2308
Investigation of the heterogeneity of post-stroke apathy using resting-state fMRI1Radiology, The First Affiliated Hospital of USTC, Hefei, China, 2GE Healthcare, Shanghai, China
Synopsis
Keywords: Stroke, fMRI (resting state)
Motivation: Post-stroke apathy (PSA) is a highly heterogeneous disorder, which presents obstacles to the effective diagnosis and treatment.
Goal(s): We intended to identify distinct subtypes of PSA and revealed the underlying neurological substrates of PSA heterogeneity.
Approach: By comparison between stroke patients and normal controls, abnormal alterations of resting-state functional connectivity (RSFC) were determined and correlated with apathy syndrome. PSA subtypes were identified based on the significant canonical correlates using hierarchical clustering.
Results: The best clustering scheme was four clusters and we observed significant group differences in graph theoretic metrics.
Impact: Various subtypes displayed distinct characteristics in terms of RSFC and graph theoretic metrics. Our study emphasizes the importance of RSFC of neural network in the evaluation of PSA heterogeneity and provides new insights for future research and therapeutic targets.
Introduction
Post-stroke apathy (PSA) is a highly heterogeneous disorder that affects approximately 30% of stroke survivors [1]. The heterogeneity of PSA presents obstacles to the effective diagnosis and treatment [2]. Using resting-state fMRI, researchers can explore spontaneous fluctuations in neural activities of different brain regions. Recent studies suggested that various patterns of abnormal alterations of neural network in the brain were closely associated with different aspects of apathy syndrome, indicating that functional neural network might explain the variability and complexity of PSA [3]. By applying multivariate analysis and clustering algorithms, it is possible to identify distinct subtypes of PSA. We intended to reveal the underlying neurological substrates of PSA heterogeneity and provide a basis for personalized interventions tailored to specific subtypes.Methods
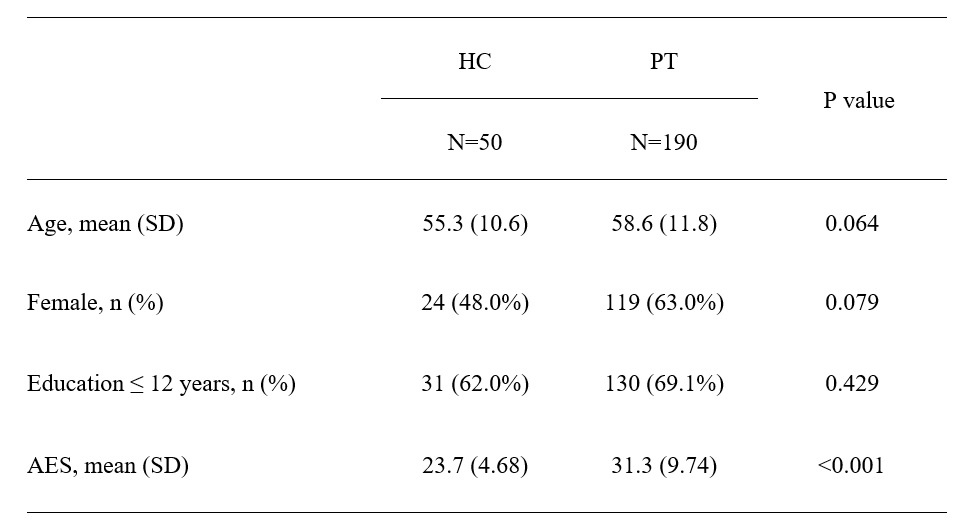
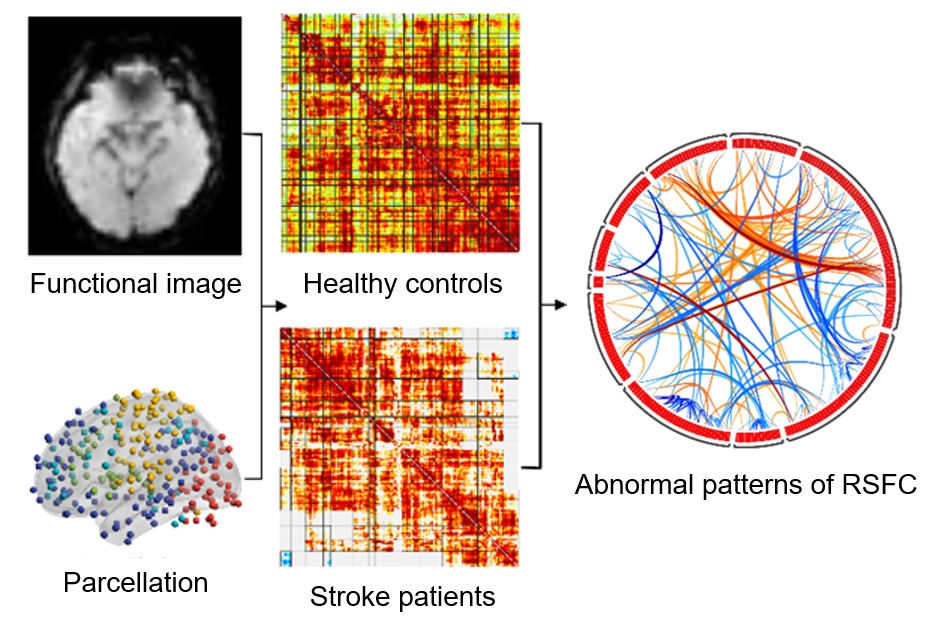
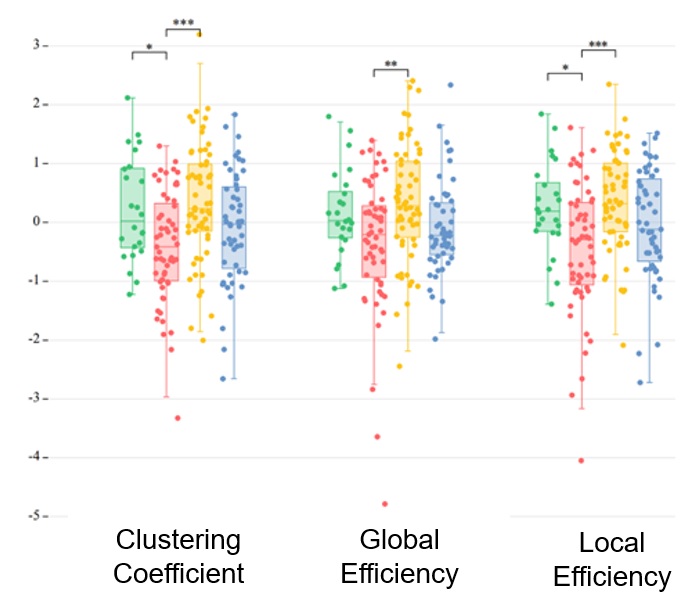
Our Institutional Review Board approved the study and written informed consent was obtained from all the participants. We prospectively recruited 190 acute ischemic stroke patients admitted to our hospital between March 2021 and September 2023. All the patients were diagnosed of first acute ischemic stroke within 2 weeks of onset. In addition, 50 healthy controls with comparable demographics were enrolled for comparison. The clinician version of apathy evaluation scale (AES) was used to assess the degree of apathy. Imaging data were acquired using a 3.0-T scanner (MR750W, GE Healthcare, WI) with a 24-channel head and neck coil. The scan parameters of resting-state fMRI were as follows: FOV = 24 × 24 cm2, matrix size = 64 × 64, TR/TE = 2000/30 ms, slice thickness/gap = 3.5/0 mm, flip angle = 90°, slice number = 36, 240 phases and scan time = 8 minutes. High-resolution 3D T1 and T2 Flair images were also acquired for spatial normalization and manual lesion segmentation. Image preprocessing was performed using ANTs (https://github.com/ANTsX/ANTs/) and the resting-state functional connectivity (RSFC) was calculated using CONN Toolbox (https://www.nitrc.org/projects/conn/). The abnormal pattern of RSFC caused by stroke was determined by the comparison between stroke patients and healthy controls. Sparse canonical correlation analysis (SCCA) was applied to identify abnormal changes of RSFC associated with PSA. PSA subtypes were identified based on the significant canonical correlates using hierarchical clustering. Graph theoretic metrics such as clustering coefficients, global efficiency and local efficiency were calculated and Kruskal-Wallis ANOVA was used to evaluate group differences between various subtypes.Results
Table 1 shows the demographic and clinical data of stoke patients and healthy controls. By two-sample t-test, we identified 189 links of RSFC that were significantly different between stroke patients and healthy controls (Figure 1). SCCA were applied to correlated clinical symptoms and the abnormal links of RSFC. We performed hierarchical clustering based on the canonical variates for RSFC and clinical symptoms and the best clustering scheme was four clusters. We observed significant group differences in graph theoretic metrics including clustering coefficient (F=6.58, df=3 p<0.001), global efficiency (F=4.855, df=3, p=0.003), and local efficiency (F=7.344, df=3, p<0.001) among four subtypes (Figure 2). Post hoc analyses was performed to compare each pair of four groups.Discussion and Conclusion
Various subtypes displayed distinct characteristics in terms of RSFC and graph theoretic metrics. Our study emphasizes the importance of RSFC of neural network in the evaluation of PSA heterogeneity and provides new insights for future research and therapeutic targets.Acknowledgements
No acknowledgement found.References
1. Ferro JM, Caeiro L, Figueira ML. Neuropsychiatric sequelae of stroke. Nat Rev Neurol. 2016;12(5):269-280.
2. Tay J, Morris RG, Markus HS. Apathy after stroke: Diagnosis, mechanisms, consequences, and treatment. Int J Stroke. 2021;16(5):510-518.
3. Drysdale AT, Grosenick L, Downar J, et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat Med. 2017;23(1):28-38.
Figures