magn Reson Med 2022:46064.
4. Togao O, Obara M, Yamashita K, et al. Hybrid multi-delay PCASL of time-encoded and variable-TR schemes for the assessment of cerebral perfusion in Moyamoya disease. Proc Int Soc Magn Reson Med 2023;23:11945.
5. Ishida S, Kimura H, Isozaki M, et al. Robust arterial transit time and cerebral blood flow estimation using combined acquisition of Hadamard-encoded multi-delay and long-labeled long-delay pseudo-continuous arterial spin labeling: a simulation and in vivo study. NMR Biomed 2020;33:e4319
Figures