2325
Both hypoperfusion and structural impairment associates with cognitive decline in HR-NICE patients1School of Future Technology, Xi'an Jiaotong University, Xi'an, China, 2Department of Rehabilitation Medicine, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China, 3Department of Neurology, First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China, 4Department of Dental Medicine, Xi'an Jiaotong University, Xi'an, China, 5GE HealthCare MR Research, Beijing, China, 6Department of Radiology Medicine, First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China
Synopsis
Keywords: Stroke, Neuroscience, cerebral blood flow; gray matter volume; gray matter asymmetry; high-risk non-disabling ischemic cerebrovascular events;
Motivation: Patients with high-risk non-disabling ischemic cerebrovascular events (HR-NICE) are recommended as the key population for stroke prevention. However, the functional impairment and underlying neural mechanisms are rarely investigated in this cohort.
Goal(s): We attempt to confirm the neural and cognitive impairment and explain the mechanism of cognitive impairment in aspects of both hypoperfusion and cortical abnormality in HR-NICE patients.
Approach: Cerebral blood flow, grey matter volume and asymmetry were calculated based on MR perfusion and anatomical data.
Results: Hypoperfusion and cortical abnormality are significant in HR-NICE patients, these neural impairments are robustly correlated with cognitive decline.
Impact: Our study confirmed the existence of early neural damage in HR-NICE patients, which is reflected in multiple aspects of hypoperfusion, grey matter atrophy and decreased asymmetry. These abnormalities collectively contribute to cognitive decline, especially in patients with left involvement.
Introduction
High-risk non-disabling ischemic cerebrovascular events (HR-NICE) patients are considered to be at a great risk of stroke recurrence and mortality. Studies have revealed that over one-third of HR-NICE patients experience a recurrent stroke within a three-month period.1 Combining with persistent intracranial artery stenosis, the occurrence of minor stroke or transient ischemic attack (TIA) in HR-NICE patients hints the existence of hypoperfusion and even cortical abnormality, both of which are potential risk factors for cognitive decline. However, little is known about the neurological and cognitive impairment in this cohort. The current study aims to illustrate that cognitive decline occurs in HR-NICE patients as well as hypoperfusion and cortical abnormalities. Additionally, we aim to examine the role of these neuropathological conditions in contributing to the observed cognitive decline.Methods
This study was approved by the institutional review board and the written informed consent was obtained from all subjects. The study included 33 HR-NICE patients (21 left-sided and 12 right-sided involvement) that were confirmed to have steno-occlusion of unilateral large artery in the anterior circulation by digital subtraction angiography, and 33 matched health controls (HC). All subjects underwent MR examination on a 3T MRI scanner (Discovery MR750w, GE Healthcare) with a 16-channel phased-array coil. For HR-NICE patients, 3D T1-weighted imaging and arterial spin labeling scans were obtained within a week after the first occurrence of minor stroke or TIA. Montreal Cognitive Assessment (MoCA) was used to evaluate the cognitive function. Grey matter volume (GMV), asymmetry index (AI) and cerebral blood flow (CBF) were calculated on Freesurfer and SPM platforms. All results were corrected for family-wise error with a cluster-level threshold of p < .05.Results
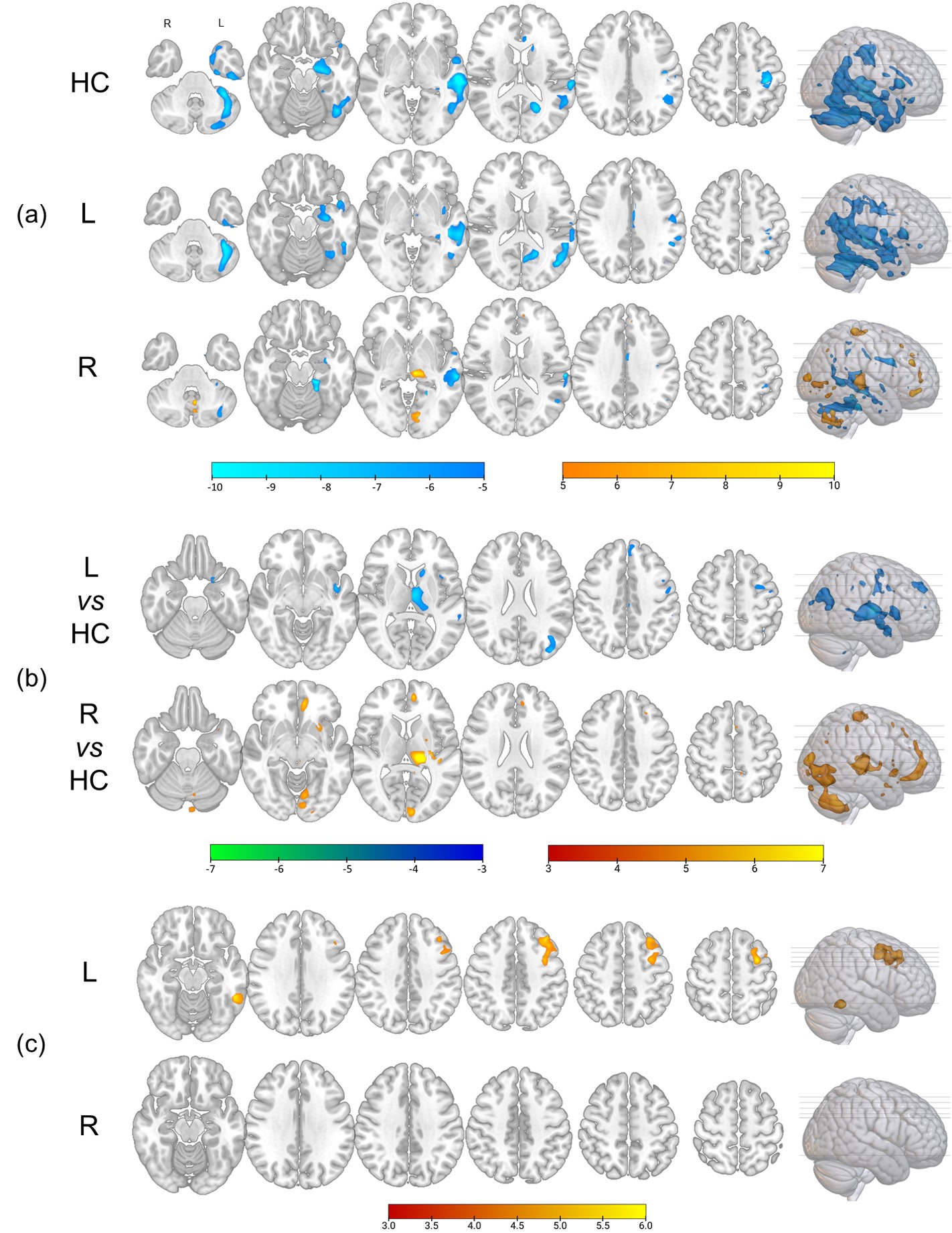
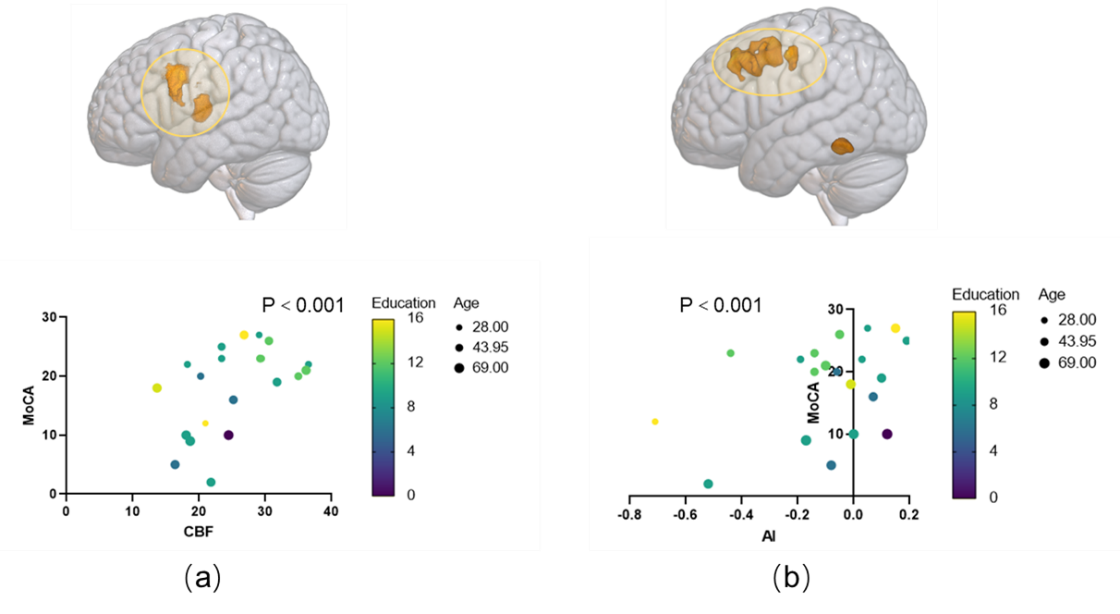
The results show a significant difference between HC and HR-NICE patients with left steno – occlusion in the total and most subitem scores of MoCA (Fig. 1). Nevertheless, patients with right steno-occlusion differ just in abstract aspect (Fig. 1). All patients present an extensive hypoperfusion in the territory of the middle cerebral artery on the affected side. A relatively higher CBF is also found in the territory of posterior circulation in patients with left–sided involvement (Fig. 2a). Correlation analysis reveals that the total MoCA score of left–sided patients is associated with the CBF of affected precentral cortex (Fig. 2b). The corresponding precentral cortex in the right hemisphere showed an increased GMV than HC. However, no significant results survive in right–side involved patients (Fig. 3). the AI in extensive areas is differed between HC and patients of two groups. In addition, the AI of middle frontal cortex is significantly correlated with MoCA in left-sided patients (Fig. 4). Multiple liner regression analysis demonstrates a robust contribution of CBF of the prefrontal cortex and AI of the middle frontal cortex to MoCA score (Fig. 5, P < 0.001, R = 0.971).Discussion
The combination of minor stroke or TIA with large artery steno-occlusion in HR-NICE patients is not currently considered as severe cerebral infarction or functional disability. However, our research indicates that the cognitive performance of HR-NICE patients is significantly poorer compared to healthy individuals, suggesting functional impairment in this critical pre-stroke state.Observations reveal that HR-NICE patients, affected by steno-occlusion, exhibit noticeable hypoperfusion in extensive regions of the frontal, temporal, and parietal lobes. This insufficient blood flow fails to meet the energy demands necessary for maintaining normal neural function.2 Additionally, cortical structural alterations are observed in left-sided patients, characterized by compensatory increased volume in the unaffected hemisphere and decreased asymmetry across the brain. These changes in gray matter volume directly lead to structural imbalances and adversely affect the asymmetrical organization, which serves as the anatomical basis for the functional dominance of the left hemisphere.3, 4 Multiple regression models consistently highlight the role of hypoperfusion and structural abnormalities in cognitive decline, providing further evidence for the various mechanisms through which neurological damage contributes to cognitive impairment.
Besides, less severe impairments in neurological and functional aspects are observed in right-sided patients, potentially due to the non-dominant role of the right hemisphere in cognitive processing. In contrast, the imbalance between energy supply and demand may be more pronounced in patients with left-side involvement. This could explain the compensatory hyperperfusion observed in the territory of the posterior circulation in these left-side involved patients, which is closely related to ischemia.
Conclusion
The current research reveals the neuropathological changes of HR-NICE patients has already occurred in aspects of hypoperfusion and cortical abnormality, both of which are significantly contributed to cognitive impairment, especially in patients with left-sided involvement.Acknowledgements
This project would not have been possible without the cooperation and support of all colleagues.References
1. Tan S and Choi PMC. Mild in Name but Not in Nature. Stroke 2021; 52: 2005-2006. 2021/05/06. DOI: 10.1161/strokeaha.121.035003.
2. Gottesman RF and Hillis AE. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol 2010; 9: 895-905. 2010/08/21. DOI: 10.1016/s1474-4422(10)70164-2.
3. Saltoun K, Adolphs R, Paul LK, et al. Dissociable brain structural asymmetry patterns reveal unique phenome-wide profiles. Nat Hum Behav 2023; 7: 251-268. 2022/11/08. DOI: 10.1038/s41562-022-01461-0.
4. Güntürkün O, Ströckens F and Ocklenburg S. Brain Lateralization: A Comparative Perspective. Physiol Rev 2020; 100: 1019-1063. 2020/04/03. DOI: 10.1152/physrev.00006.2019.
Figures
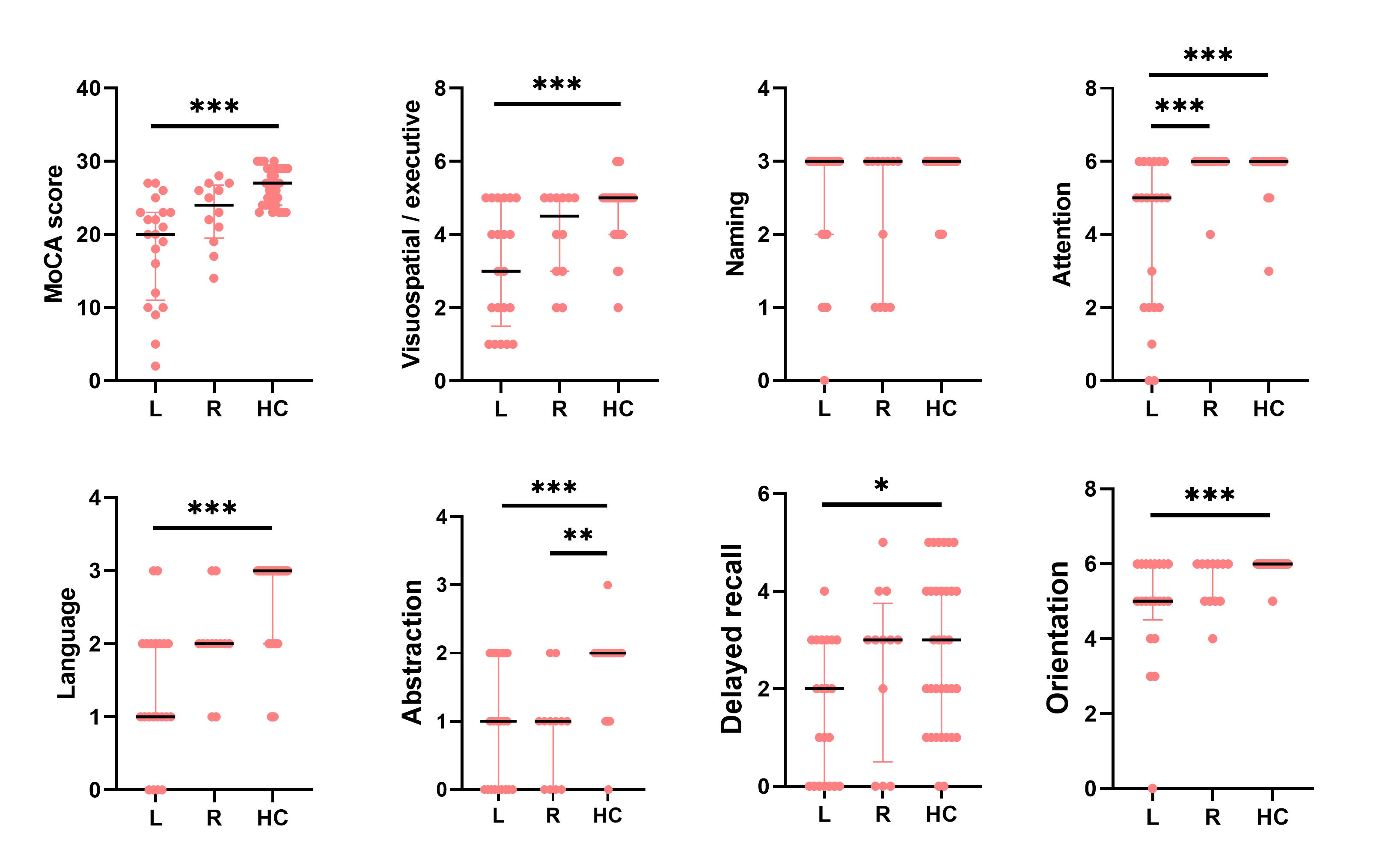
Fig. 1 Comparison of total and subitem MoCA scores in patients with left and right involvement and HC. Patients with left involvement show a significantly poor cognitive performance in all aspects expect naming, while right-involved patients just differ in the aspect of abstraction. MoCA, Montreal Cognitive Assessment; L, patients with left involvement; R, patients with right involvement; HC, health controls; *, P < 0.05; **, P < 0.01; ***, P <0.001.
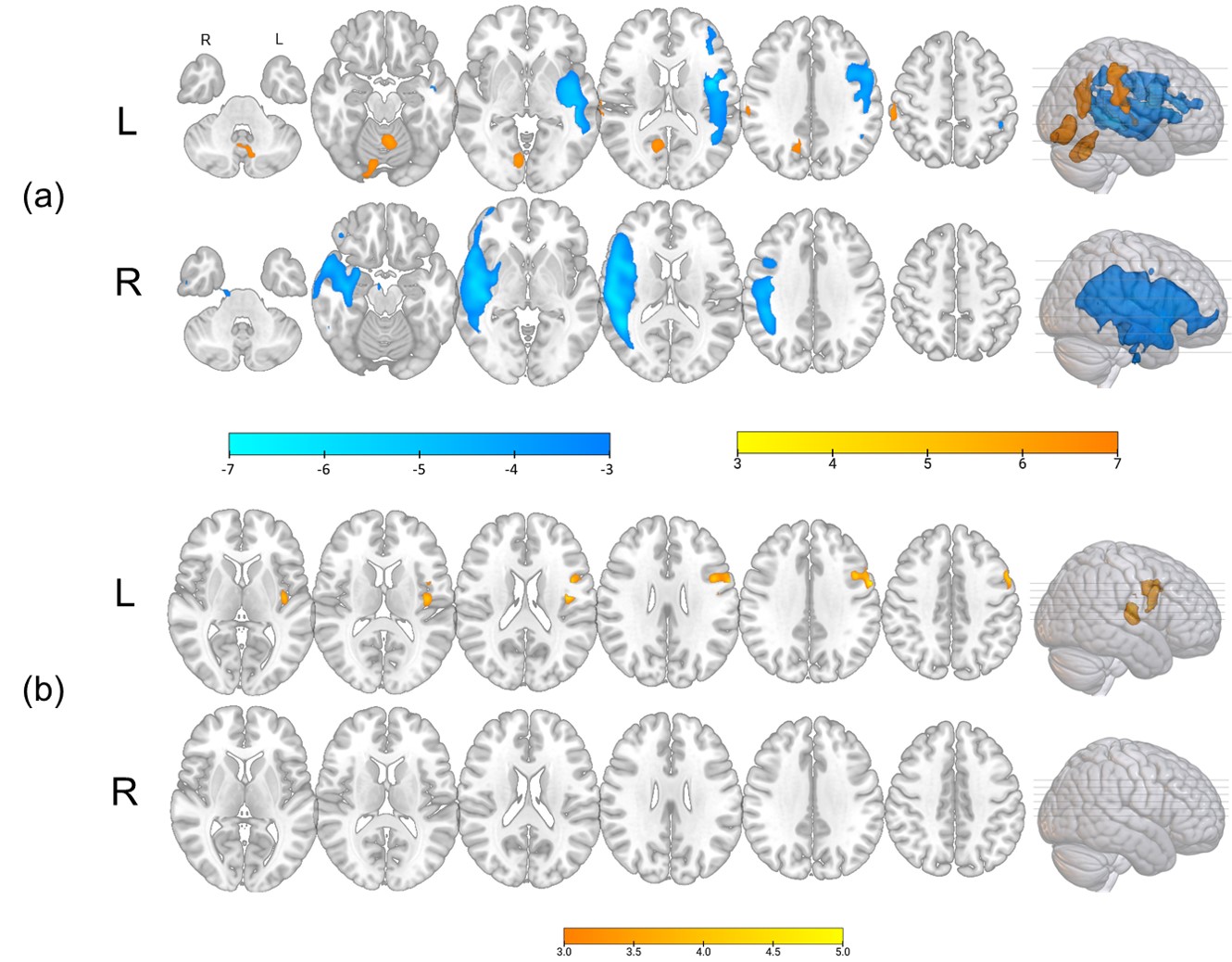
Fig. 2 Perfusion condition of HR-NICE patients compared to HC and its correlation with MoCA score. (a) hypoperfusion (cool) and hyperperfusion (warm) in HR-NICE patients of left or right involvement. (b) the cerebral blood flow of precentral and superior temporal cortex is correlated with total MoCA score in left-sided patients. L, left-involved patients; R, right-involved patients; HR-NICE, high-risk non-disabling ischemic cerebrovascular events; MoCA, Montreal Cognitive Assessment.