2315
Neurovascular characterization of early brain injury in subarachnoid hemorrhage with Multi-modality MRI (1H and 23Na)1Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, United States, 2Neurovascular Research Unit, Department of Radiology, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, United States, 3Department of Neurology, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, United States
Synopsis
Keywords: Stroke, Traumatic brain injury
Motivation: This work is to identify d 23Na (sodium) as a biomarker for early brain injuries (EBI) after subarachnoid hemorrhage (SAH).
Goal(s): This research utilizes a novel head-implanted coil to measure 1H and 23Na whole-brain MRI for characterization of EBI.
Approach: We achieved acquisition of 1H for anatomical templates and 23Na MRI images at an impressive spatial resolution of 300x300x500 µm.
Results: We surprisingly observed that the 23Na signal precedes the appearance of conventional 1H diffusion-weighted signal after SAH-related brain injury. Also, a concentration gradient distribution of 23Na mapping within the EBI regions demonstrated a finer granularity not typically depicted by conventional 1H MRI.
Impact: This work revealed the distinct 23Na dynamics for EBI detection and highlighted the critical usage of a multi-modal platform to specify the EBI after SAH.
INTRODUCTION
Subarachnoid hemorrhage (SAH) accounts for 5-10% of cerebrovascular accidents, with a mortality rate of 40 and 50% for hospitalized patients. Early brain injury (EBI) phase after SAH (the first 72h) is a significant cause of morbidity and mortality in SAH patients. Conventional SAH/stroke detection relies on proton-based (1H) MRI techniques, whereas functional MRI (fMRI) brain mapping indirectly measures neuronal activity through the neurovascular coupling mechanism. Because sodium (23Na) is the primary ion in triggering neuronal action potentials, non-invasive 23Na mapping is a promising diagnostic tool for studying neuronal activities in diseases such as SAH and stroke. Here, we introduced a multimodal MRI platform MRI (1H and 23Na) to improve the sensitivity and specificity of 23Na signaling in probing neurovascular mechanisms of EBI after SAH.METHODS
Animal Model:C57BL/6 mice (Charles River Laboratories, MA) were anesthetized with isoflurane 2.5% for induction and 1%–1.25% for maintenance (70% N2/30% O2). Blood pressure was continuously monitored via a femoral artery catheter (PowerLab; AD Instruments, MO). The mice were performed with filament middle cerebral artery occlusion (MCAO) for ischemia stroke or filament perforation SAH induction models. General surgical preparation was performed as described previously1,2.
MR Techniques:
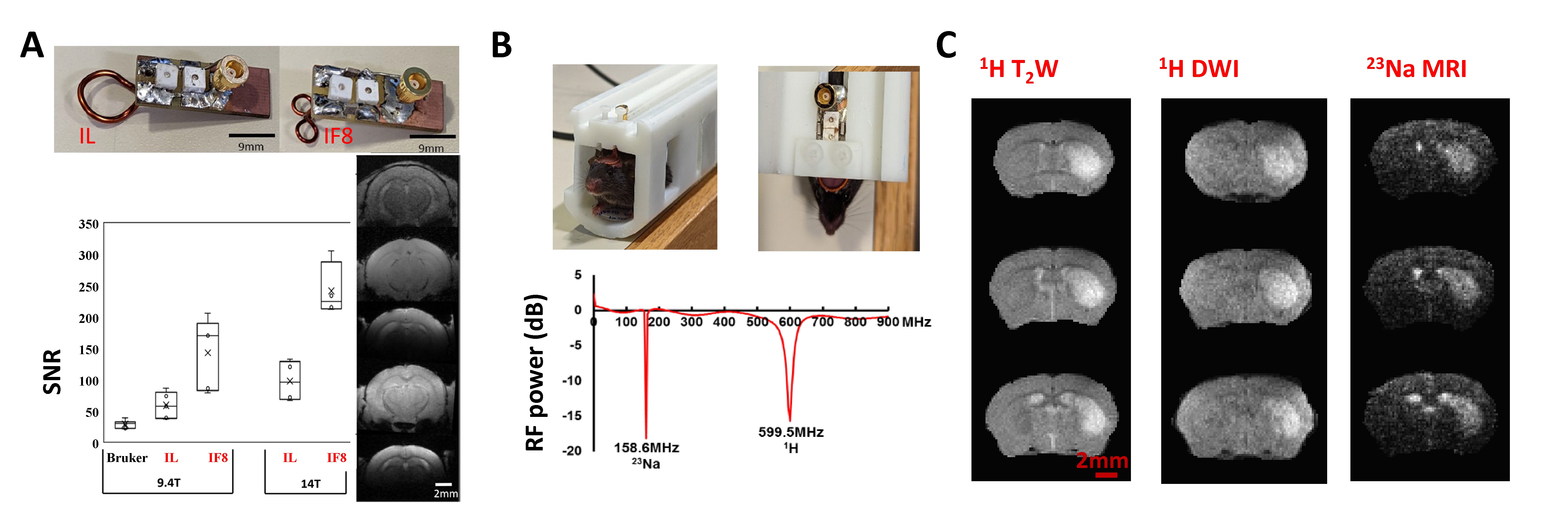
All images were acquired with a 14 T/13 mm horizontal bore magnet (Magnex), interfaced to a Bruker AV-Neo console (Bruker), and equipped with a 6 cm gradient set, capable of providing 1.2 T/m (Resonance Research). A tunned transceiver surface implantable coil was used to acquire fMRI images. The T2W anatomical, DWI, and 23Na MRI scans were acquired with the same FOV(14.4X9.6X8 mm3), with a matrix of 96X48X16, 48X32X16, and 48X32X16, respectively. For DWI, b values of 50, 100, 150, 250, 400, and 600 s/mm2 were applied.
RESULTS
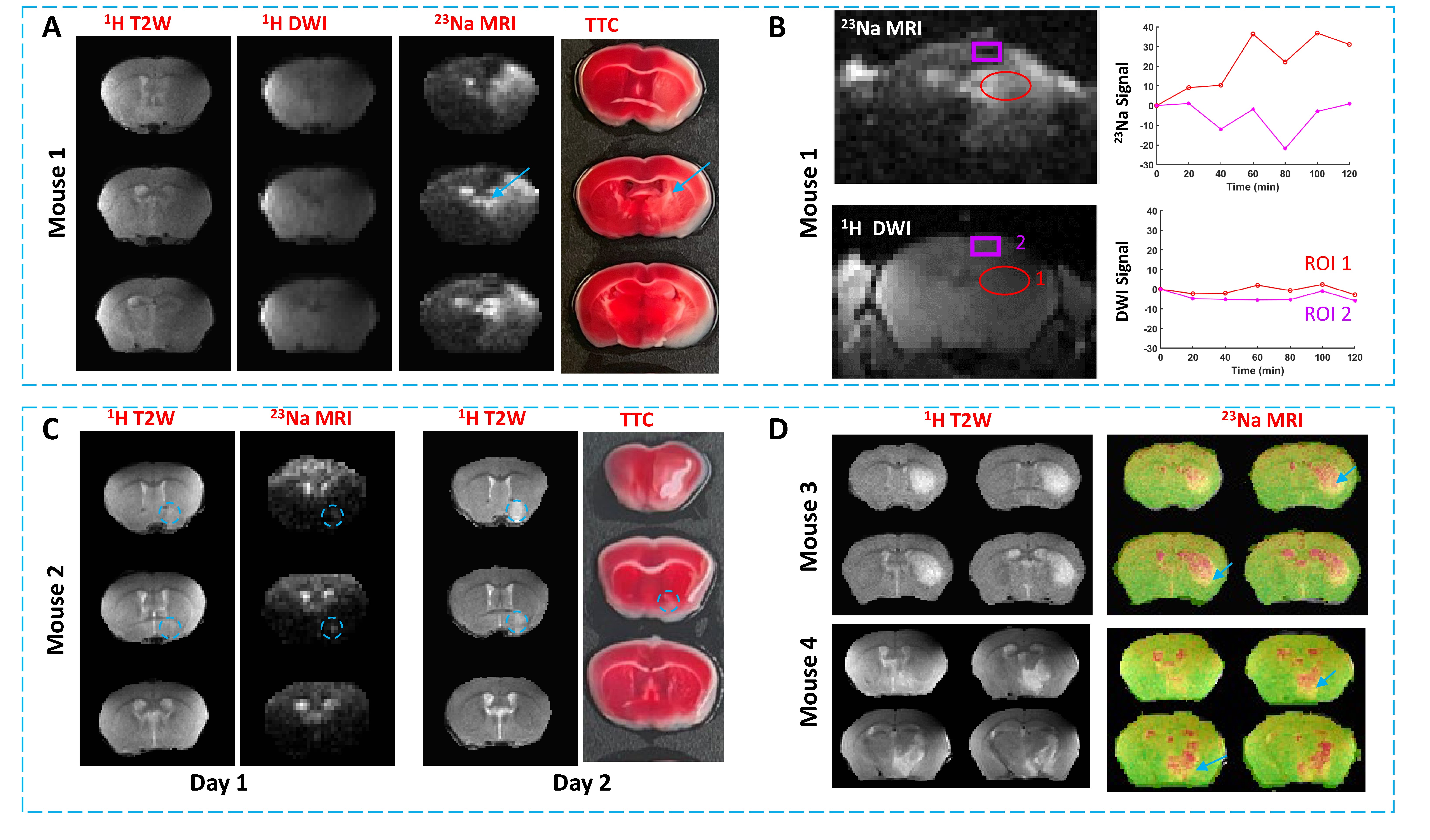
We have established a high-resolution 23Na MRI platform based on our high-field 14T preclinical scanner. The SNR head-implanted RF coil (<2.5g) is ~ 8 times higher with our 14T scanner than the conventional Bruker 4 array coil when imaging mouse brains with 9.4T (Fig 1A). A dual-tuned was implanted for the acquisition of 1H T2-weighted (T2W) anatomical and diffusion-weighted imaging (DWI) maps and 23Na MRI from the same animal in our 14T scanner (Fig 1B). This implantable double-tuned 1H/23Na RF coil can improve the SNR with an impressive 300 µm in-plane brain-wide 23Na-based MRI readout for MCAO ischemic stroke (Fig 1C), demonstrating a superior SNR and spatial resolution compared to prior high-field MRI studies.We obtained pilot 23Na MRI data to track alterations in 23Na signals following acute SAH (filament perforation model) in 4 mice. In mouse 1, we observed that the 23Na signal appears as early as 45 minutes following SAH induction and before the appearance of the T2W and DWI signal (Fig 2A). Moreover, our pilot data showed unique 23Na temporal dynamics between the core and the surrounding injury regions, particularly during the first 4 hours of SAH induction (Fig 2B). In mouse 2, the hyperintensity only appeared on 23Na MRI with a minor brain injury following the first day of SAH, while it began to appear in T2W MRI on the second day (Fig 2C). Our pilot study also revealed a heterogeneous distribution of 23Na MRI signal within the EBI region delineated by conventional T2W/DWI-based MRI (Fig 2D). This observation indicates the presence of a 23Na concentration gradient within the EBI regions. This heterogeneous distribution of 23Na signal mapping within the EBI regions may exhibit a finer granularity than what is typically depicted by conventional 1H MRI based on T2W and DWI approaches.
CONCLUSIONS
We optimized the implanted double-tuned 1H/23Na RF coils for high-resolution 23Na-based and T2-weighted 1H MRI readout of early brain injuries after SAH. We observed distinct temporal and spatial features of 23Na dynamics after SAH induction. This work implies that 23Na MRI may offer a more precise approach to identifying EBI after SAH.Acknowledgements
This research was funded by NIH funding (RF1NS113278, RF1NS124778, R01NS122904, R01NS120594), NSF grant 2123971, and the S10 instrument grant (S10 MH124733–01) to Dr. Yu in Martino’s Center. Funding was received by the National Institute of Neurological Disorders and Stroke at the National Institutes of Health R01NS102969 to Dr. Ayata; R25NS065743, KL2TR002542, and K08NS11260 to Dr. Chung, Ellison Foundation for Dr. Ayata, Andrew David Heitman Foundation for Drs Ayata, Chung, and Jiang, American Heart Association and American Stroke Association(18POST34030369), Aneurysm and AVM Foundation Brain Aneurysm Foundation to Dr. Chung.References
1 Fischer, P. et al. Rapid hematoma growth triggers spreading depolarizations in experimental intracortical hemorrhage. Journal of Cerebral Blood Flow & Metabolism 41, 1264-1276 (2021).
2 Lai, J. H., Qin, T., Sakadžić, S., Ayata, C. & Chung, D. Y. Cortical Spreading Depolarizations in a Mouse Model of Subarachnoid Hemorrhage. Neurocritical Care 37, 123-132 (2022). https://doi.org:10.1007/s12028-021-01397-9
Figures