2313
High-resolution 3D Multislab DWI for the Diagnosis of Acute Stroke1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Department of Radiology, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, China, 3MR R&D, Philips Healthcare, Suzhou, China
Synopsis
Keywords: Stroke, Diffusion/other diffusion imaging techniques
Motivation: Conventional low-resolution 2D DWI has limited diagnosis accuracy in stroke patients.
Goal(s): Our goal was to apply high-resolution 3D DWI in stroke patients and assess its diagnostic capabilities compared to low-resolution 2D DWI.
Approach: We employed simultaneous multislab imaging for 3D diffusion signal sampling, utilizing opposite phase encoding polarity for distortion correction and CPEN for boundary artifact correction. We conducted examinations on 15 acute stroke patients.
Results: The utilization of high-resolution 3D DWI with isotropic resolution significantly enhances image quality in terms of clarity, distortion levels, and clinical value, surpassing traditional 2D DWI.
Impact: High-resolution isotropic 3D DWI, using simultaneous multislab acquisitions, may help in the identification of small brain lesions that may be challenging to detect using low-resolution 2D DWI.
Introduction
This study employs the previously developed high-resolution 3D DWI technique (multi-band-accelerated multi-slab imaging)[1-3] to detect small lesions in ischemic stroke. Previous studies have utilized conventional 2D DWI to achieve thin-layer imaging with layer thicknesses ranging from 1.5 to 3.5 mm[4-8]. However, 2D EPI DWI has lower SNR efficiency than the 3D DWI technique[1]. This study will use this 3D DWI protocol to at least enhance the DWI resolution of clinical acute ischemic stroke examinations to 1.5 mm isotropic and compare it with the 2D DWI sequence to investigate whether the high-resolution 3D DWI technology helps improve diagnosis accuracy of acute ischemic stroke lesions.Method
This experiment only included patients with minor symptoms and stable conditions. The inclusion criteria did not strictly require the subtype of ischemic stroke or whether it was the first onset.The specific inclusion criteria were: (1) clinical symptoms suggestive of ischemic stroke or transient ischemic attack with an NIHSS score (National Institutes of Health Stroke Scale) between 1-4 points, indicating a minor stroke; (2) within 72 hours of the onset; (3) exclusion of cerebral hemorrhage by CT; (4) ≥18 years of age; (5) no contraindications to MRI and in a sufficiently stable state to undergo MRI scanning. The exclusion criteria were: (1) image quality not meeting the requirements; (2) patients experiencing discomfort or other reasons unable to complete the scan. A total of 15 patients were scanned in the experiment. All experiments were approved by the institutional review board, and patients had signed informed consent before the experiment.
The experiments were conducted on a 3.0 T scanner (Ingenia CX, Philips Healthcare, Best, The Netherlands) with a 32-channel head coil. The MRI scans included DWI, T2W, T1W FLAIR, T2W FLAIR, and SWI, With the parameters shown in Table 1. Except for the 3D blipped-SMSlab, all other sequences were part of the routine scanning protocol used for stroke patients.
The reconstruction of blipped-SMSlab used the methods described in the previous work[2, 3]. Additionally, it uses positive and negative ky encoding to correct for EPI distortions. Then, the CPEN algorithm[9] is used to correct boundary artifacts.
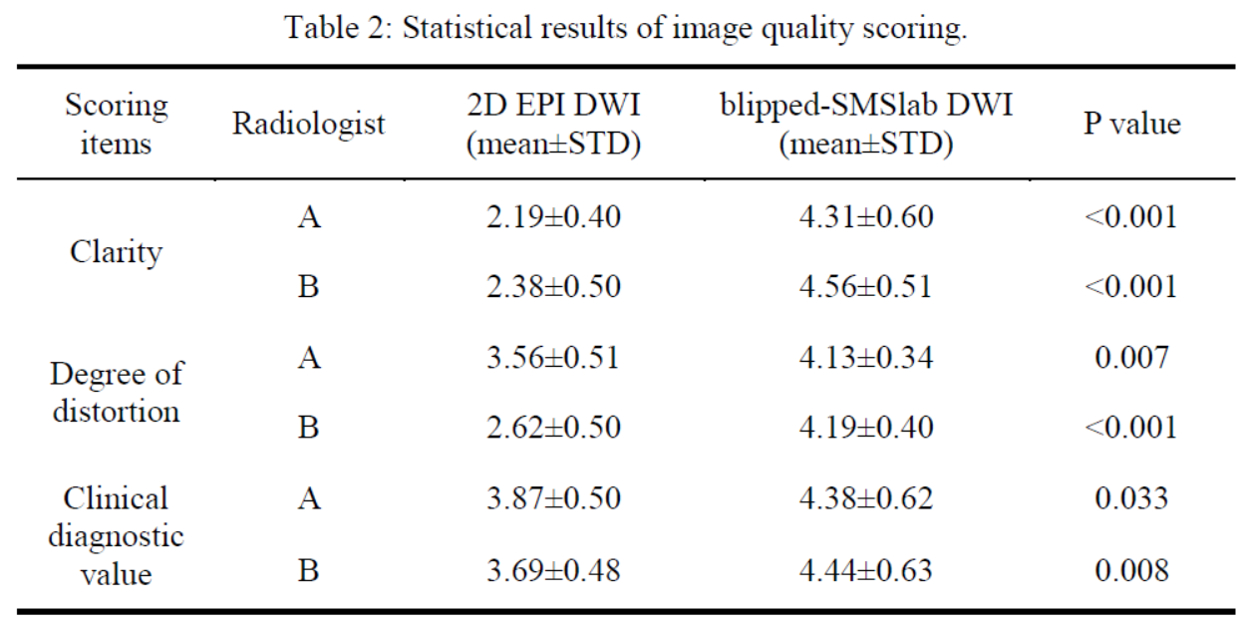
Then, diffusion images from the 15 patients were randomly arranged and scored by two radiologists who were blinded to the patient information and sequence information. The scoring (from 1 to 5) included: (1) Clarity: 1 for very unclear, unable to meet the needs of identifying lesions; 5 for very clear, able to identify more structural details or lesions. (2) Degree of distortion: 1 for very severe distortion, significantly interfering with diagnosis; 5 for no visible distortion. (3) Clinical diagnostic value: 1 for almost no value, unable to meet clinical needs; 3 for meeting basic clinical needs; 5 for very high value, able to provide more information than the regular clinical sequences.
After scoring, the scores for each item were compared between 2D EPI DWI and blipped-SMSlab DWI. The Wilcoxon signed-rank test was used to analyze whether there was a statistical difference of the scores, with the threshold set at P<0.05. Finally, the intraclass correlation coefficient (ICC) was used to assess the consistency and reliability between the scoring results of the two radiologists. An ICC value greater than 0.75 is generally considered to represent good consistency.
Results
Only 2 patients showed acute infarct lesions in the mean diffusion images, which are shown in Figures 1 and 2.The scoring results from the two diffusion sequences are shown in Table 2. The blipped-SMSlab DWI had higher image clarity, less image distortion, and higher clinical diagnostic value compared to the 2D EPI DWI. Furthermore, the consistency analysis showed that the scoring results of the two radiologists were consistent across the three items, with ICC values greater than 0.75, indicating reliable results.
Discussion and conclusion
The study conducted a preliminary comparison between traditional 2D EPI DWI and high-resolution 3D DWI. High-resolution DWI based on blipped-SMSlab acquisition may help in identifying small acute infarcts that are not easily detected on low-resolution DWI. Future research could include more patients to improve the reliability of the conclusions. Also, how to optimize the balance between examination efficiency and resolution without increasing patient risk can be another research topic.This study was the first to apply blipped-SMSlab with a resolution of 1.5 mm isotropic to the clinical examination of ischemic stroke. According to the radiologists' evaluations, compared to traditional DWI, this method significantly improves image quality and may increase the detection rate of ischemic lesions.
Acknowledgements
No acknowledgement found.References
1. Liu, S., et al., Magn Reson Med, 2023. 90(3): p. 978-994.
2. Zhang, J., et al., in ISMRM. 2022. p. 4694.
3. Zhang, J., S. Liu, and H. Guo, in ISMRM. 2022. p. 2023.
4. Hafermehl, K.T., in Centre for Neuroscience. 2016, University of Alberta.
5. Albach, F.N., et al., Stroke, 2013. 44(4): p. 1043-1048.
6. Choi, B.S., et al., Am J Neuroradiol, 2012. 33(9): p. 1771.
7. Benameur, K., et al., AJNR Am J Neuroradiol, 2006. 27(9): p. 1987-1989.
8. Entwisle, T., Y. Perchyonok, and G. Fitt, J Med Imag Radiat On, 2016. 60(5): p. 616-623.
9. Zhang, J., et al., Magn Reson Med, 2022. 87(3): p. 1546-1560.
Figures
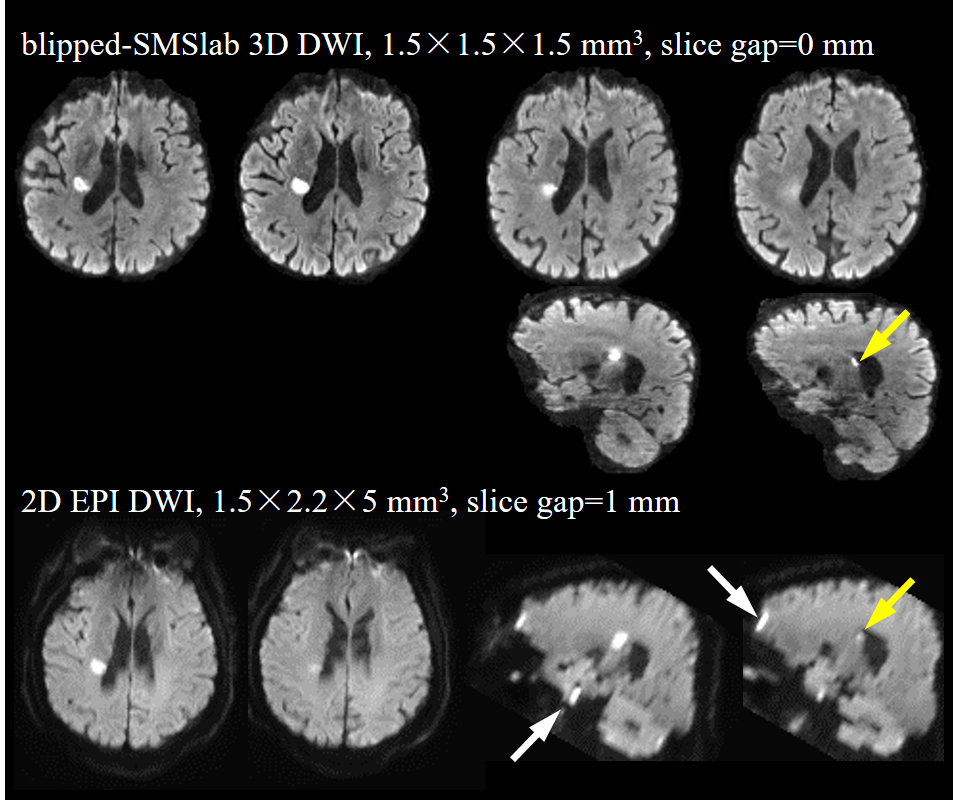
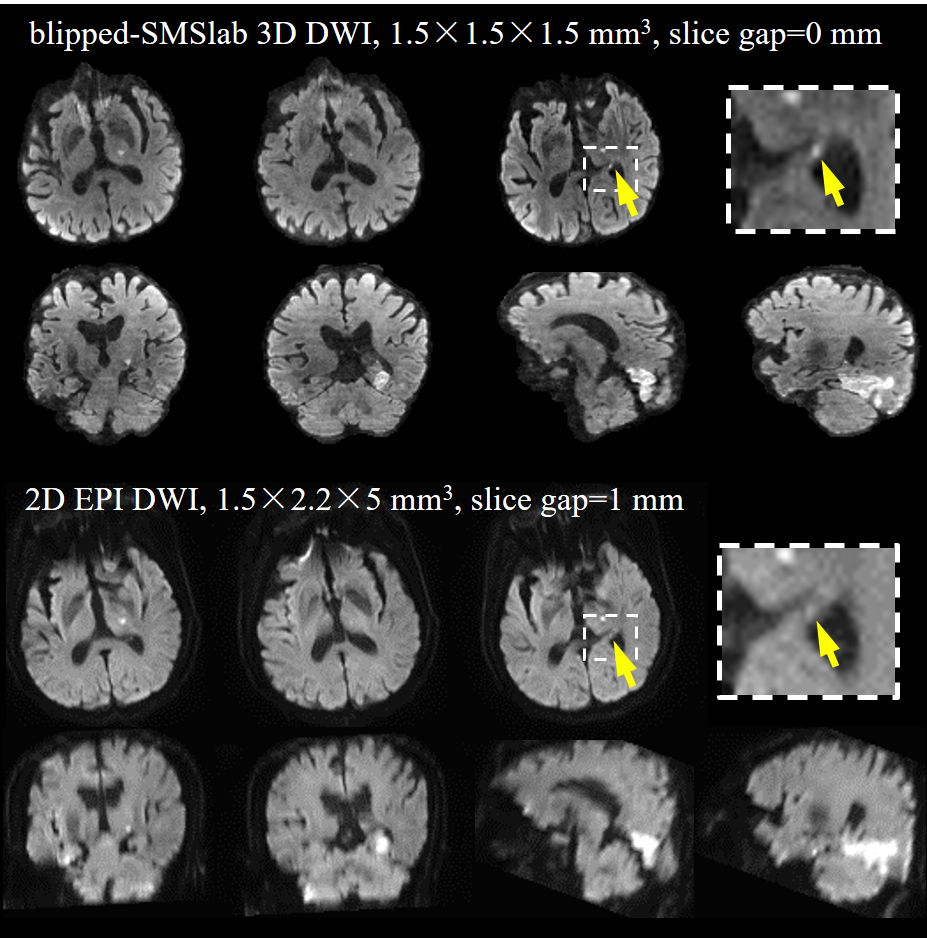
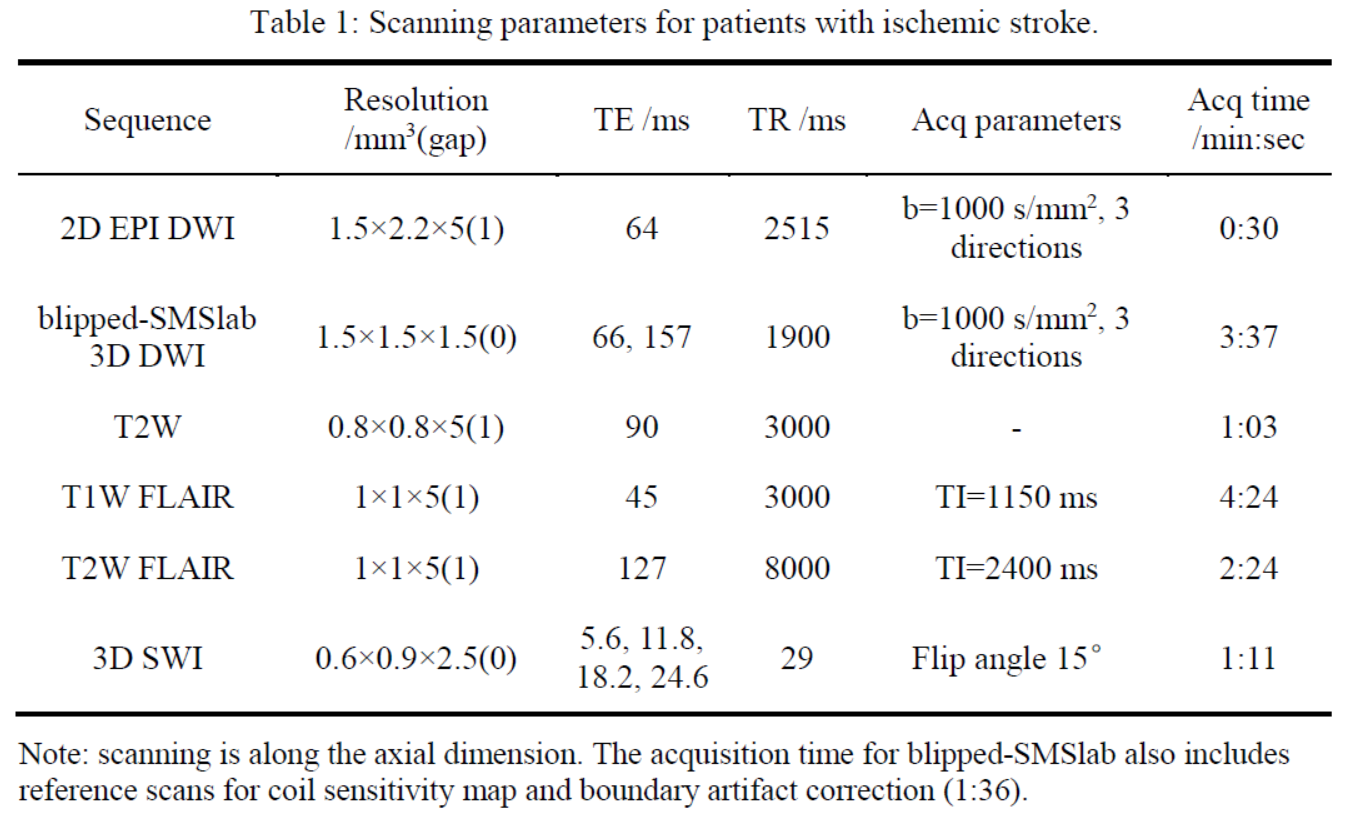
Table 1: Scanning parameters for patients with ischemic stroke. Note: scanning is along the axial dimension. The acquisition time for blipped-SMSlab also includes reference scans for coil sensitivity map and boundary artifact correction (1:36).