2309
fMRI & DTI to Study Neural Correlates in Controlled Brain Stimulation for Post Stroke Rehabilitation1Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India, 2Department of Psychiatry, All India Institute of Medical Sciences, New Delhi, India, 3Department of NMR, All India Institute of Medical Sciences, New Delhi, India, 4Department of Neurology, All India Institute of Medical Sciences, New Delhi, India
Synopsis
Keywords: Stroke, Stroke, Rehabilitation, DTI
Motivation: To study the impact of closed-loop brain stimulation in neuroplasticity in stroke rehabilitation.
Goal(s): In this study we investigate with fMRI and diffusion tensor MR imaging the neural correlates with closed loop brain stimulation in stroke.
Approach: fMRI and DTI for six subjects was taken in a pilot case-control study.
Results: fMRI and DTI both showed higher cortical activity and increase in FA values for ipsilesional CST in cohort of patients with TMS-robotic intervention than the control group.
Impact: A brain stimulation system integrated with an exoskeleton, providing a real-time bidirectional feedback mechanism for patients, has been shown to actively involve patients in their rehabilitation journey.
Introduction
The presence of numerous sensorimotor impairments following a stroke significantly constrains a patient's functional capacity. Repetitive Transcranial Magnetic Stimulation (rTMS) involving predefined passive stimulation at both low and high frequencies has displayed evidence of improved motor recovery in stroke rehabilitation. Nevertheless, this approach lacks patient engagement, feedback, and the ability to personalize treatment according to the patient's clinical needs (1). Recent developments in bio-signal-guided brain stimulation have shown promising potential for strengthening synaptic connections through a closed-loop method in cellular studies, non-primate models, and healthy subjects (2). While rare, seminal studies have indicated the feasibility of Activity-Dependent single-pulse TMS, where motor activity in the affected hand triggers TMS directed at the lesioned motor cortex (3)(4). In this study we investigate with fMRI and diffusion tensor MR imaging the neural correlates with closed loop brain stimulation in stroke.Methods
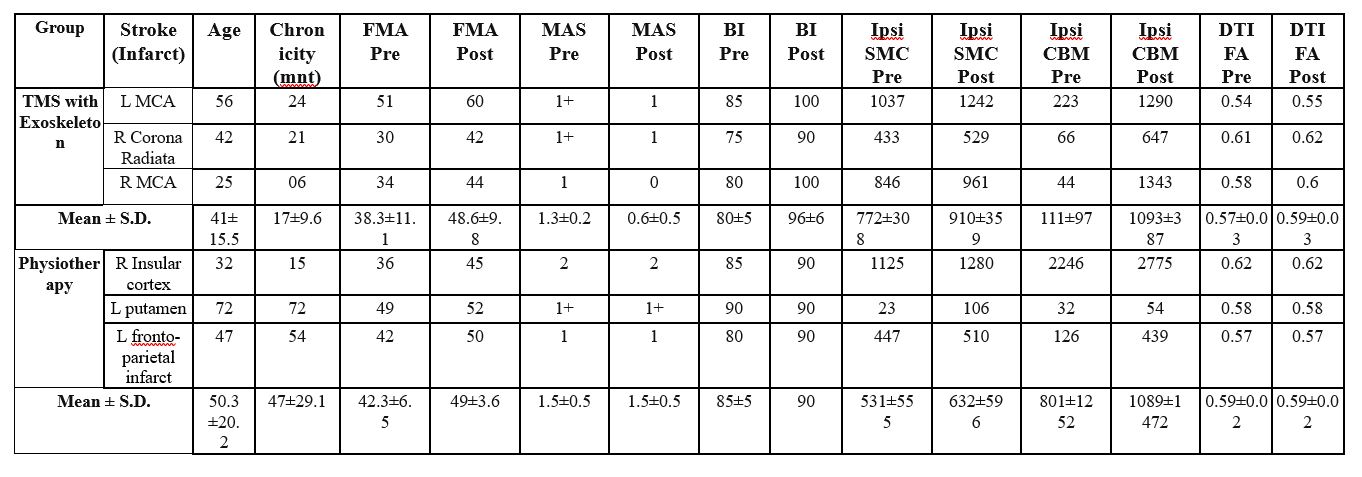
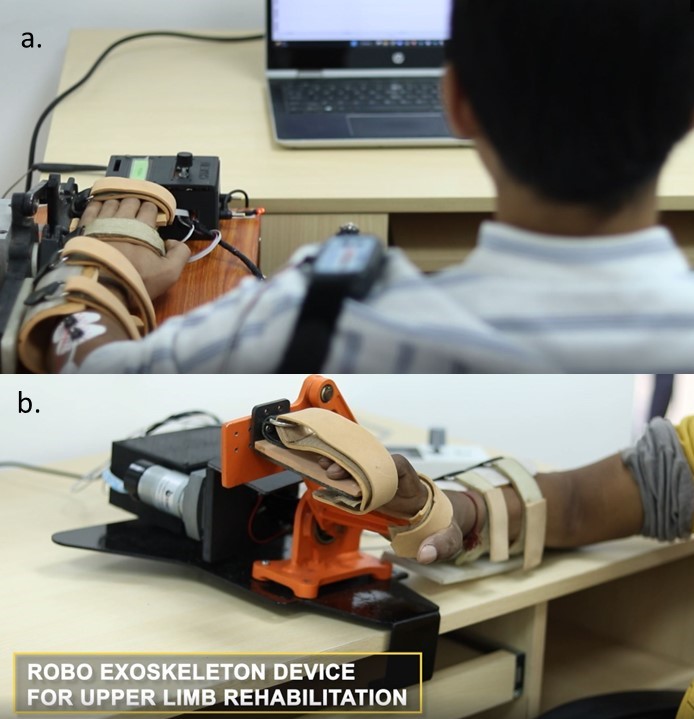
A patient centric brain stimulation platform was developed to study the neural reorganizations in response to brain stimulation while patient is engaged voluntarily in the therapy. Patient’s Electromyogram (EMG) from affected-hand by controlled TMS (to lesioned M1) and simultaneously using an Exoskeleton device (5) ensuring completion of the movement attempted. The real-time performance biofeedback of EMG ensures patient’s engagement. Six (n=6) right-handed, hemiparetic patients with 3–120 months’ chronicity ware recruited in two groups- 1) TMS Exoskeleton group and 2) Physiotherapy group; EMG controlled TMS with exoskeleton session (5) was given to three patients in group 1 for 45 minutes/day for 20 sessions and same amount of physiotherapy was given to another three patients in group 2 (Figure 1). Clinical-assessment using Modified Ashworth Scale (MAS), Fugl-Meyer Assessment (FMA) Scale, Barthel-Index (BI), neuroimaging (fMRI) and structural T1 and Diffusion Tensor Imaging (DTI) was acquired both pre- & post-intervention. For fMRI, Block-design paradigm of 40s alternate baseline and activation-task were used. Patients performed self-paced wrist-extension repeatedly in full Range-of-Motion with affected-hand. Presentation on MR compatible 20” LCD monitor (Esys in vivo eprime 1.1) with projection on mirror attached to head coil where image-of-hand notifies the active-block and cross on image-of-hand represents the rest-block. fMRI-data were acquired as 31 slices, TR = 2000ms, TE = 30 ms, FOV = 230x230x155mm, Flip angle: 90°, voxel-size:1.8×1.8×5 mm. Data-analysis (using SPM12) included realignment by aligning images to mean-image, co-registration using T1-image, normalized, and smoothing with 8×8×8 Full Width at Half-Maximum (FWHM) filter on pre-& post-BOLD images. DTI data were acquired pre-and post-therapy using the same scanner with TR/TE: 4820/92 ms, Flip-angle: 90 degrees, FOV: 230×230×148 mm, voxel size: 2×2×2 mm, slice thickness: 2mm, 32 volumes with b=800 s/mm2 and one volume with b=0 s/mm2. FA values were calculated for DTI data (using FSL) for corticospinal tract of the ipsilesional hemisphere.Results
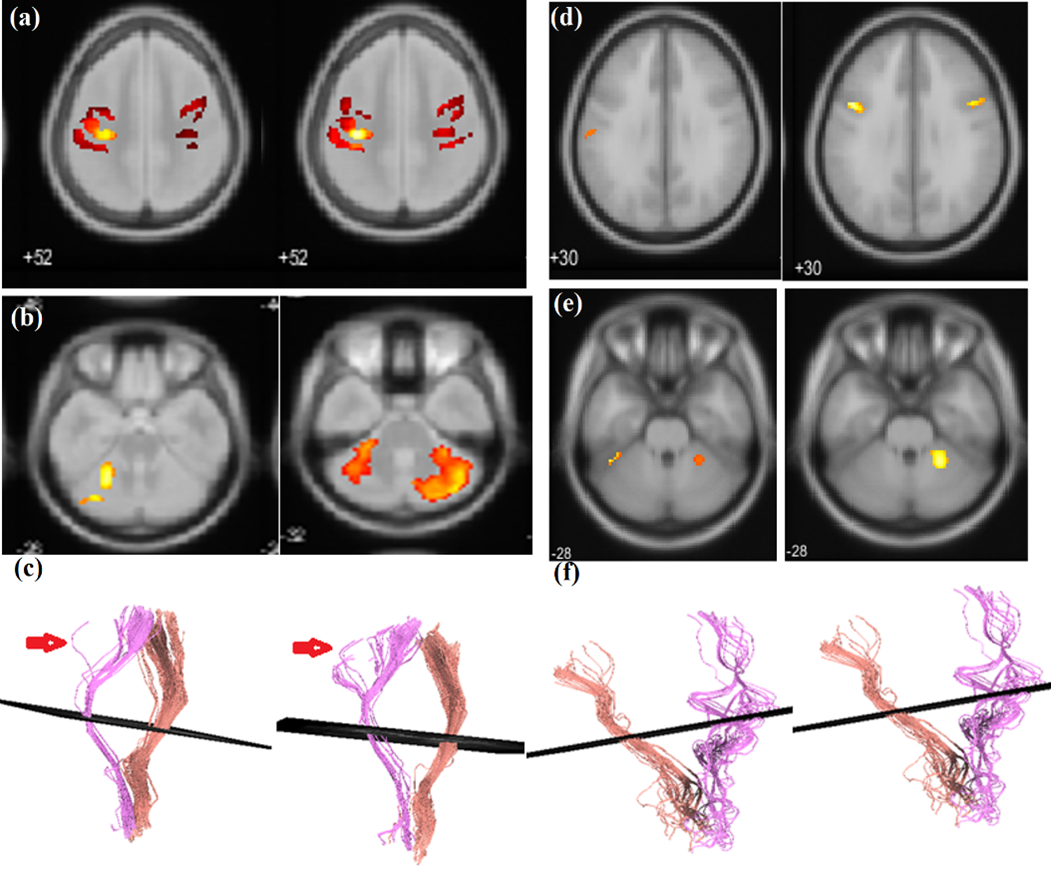
Figure 2 showing the exoskeleton device integrated with TMS system. Cortical remapping was observed in terms of neural activation evidenced in functional MRI before and after 20 sessions. All six patients showed improvement in the clinical-scales. Pre- to post-20 sessions (Figure 1), TMS exoskeleton patients’ in group were observed to have reduced spasticity at wrist (MAS from 1.3±0.2 to 0.6±0.5) compared to physiotherapy group (MAS from 1.5±0.5 to 1.5±0.5), increase independence in ADL as demonstrated by increased Barthel-Index (from 80±5 to 96±6) compared to physiotherapy group (from 85±5 to 90). Sensorimotor-control improvement as indexed by FM, was observed in both groups, (from 38.3±11.1 to 48.6±9.8) in TMS-Exoskeleton group compared to physiotherapy group (from 42.3±6.5 to 49±3.6). Ipsilesional Sensorimotor Cortex (SMC) BOLD fMRI activity has been observed to be increased in TMS exoskeleton group (from 772±308 to 910±359) as compared to physiotherapy group (531±555 to 632±596) (Figure 3a,d). Ipsilesional Cerebellum activity increased in TMS Exoskeleton group (from 111±97 to 1093±387) as compared to physiotherapy group (from 801±1252 to 1089±1472) (Figure 3b,e). DTI-derived FA-values for ipsilesional CST were found to be increased for TMS exoskeleton group (0.57±0.03 to 0.59±0.03), and the post-therapy tracts were observed to be denser and more intact as compared to pre-therapy, while for the physiotherapy group, the values were observed to show no change (0.59±0.02 to 0.59±0.02) (Figure 3c,f).Conclusion
A transcranial magnetic brain stimulation system has been designed that is integrated with a customized exoskeleton device, providing a real-time bidirectional feedback mechanism for patients in stroke rehabilitation. It has been shown to actively engage patients in their rehabilitation journey. The intervention showed good improvement in cortical representative areas with fMRI and change in DTI showed strengthen CST with only 20 sessions of intervention. The outcomes demonstrate promising findings that warrant additional investigation with a larger group of participants.Acknowledgements
Authors thank the funding support from SERB, ICMR and INAE, Government of India.References
1. Rossini, P. M., Burke, D., Chen, R., Cohen, L. G., Daskalakis, Z., Di Iorio, R., et al. (2015). Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: basic principles and procedures for routine clinical and research application: an updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 126, 1071–1107. doi: 10.1016/j.clinph.2015.02.001 2. Edwardson, M. A., Lucas, T. H., Carey, J. R., and Fetz, E. E. (2013). New modalities of brain stimulation for stroke rehabilitation. Exp. Brain Res. 224, 335–358. doi: 10.1007/s00221-012-3315-1 3. Bütefisch C. M., Khurana V., Kopylev L., Cohen L. G. (2004). Enhancing encoding of a motor memory in the primary motor cortex by cortical stimulation enhancing encoding of a motor memory in the primary motor cortex by cortical stimulation. J. Neurophysiol. 91, 2110–2116. doi: 10.1152/jn.01038.2003 4. Izumi S. I., Kondo T., Shindo K. (2008). Transcranial magnetic stimulation synchronized with maximal movement effort of the hemiplegic hand after stroke: a double-blinded controlled pilot study. J. Rehabil. Med. 40, 49–54. doi: 10.2340/16501977-0133 5. Singh, N.; Saini, M.; Anand, S.; Kumar, N.; Padma Srivastava, M.V.; Mehndiratta, A. (2019) Robotic Exoskeleton for Wrist and Fingers Joint in Post-Stroke Neuro-Rehabilitation for Low-Resource Settings. IEEE Transactions on Neural Systems and Rehabilitation Engineering. 27(12):2369-2377. DOI: 10.1109/TNSRE.2019.2943005.Figures