2318
Reproducibility of Whole-Brain Cerebral Blood Flow measurements using phase contrast and arterial spin labeling MRI1Department of Radiology, Stanford University, Stanford, CA, United States, 2Department of Neurosurgery, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Stroke, Neurofluids, Perfusion, Reproducibility
Motivation: We investigated the reproducibility of cerebral blood flow (CBF) measurement techniques with phase contrast (PC) and arterial spin labeling (ASL) MRI given their importance in diagnosing cerebrovascular diseases.
Goal(s): Demonstrate the reproducibility of phase contrast and arterial spin labeling MRI techniques for measuring CBF.
Approach: We used comparative analysis of CBF measurements using phase contrast and arterial spin labeling pre- and post- diamox vasodilation test, measured twice by a week apart.
Results: Strong interclass correlation across modalities and sessions, indicating strong reproducibility for both techniques.
Impact: We conclude that PC- and ASL- MRI measurements are in good agreement and have strong inter-session reproducibility in measuring CBF before and after vasodilation.
Target Audience
Neuro MRI physicists, radiologists, MR vendorsPurpose
Cerebral blood flow (CBF) is an important hemodynamic biomarker in diagnosing cerebrovascular diseases and can be measured using imaging modalities (1). Studies have shown that decreased CBF is linked with neurodegeneration (2) and a higher risk for cerebrovascular diseases (3). Arterial spin labelling and Phase Contrast are two commonly used MR techniques for CBF measurements. While these modalities have been applied in several clinical studies (4, 5), their reproducibility in different physiological conditions remains to be elucidated. Vasodilation is one of the most effective techniques to alter vascular hemodynamics in vivo during an imaging session, and it has been applied to determine the reserve of CBF. In this work, we investigate the reproducibility of CBF measurements in different physiological conditions using ASL and PC MRI.Methods
A total of 35 (mean age 33.9±9.8; F:M, 18:17) normal adults scanned from February 2019 and May 2023 were included in this work. MRI data were acquired in a test-retest experimental design separated by an average 26 days using a 3T MRI (Signa, GE Healthcare, Waukesha, WI) scanner. ASL with the following parameters were acquired: TR=5652 ms, TE=10.7 ms, field-of-view=24 cm, slice thickness=4 mm, number of slices=36, post-label delays: 700, 1250, 1800, 2350, 2900, 3450, and 4000 msec (average scan time 4.30 min) using a Hadamard labeling technique. CBF was calculated from the ASL sequence using a weighted delay approach as described previously(1). A single slice planned between C2 and C3 and cardiac-gated fast low-angle gradient echo sequence with the following parameters were used for PC-MRI: TR/TE = 12/4.6 ms, flip angle = 20 degrees, matrix size = 480 x 384, voxel size = 0.375 x 0.375 mm, slice thickness = 3 mm, number of averages = 2, and velocity encoding = 100 cm/s in the inferior-to-posterior direction. PC-MRI flow data was analyzed using the software on the Arterys (San Francisco, CA) platform, using a region-growing algorithm to define the borders of the arterial lumen of the bilateral internal carotid and vertebral arteries. The blood flow in each vessel was determined by multiplying the flow velocity and area for each vessel, and summing the measurements to yield the total brain blood flow, in units of ml/min. Total brain weight was derived from the volume measured by the T1-weighted anatomical image using the FSL Brain Extraction Toolbox assuming brain tissue density of 1.1 g/ml, which included the ventricular and cerebrospinal fluid spaces. Mean whole brain CBF was calculated from the total blood inflow divided by the total brain weight, yielding the absolute units of ml blood/100 g/min (4). Interclass correlation coefficient (ICC) was used to assess the reliability of CBF measurements across modalities (6). A higher ICC implies a higher reproducibility. Bland-Altman analyses were performed to evaluate the CBF values obtained in the test-retest sessions using both ASL and PC MRI.Results
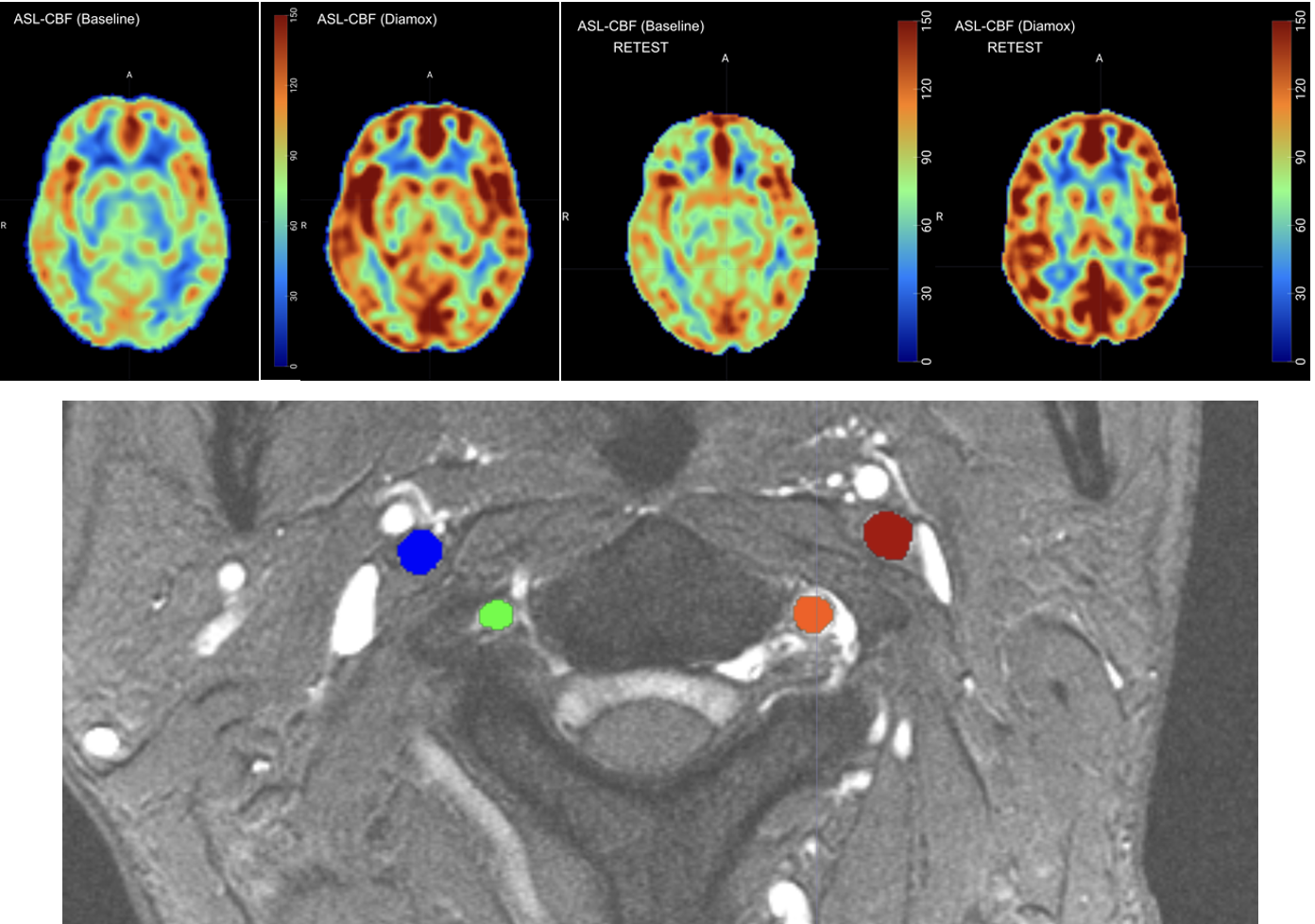
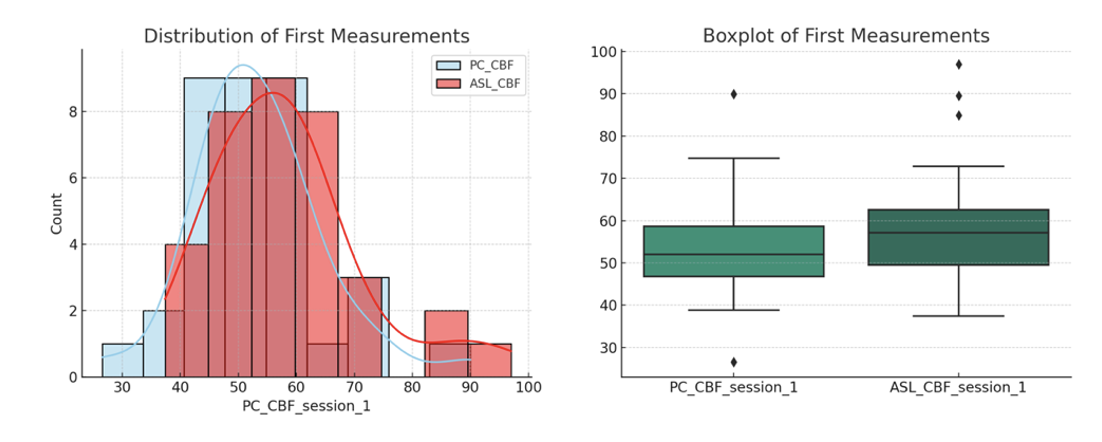
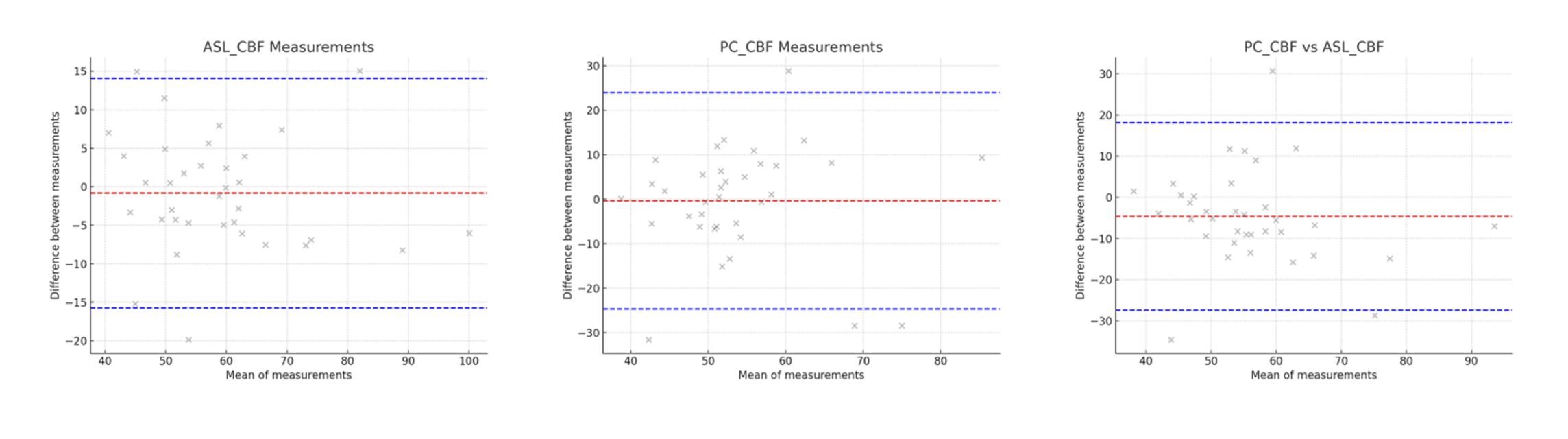
Figure 1 shows ASL and PC MRI maps, showing good visual agreement across test and retest sessions, with both sessions reporting a global increase in CBF after Diamox as expected. Phase contrast image is masked with respect to the vessels segmented for Arterys quantification pipeline. Figure 2 shows Bland-Altman plots with good error bounds and the mean difference bar being nearly zero for all the plots provided.Figure 3 shows the distribution of CBF measurments on patient-by-patient basis with histogram and box plots. Before vasodilation, the interclass correlation coefficient (ICC) within sessions were ICC=0.92 and ICC=0.56 with a mean bias of -0.18 and -0.83 ml/100g/min for ASL- and PC- MRI measurements respectively. Agreement of whole-brain CBF across both modalities within the same session were ICC = 0.71 (p-value = 0.0226) with a bias of -4.69 ml/100g/min. After vasodilation with Diamox injection, ICC=0.78 and ICC=0.64 with a mean bias of -0.45 and 3.68 ml/100g/min for ASL- and PC- MRI measurements were reported with ICC = 0.97 (p-value = 0.0029) and a bias of 10.54 ml/100g/min between modalities.Discussion and Conclusion
In this work, we evaluated the reproducibility of whole brain CBF in normal subjects measured by ASL and PC MRI. Reproducibility before and after vasodilation for both imaging methods are comparable, revealing a slight bias below the zero threshold on the bland-altman analysis. In the context of clinical applications in assessing CBF, ASL and PC are both excellent methods with high reproducibility. ASL offers a more simplistic pipeline for regional cerebral blood flow mapping whereas PC-MRI offers a global perfusion measure and can be used as a proxy.Acknowledgements
No acknowledgement found.References
1. Zhao MY, Tong E, Duarte Armindo R, et al.: Short- and Long-Term MRI Assessed Hemodynamic Changes in Pediatric Moyamoya Patients After Revascularization. Journal of Magnetic Resonance Imaging 2023; n/a(n/a).
2. Korte N, Nortley R, Attwell D: Cerebral blood flow decrease as an early pathological mechanism in Alzheimer’s disease. Acta Neuropathol 2020; 140:793–810.
3. Antonucci MU, Burns TC, Pulling TM, et al.: Acute Preoperative Infarcts and Poor Cerebrovascular Reserve Are Independent Risk Factors for Severe Ischemic Complications following Direct Extracranial-Intracranial Bypass for Moyamoya Disease. AJNR Am J Neuroradiol 2016; 37:228–235.
4. Ishii Y, Thamm T, Guo J, et al.: Simultaneous phase-contrast MRI and PET for noninvasive quantification of cerebral blood flow and reactivity in healthy subjects and patients with cerebrovascular disease. J Magn Reson Imaging 2020; 51:183–194.
5. Fan AP, Jahanian H, Holdsworth SJ, Zaharchuk G: Comparison of cerebral blood flow measurement with [15O]-water positron emission tomography and arterial spin labeling magnetic resonance imaging: A systematic review. J Cereb Blood Flow Metab 2016; 36:842–861.
6. Koo TK, Li MY: A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. Journal of Chiropractic Medicine 2016; 15:155–163.
Figures