2323
Increased T2 value suggest the NA-CST degeneration following stroke proved by multiple overlapping-echo detachment qMRI1Functional Magnetic Resonance and Molecular Imaging Key Laboratory of Henan Province, Department of Magnetic Resonance Imaging, the First Affiliated Hospital of Zhengzhou University, Zhengzhou University, Zhengzhou, China, 2Department of Electronic Science, Fujian Provincial Key Laboratory of Plasma and Magnetic Resonance, School of Electronic Science and Engineering, National Model Microelectronics College, Xiamen University, Xiamen, China, 3The Laboratory «MRT TECHNOLOGIES», The Institute International Tomography Center of the Russian Academy of Sciences, Novosibirsk, Russian Federation, 4Pingdingshan College, Pingdingshan, China, 5Philips Healthcare, Beijing, China
Synopsis
Keywords: Stroke, Stroke
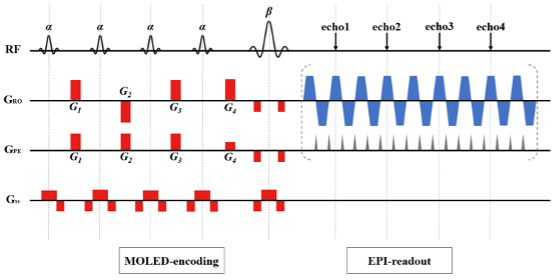
Motivation: Stroke patients commonly face challenges during clinical magnetic resonance imaging (MRI) examinations due to loss of consciousness and involuntary movements. This study aims to address these challenges using a self-developed ultra-fast, multiple overlapping-echo detachment (MOLED) quantitative magnetic resonance technology.
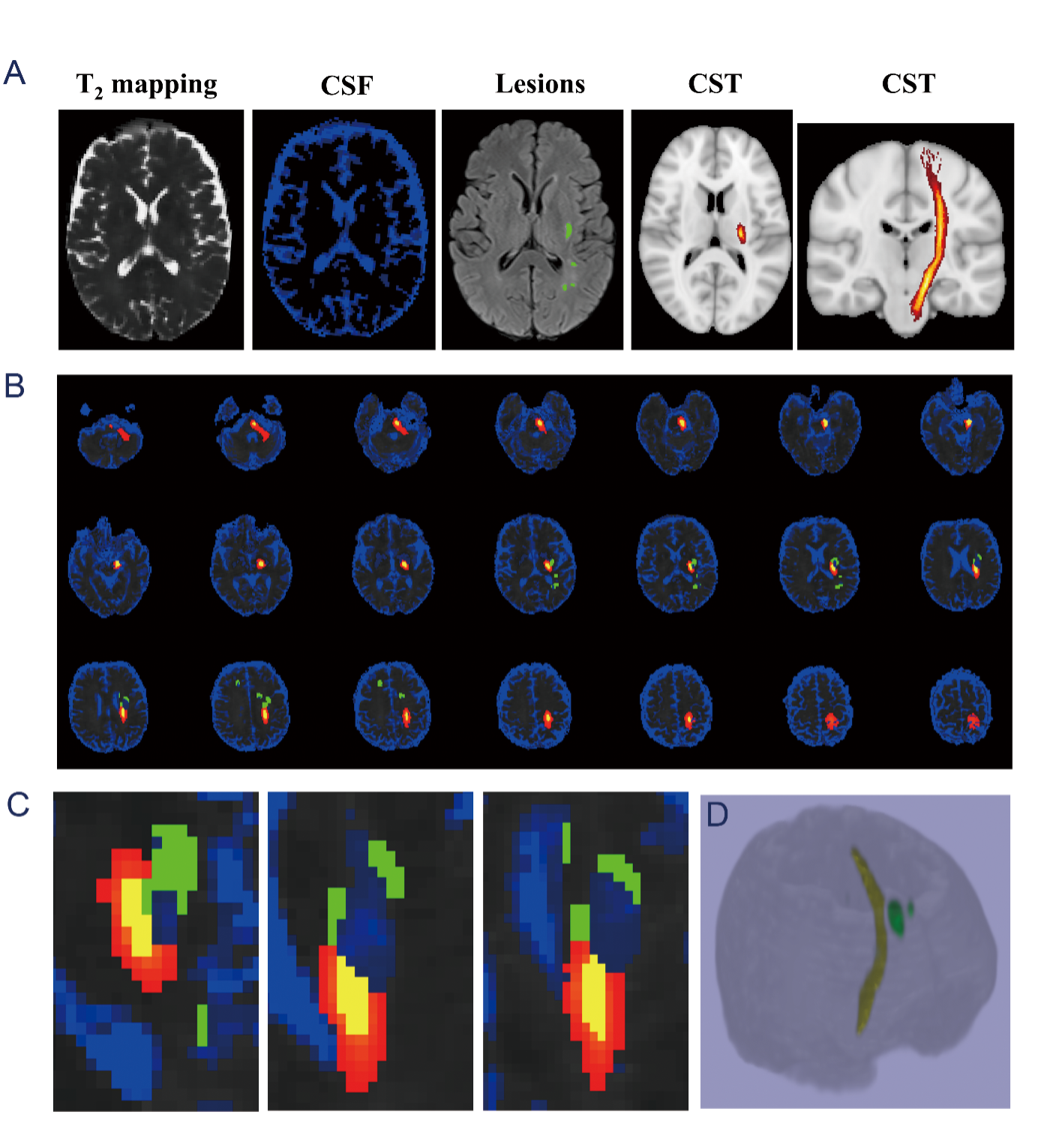
Goal(s): Through this technology, we seek to quantitatively detect potential damage to the motor-related normal-appearing corticospinal tract (NA-CST) following stroke.
Approach: Total 79 patients underwent routine scan and MOLED. A deep learning network was utilized for quantitative image reconstruction.
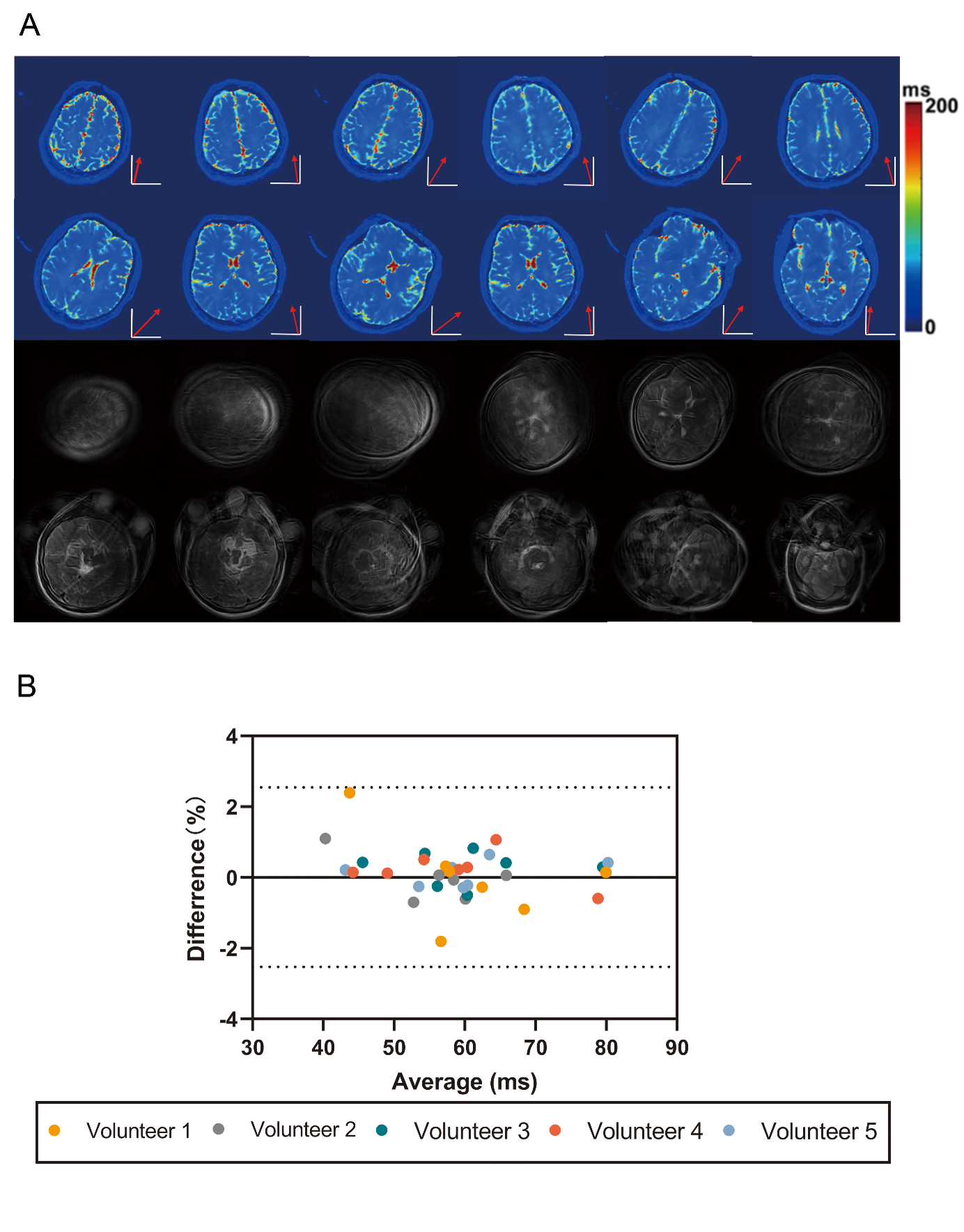
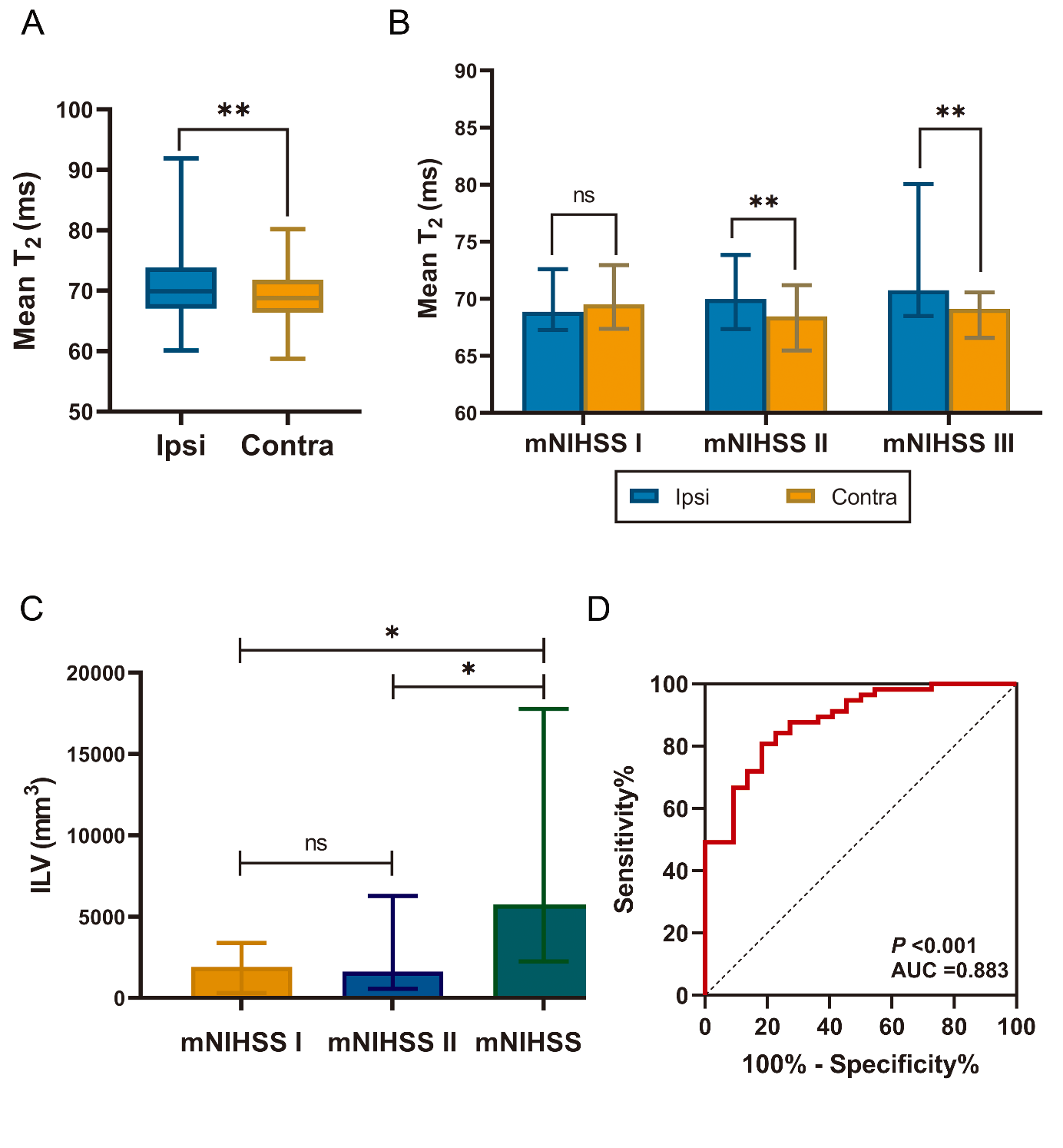
Results: MOLED T2 imaging showed high accuracy and repeatability, was unaffected by head motion, correlated with motor dysfunction severity, and predicted motor impairment post-stroke.
Impact: The MOLED technique quickly and accurately quantifies imaging in stroke patients with involuntary movements and helps monitor post-stroke motor impairment progression.
Acknowledgements
No acknowledgement found.References
No reference found.Figures