2321
Cerebral blood flow from arterial spin labeling may serve as a marker for clinical outcome following large vessel occlusion and thrombectomy1Department of Diagnostic and Interventional Radiology, University Hospital Ulm, Ulm, Germany, 2Department of Diagnostic and Interventional Neuroradiology, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany, 3Department of Neurology, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany
Synopsis
Keywords: Stroke, Brain
Motivation: Determination of a non-invasive imaging biomarker for outcome following ischemic stroke.
Goal(s): To investigate whether cerebral blood flow from arterial spin labeling can be used as an imaging biomarker for assessment of clinical outcome following stroke with mechanical thrombectomy.
Approach: Prospective study with pseudo-continuous arterial spin labeling acquired few days after mechanical thrombectomy, combined with outcome evaluation few days and 3-months post-stroke.
Results: Percent cerebral blood flow difference (i.e., between infarct masks in relation to the mirrored mask in the unaffected hemisphere), pre-stroke modified Rankin Scale, and infarct volume were associated with functional independence (i.e., modified Rankin Scale 0-2 at 3-months post-stroke).
Impact: Percent cerebral blood flow difference from the infarct territory may predict functional independence in patients with ischemic stroke and mechanical thrombectomy. Thus, this quantitative parameter may be used as an early non-invasive imaging biomarker to predict clinical outcome.
Introduction
Ischemic stroke is a leading cause of morbidity and mortality worldwide1,2. Large vessel occlusion (LVO) affecting major intracranial vessels can lead to drastic impairment of cerebral blood flow (CBF) in the distally located brain parenchyma, relating to the immanent risk of tissue infarct and long-term sequelae1,2. To avoid long-term functional impairment, LVO can be treated with mechanical thrombectomy (MT), which has revolutionized stroke care following several landmark clinical trials over the last decade3-5. Restored brain perfusion following clot retrieval can be non-invasively measured by arterial spin labeling (ASL), an MRI technique enabling the assessment of CBF6. While ASL-derived CBF has been shown to be sensitive to detect brain perfusion changes following ischemic stroke and MT6-8, whether post-stroke infarct perfusion is linked to the risk of hemorrhagic transformation (HT) and/or better clinical outcome remains a matter of debate. Against this background, we aimed to evaluate ASL-based CBF measurements in the infarct core as a prognostic imaging biomarker, and to investigate the relevance of infarct territory hyperperfusion for development of HT.Methods
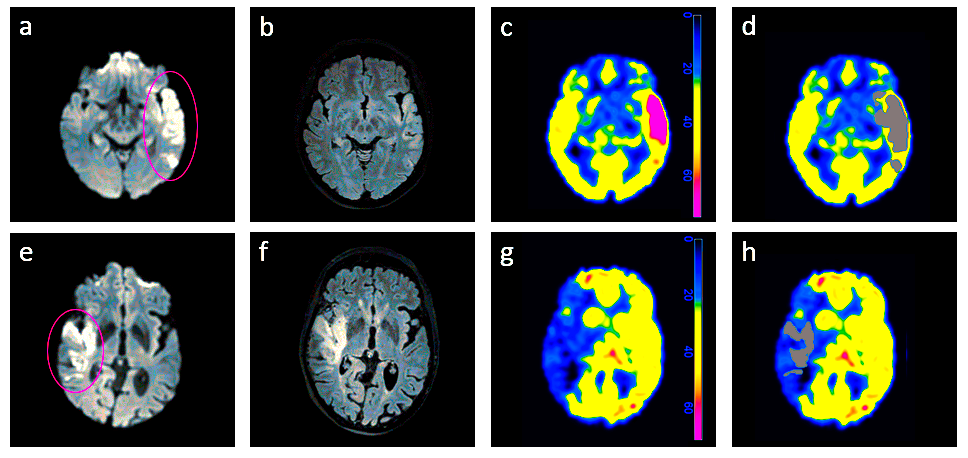
In this prospective monocentric study, we included demographic, clinical, and imaging data from 111 patients (50 men, median age: 74 years), who had undergone MT for ischemic stroke due to LVO of the anterior circulation. Whole-brain pseudo-continuous ASL (pCASL) was acquired at 3-Tesla (32-channel head coil) at median 4 days after MT (i.e., scanned during the acute in-hospital setting prior to discharge) with the following pulse sequence parameters (in line with previous recommendations9,10): 2D echo planar imaging (EPI) readout, label duration=1,800 ms, post-label delay=2,000 ms, repetition time=4478 ms, echo time=11 ms, flip angle=90°, SENSE factor=2, EPI factor=25, scan duration=5:31 min. Additional proton density-weighted M0 data were acquired for CBF quantification. Furthermore, we acquired 3D fluid-attenuated inversion recovery (FLAIR), diffusion-weighted imaging (DWI), 3D non-contrast-enhanced T1-weighted (T1w) images for segmentation and co-registration purposes, and susceptibility-weighted imaging (SWI) for HT screening. Clinical information was obtained at admission, at discharge, and during a follow-up visit 3 months following stroke and MT. Specifically, National Institutes of Health Stroke Scale (NIHSS) scores were determined at admission, and functional independence was defined as the primary outcome, related to a modified Rankin Scale (mRS) 0 to 2 at 3-months post-stroke.Image processing of T1w and pCASL data used custom-built MATLAB scripts (Matlab 2021b) and Statistical Parametric Mapping (SPM12). Image time series were motion-corrected and CBF (in ml/100g/min) was quantified according to previous recommendations9,10. Whole-brain CBF maps and DWI data were co-registered to native T1w space. Tissue probability maps were segmented, and gray matter (GM) masks were applied to CBF maps at a threshold of 0.611. Infarct segmentation of DWI-positive ischemic lesions was performed semi-automatically using ITK-Snap (version 3.8.0; Fig.1). The FLAIR images were available to aid in exact infarct border identification (Fig.1). The CBF values were evaluated from the overlay of the infarct and GM masks, followed by mirroring the individual infarct mask across the midline (Fig.1). Voxel counts of the infarct masks were extracted and multiplied by the voxel size to arrive at infarct volumes. Relative CBF difference was calculated patient-wise from the infarct masks in relation to the mirrored mask in the unaffected hemisphere:
%CBF_difference = [(CBFinfarct_mask – CBFmirrored_mask) / (CBFmirrored_mask)] x 100%
Regression analyses were used to associate demographic, clinical, and imaging parameters with functional independence as the primary outcome measure (p<0.05: statistically significant).
Results
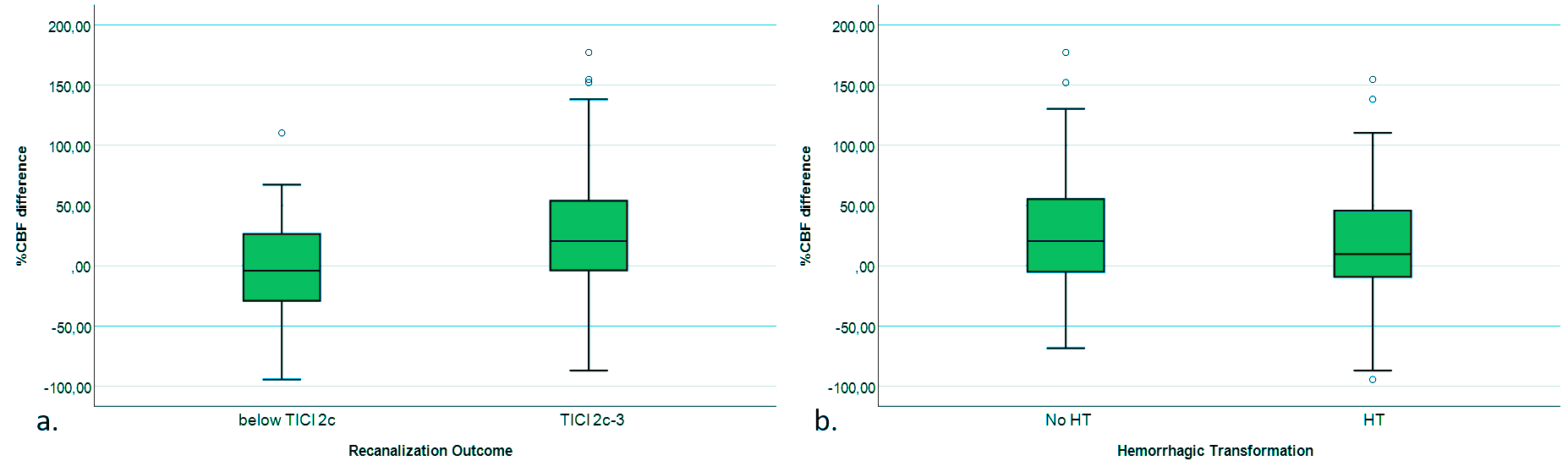
According to univariate analysis, age (odds ratio [OR]=0.97, p=0.03), pre-stroke mRS (OR=0.36, p<0.001), NIHSS at admission (OR=0.93, p=0.04), Alberta Stroke Program Early Computed Tomography Score (ASPECTS) at admission (OR=1.26, p=0.03), complete recanalization (OR=2.95, p=0.03), DWI-positive infarct volume on post-treatment MRI (OR=0.994, p=0.002), and %CBF increase (OR=1.009, p=0.04) were associated with functional independence. According to multivariate regression, %CBF increase (OR=1.01, p=0.02), pre-stroke mRS (OR=0.30, p<0.001), and infarct volume (OR=0.99, p=0.001) were significantly associated with functional independence. Furthermore, post-stroke infarct %CBF increase from the DWI-positive infarct territory was not significantly different between patients with and without HT (p=0.45; Fig.2).Discussion
%CBF may be used as a viable imaging biomarker for clinical outcome, as infarct hyperperfusion is likely a surrogate of micro- and macrovascular infarct hemodynamics. While we used pCASL in this study, multi-delay ASL may become an advanced option in the future to improve CBF estimates as it could account for intra- and inter-subject variations in the arterial transit time.Conclusion
PCASL-derived %CBF difference from the DWI-positive infarct territory may independently predict functional independence at 3-months post-stroke with MT. Furthermore, infarct %CBF increase may not be significantly associated with an increased HT risk.Acknowledgements
No acknowledgement found.References
1. Donkor ES. Stroke in the 21(st) Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res Treat. 2018;2018:3238165.
2. Collaborators GBDS. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. Oct 2021;20(10):795-820.
3. Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. Jun 11 2015;372(24):2285-95.
4. Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. Mar 12 2015;372(11):1009-18.
5. Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. Jan 1 2015;372(1):11-20.
6. Sollmann N, Hoffmann G, Schramm S, et al. Arterial Spin Labeling (ASL) in Neuroradiological Diagnostics - Methodological Overview and Use Cases. Rofo. Jul 19 2023 [Online ahead of print].
7. Potreck A, Mutke MA, Weyland CS, et al. Combined Perfusion and Permeability Imaging Reveals Different Pathophysiologic Tissue Responses After Successful Thrombectomy. Transl Stroke Res. Oct 2021;12(5):799-807.
8. Zaharchuk G. Arterial spin labeling for acute stroke: practical considerations. Transl Stroke Res. Jun 2012;3(2):228-35.
9. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. Jan 2015;73(1):102-16.
10. Lindner T, Bolar DS, Achten E, et al. Current state and guidance on arterial spin labeling perfusion MRI in clinical neuroimaging. Magn Reson Med. 2023 May;89(5):2024-2047.
11. Pinto J, Chappell MA, Okell TW, et al. Calibration of arterial spin labeling data-potential pitfalls in post-processing. Magn Reson Med. Apr 2020;83(4):1222-1234.
Figures