2322
DSC-2500msASL Mismatch may distinguishes between transient ischemic attack and stroke in intracranial stenosis1Department of MRI, Shaanxi Provincial People’s Hospital, Xi'an, China, 2Shaanxi Provincial People’s Hospital, Xi'an, China, 3Philips Helathcare, Xi'an, China
Synopsis
Keywords: Stroke, Arterial spin labelling
Motivation: Cerebral perfusion-weighted imaging (PWI) can be used to characterize differences in hemodynamic characteristics between transient ischemic attack (TIA) and stroke populations, but little is known about the differences between DSC and ASL.
Goal(s): this study to investigate the differential hemodynamic characteristics of the corresponding regions of the middle cerebral artery (MCA) in patients with ischemic stroke and TIA, and to establish a prediction model for ischemic stroke.
Approach: Dynamic Susceptibility Contrast (DSC) and Arterial Spin Labeling (ASL)
Results: The results indicate that Hyperhomocysteinemia and DSC-2500msASL mismatch can be used to identify patients with TIA and stroke.
Impact: We found that differences in blood perfusion in stroke and TIA patients, especially DSC-2500msASL mismatch may be a biological marker of stroke, which provides a scientific basis for screening high-risk TIA patients and early clinical intervention.
Introduction
Intracranial atherosclerotic stenosis (ICAS), especially the middle cerebral artery (MCA) involvement, is the main cause of acute ischemic stroke (AIS) or transient ischemic attack (TIA)[1-2]. However, TIA patients have a higher chance of subsequent ischemic stroke, which seriously affects the survival status of TIA patients [3-4]. The occurrence of stroke is related to the vascular lumen characteristics, plaque characteristics and cerebral blood flow defects of ICAS[5]. Previous studies used high-resolution magnetic resonance imaging (HRMRI) to characterize plaque features and dynamic sensitivity contrast-enhanced (DSC) perfusion-weighted imaging (PWI) to reflect hemodynamic injury[6]. However, there are no studies on the difference in DSC and ASL perfusion to characterize the hemodynamic changes in patients with intracranial artery stenosis. Therefore, DSC and ASL were used to investigate the differential hemodynamics of MCA in patients with ischemic stroke and TIA, and tried to establish a predictive model of ischemic stroke together with clinical risk factors in this study.Materials and Methods
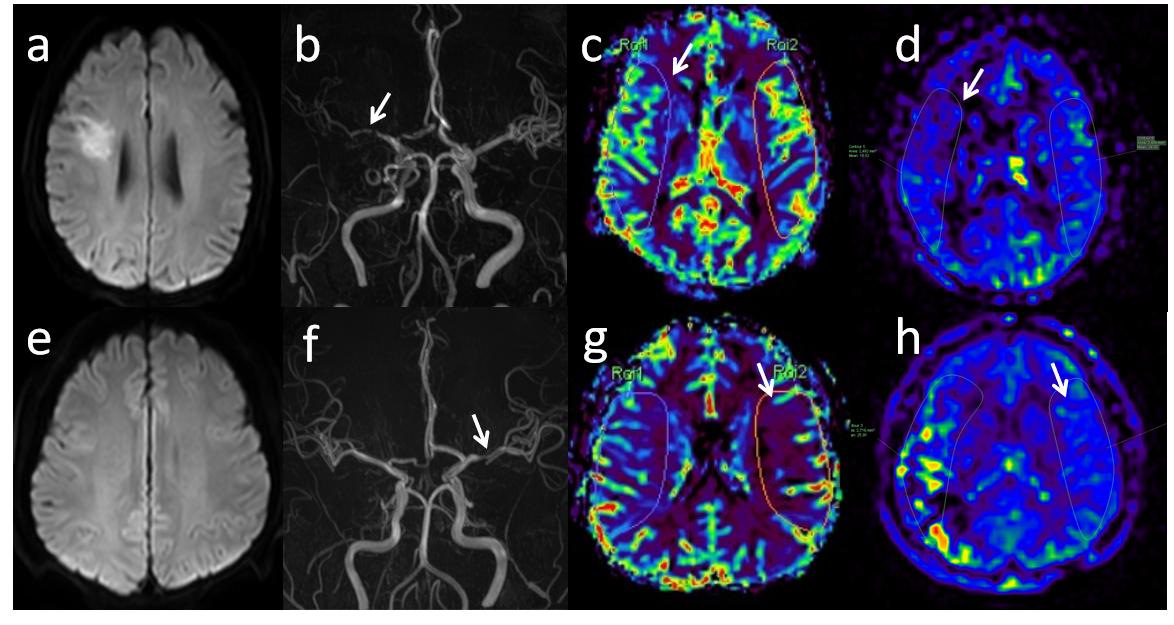
Consecutive patients with sICAS were retrospectively collected from October 2020 to December 2021. All patients underwent MR imaging using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare,) with a 32-channel head coil. A total of 32 participants were finally evaluated, and 12/20 were assigned to TIA/stroke group (table 1). Two experienced neuroradiologists were blinded to any clinical information, evaluated blood perfusion information in the MCA area on the DSC images and ASL (2-PLD: 1500 ms, 2500 ms) images, mirror measured CBF on the affected and unaffected side. And to define the perfusion reduction as: DSC-Hypoperfusion: (DSC-rCBFa - DSC-rCBFu)/DSC-rCBFa≥10%;1500msASL-Hypoperfusion:(1500msASL-CBFa - 1500msASL-CBFu)/1500msASL-CBFa≥10%;2500msASL-Hypoperfusion:(2500msASL-CBFa - 2500msASL-CBFu)/2500ASL-CBFa≥10%. If the CBF perfusion reduction of the above sequence is inconsistent, it is defined as a perfusion mismatch. Logistic regression (binary variables) analyses were performed to assess the different features between TIA and stroke group. Variables with P values <0.05 were entered into the multivariate logistic analysis. Receiver operating characteristic (ROC) curves were used to evaluate the diagnostic performance of the different models. All tests were twosided and performed by using SPSS (version 26, IBM) where appropriate. A significant difference was assumed if p < 0.05.Results
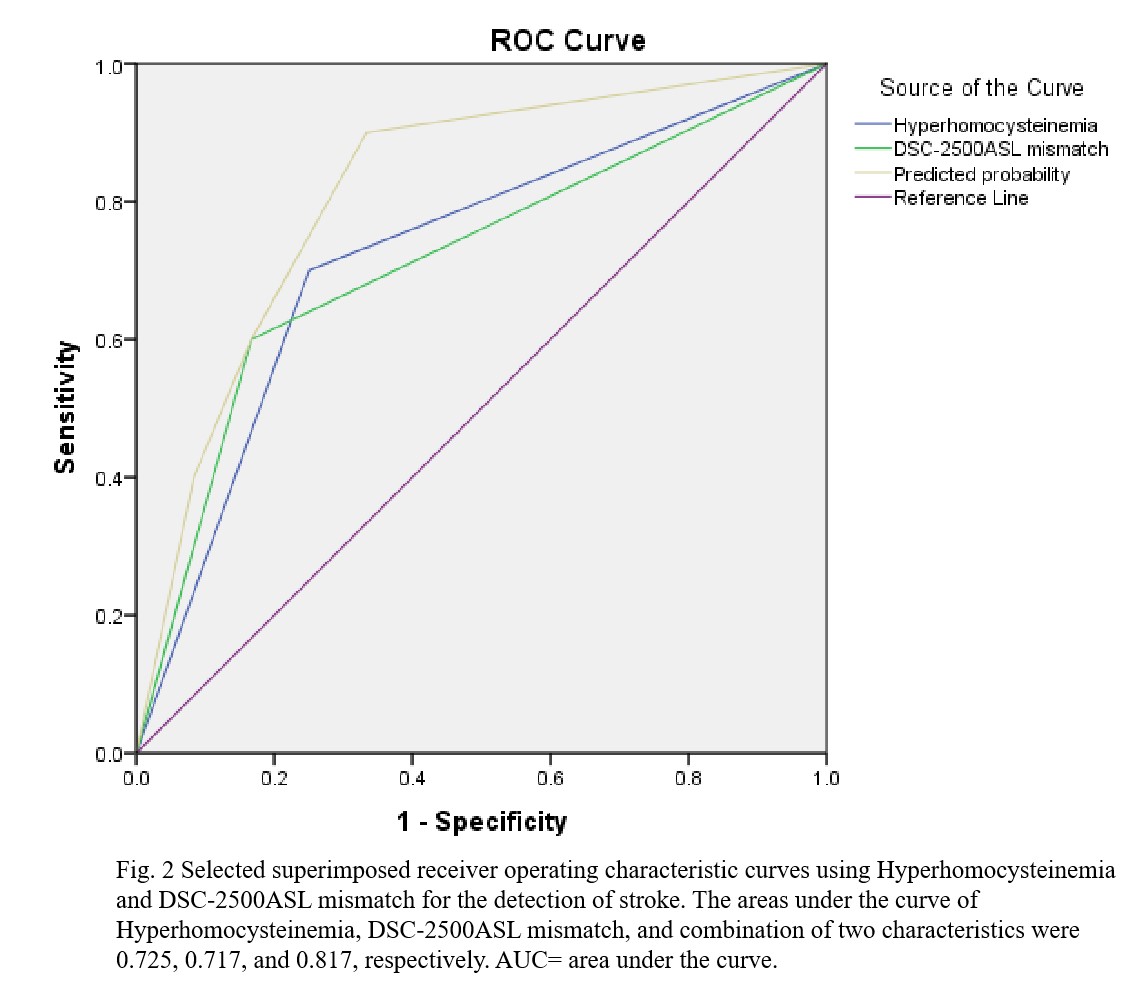
Figure 1 shown two typical examples of images and measurements. Compared with the TIA group, the stroke group had significantly more patients with hyperhomocysteinemia (Table 1). 2500msASL-Hypoperfusion, DSC-2500msASL mismatch were significantly higher in stroke than those in the TIA group (Table 2). Multivariable regression analysis revealed that hyperhomocysteinemia and DSC-2500msASL mismatch were risk factors for patients with ischemic strokeafter adjusting for clinical confounding factors ( P = 0.036, 0.043). All other indices shown no significant difference between two groups. In distinguishing between patients with ischemic stroke and TIA, the diagnostic accuracy of the combination of hyperhomocysteinemia and DSC-2500msASL mismatch was higher than that of the above single features (Figure 2). The combination had a significantly higher AUC(95%CI 0.655–0.978, AUC=0.817) than hyperhomocysteinemia (95%CI 0.539–0.911, AUC=0.725) and DSC-2500msASL mismatch (95%CI 0.533–0.900, AUC=0.717), respectively.Discussion
This study found a difference between the ASL and DSC methods in showing cerebral perfusion abnormalities in patients with ischemic stroke and TIA. Although perfusion showed little difference between the two groups when PLD was 1500ms, ASL and DSC perfusion mismatch was significantly different between stroke and TIA patients when PLD was delayed by 2500ms. This indicates the importance of two PLD to distinguish stroke from that of TIA patients, which side reflects the difference between the perfusion process and the outcome of patients with stroke and TIA. ASL at a PLD of 2500ms in this study showed more stroke patients with hypoperfusion than those demonstrated with DSC. The reason may be the occurrence of post-infarction reperfusion or open collateral circulation in these stroke patients, and the hyperperfusion (magnetized-labeled endogenous water quality is sensitive to BBB damage) is generally poor, so such unmatched patients should pay additional clinical attention[7]. However, in TIA patients, there are fewer mismatched patients and comparable perfusion abnormalities, which may indicate that TIA patients may not break the blood-brain barrier, and additional attention should be paid to TIA patients with mismatched perfusion. Therefore, the prolongation of PLD increases the difference of blood flow abnormalities between TIA patients and stroke patients. ASL with multi-PLD has more clinical value than the ASL with single PLD in intracranial stenosis evaluation.Conclusion
DSC-2500msASL mismatch may be a biological marker for screening high-risk TIA patients, and we should pay additional attention to this population for more aggressive secondary stroke measures.Acknowledgements
No acknowledgement foundReferences
[1] Chen PH,Gao S,Wang YJ,et al.Classifying Ischemic Stroke, from TOAST to CISS.CNS Neurosci Ther, 2012,18(6): 452–456. [2] Wong KS, Li H.Long-term mortality and recurrent stroke risk among Chinese stroke patients with predominant intracranial atherosclerosis. Stroke, 2003. 34(10): 2361-6.[3] Garg A, Limaye K, Shaban A,et al.Risk of Ischemic Stroke after an Inpatient Hospitalization for Transient Ischemic Attack in the United States.NEUROEPIDEMIOLOGY. 2021-01-01;55(1):40-46.[4] Mendelson, SJ; Prabhakaran, S. Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke.JAMA-J AM MED ASSOC. 2021-03-16;325(11):1088-1098. [5] Liu S, Luo Y, Wang C et al (2020) Combination of plaque haracteristics, pial collaterals, and hypertension contributes to misery perfusion in patients with symptomatic middle cerebral artery stenosis. J Magn Reson Imaging 51:195–204. [6] Liu S , Tang R , Xie W, et al. Plaque characteristics and hemodynamics contribute to neurological impairment in patients with ischemic stroke and transient ischemic attack.[J]. European radiology, 2021, 31(4):2062-2072.[7]Wang DJ , Alger JR . Qiao JX . et al . The value of arterial spir labeled perfusion imaging in acute ischemic stroke : comparison with dynamic susceptibility contrast - enhanced MRI [ J ]. Stroke ,2012,43(4):1018-1024.Figures
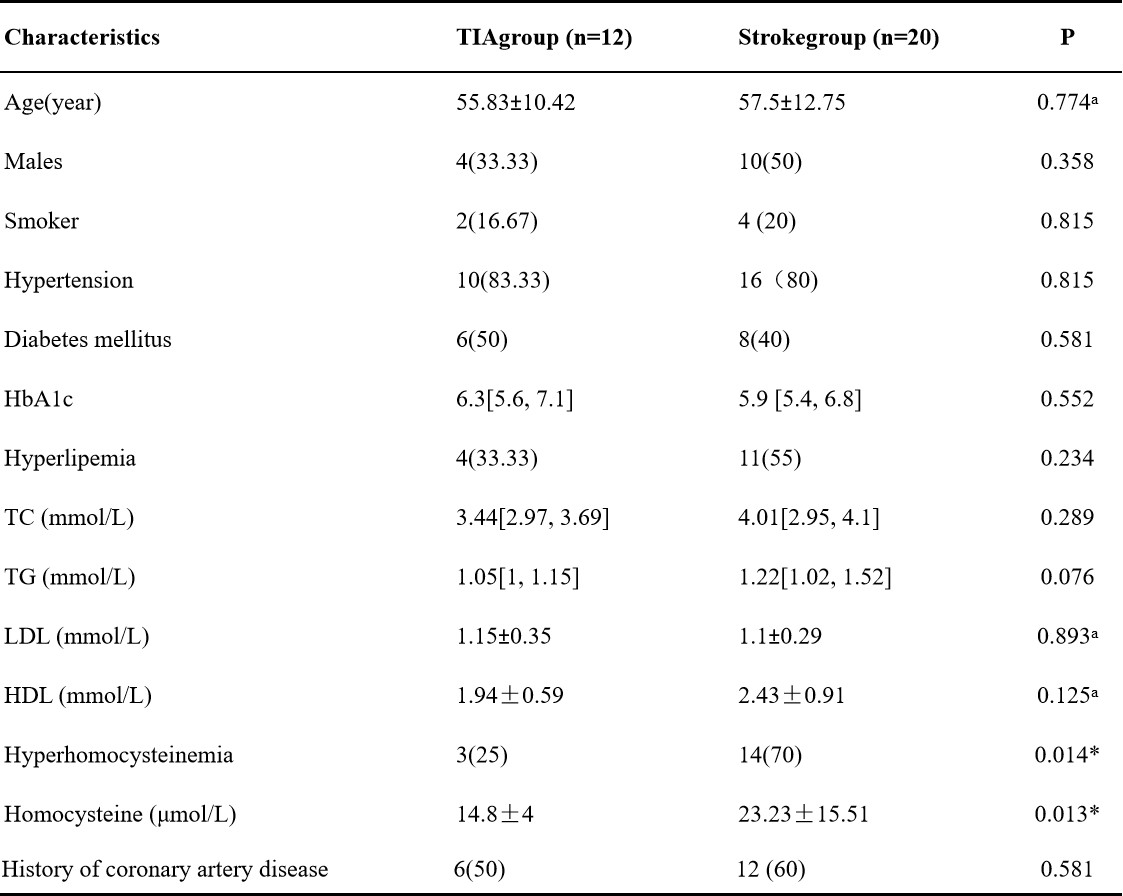
Table 1. Characteristics of patients in the two groups
All values represented as numbers (%) or or median [interquartile range] unless otherwise indicatedHbA1c = glycosylated hemoglobin; TC = total cholesterol; TG = triglyceride; HDL = high-density lipoprotein cholesterol; LDL = low-density lipoprotein cholesterol; *p < 0.05 was recognized as statistically different from the two groupsaData presented as mean ± standard deviation
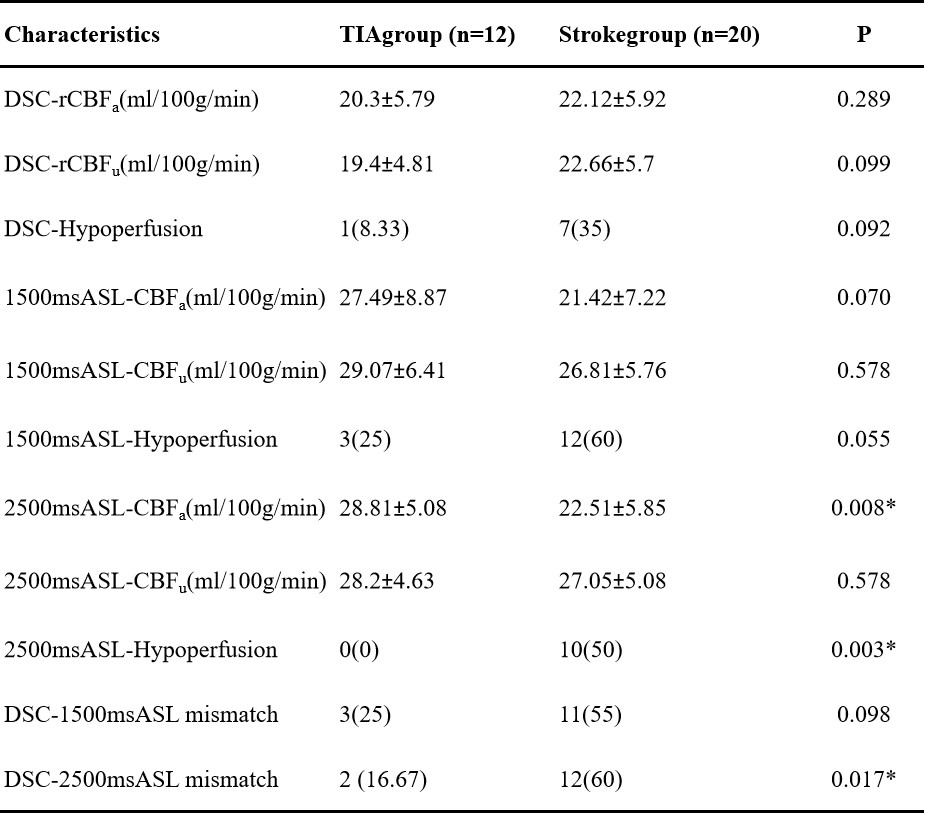
Table 2. Comparison of ASL Characteristics in the two groups
All values represented as numbers (%) or or median [interquartile range] unless otherwise indicated*p < 0.05 was recognized as statistically different from the two groupsaData presented as mean ± standard deviationa = affected side u=unaffected sideDSC-Hypoperfusion: (DSC-rCBFa - DSC-rCBFu)/DSC-rCBFa≥10%1500msASL-Hypoperfusion:(1500msASL-CBFa - 1500msASL-CBFu)/1500msASL-CBFa≥10%2500msASL-Hypoperfusion:(2500msASL-CBFa - 2500msASL-CBFu)/2500msASL-CBFa≥10%