2307
A 3.5-minute ultrafast brain MRI and head MRA protocol for evaluation of acute ischemic stroke in the inpatient setting1Massachusetts General Hospital, Boston, MA, United States, 2Siemens Medical Solutions USA, Boston, MA, United States, 3Harvard-MIT Health Sciences and Technology, Boston, MA, United States, 4Siemens Healthcare, Erlangen, Germany
Synopsis
Keywords: Stroke, Stroke, ultrafast MRI, emergency, inpatient, msEPI, compressed sensing, MRA
Motivation: MRI is more sensitive than CT for diagnosing ischemic stroke, yet its use in the acute setting is limited by acquisition time.
Goal(s): To determine the diagnostic performance of an ultrafast 3T brain MRI/head MRA protocol compared to a standard-of-care reference protocol for evaluation of acute ischemic stroke.
Approach: Two raters evaluated diagnostic quality and presence of acute and chronic intracranial findings in 12 inpatients imaged with ultrafast and reference protocols.
Results: Both raters found the ultrafast protocol was of diagnostic quality. Acute infarction, significant vascular findings, and most chronic findings were equally identified on both ultrafast and reference protocols.
Impact: The 3.5-minute ultrafast MR/MRA protocol may improve time to diagnosis and intervention in acute stroke without sacrificing diagnostic quality. It may improve patient throughout and triage in inpatient and emergency settings without compromising diagnosis or patient safety.
Introduction
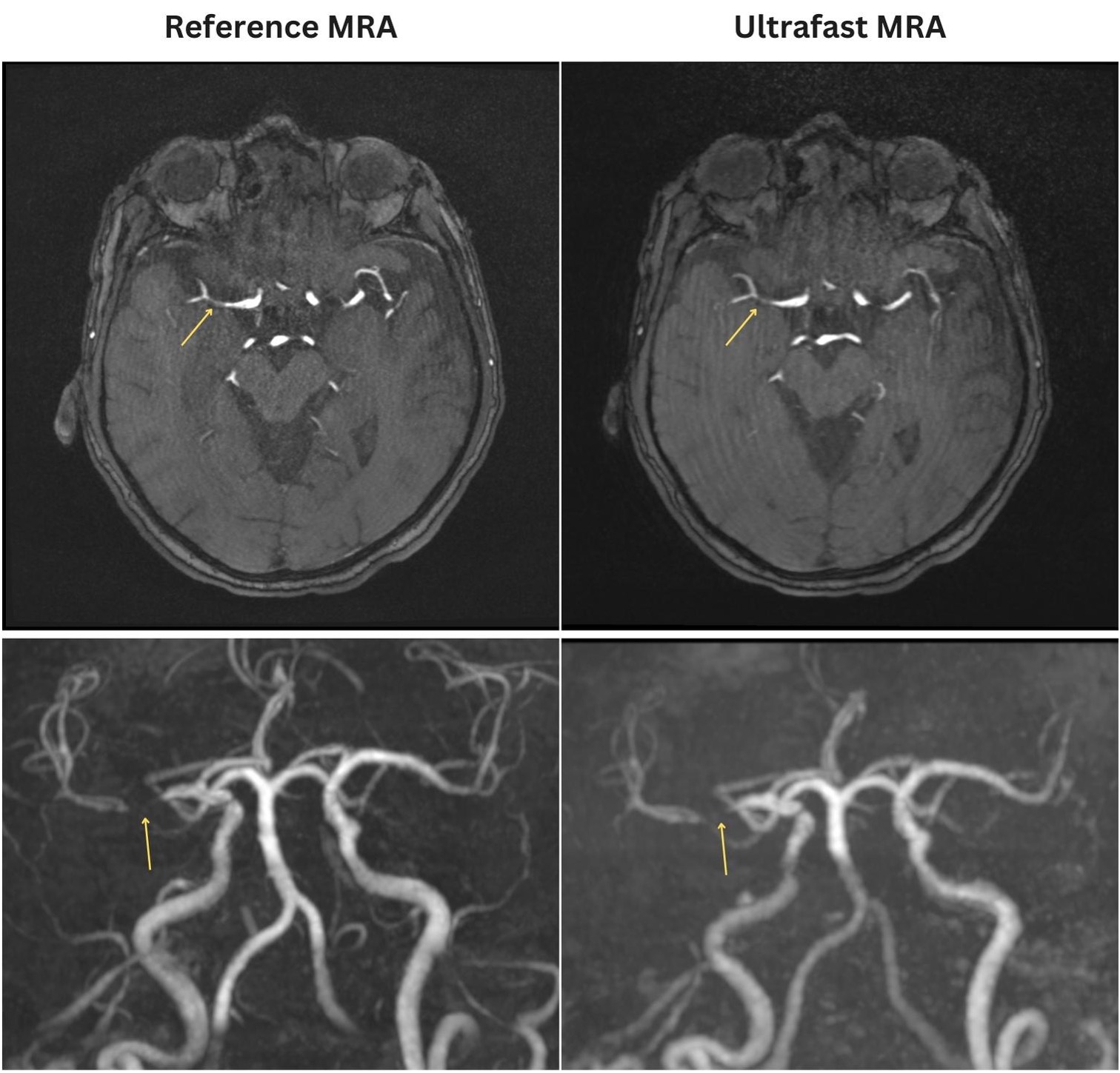
There is increasing utilization of magnetic resonance imaging (MRI) in the emergency setting.1 MRI is superior to CT for assessment of parenchymal integrity, tissue viability, and ischemic core in acute stroke.2,3 Time-of-flight (TOF) head MRA is important for evaluation of large vessel occlusion and severe stenosis.4 Fast MRI sequences have been developed to address these limitations but are often plagued by artifacts or poor image quality.5,6 We developed a 3.5-minute ultrafast brain MRI/head MRA protocol for rapid and accurate evaluation of acute ischemic stroke using a combination of multi-shot echo planar imaging, Compressed Sensing TOF-MRA, and AI-assisted reconstruction.7 Here, we assessed the diagnostic performance of the ultrafast protocol for evaluation of acute ischemic stroke in the inpatient setting.Methods
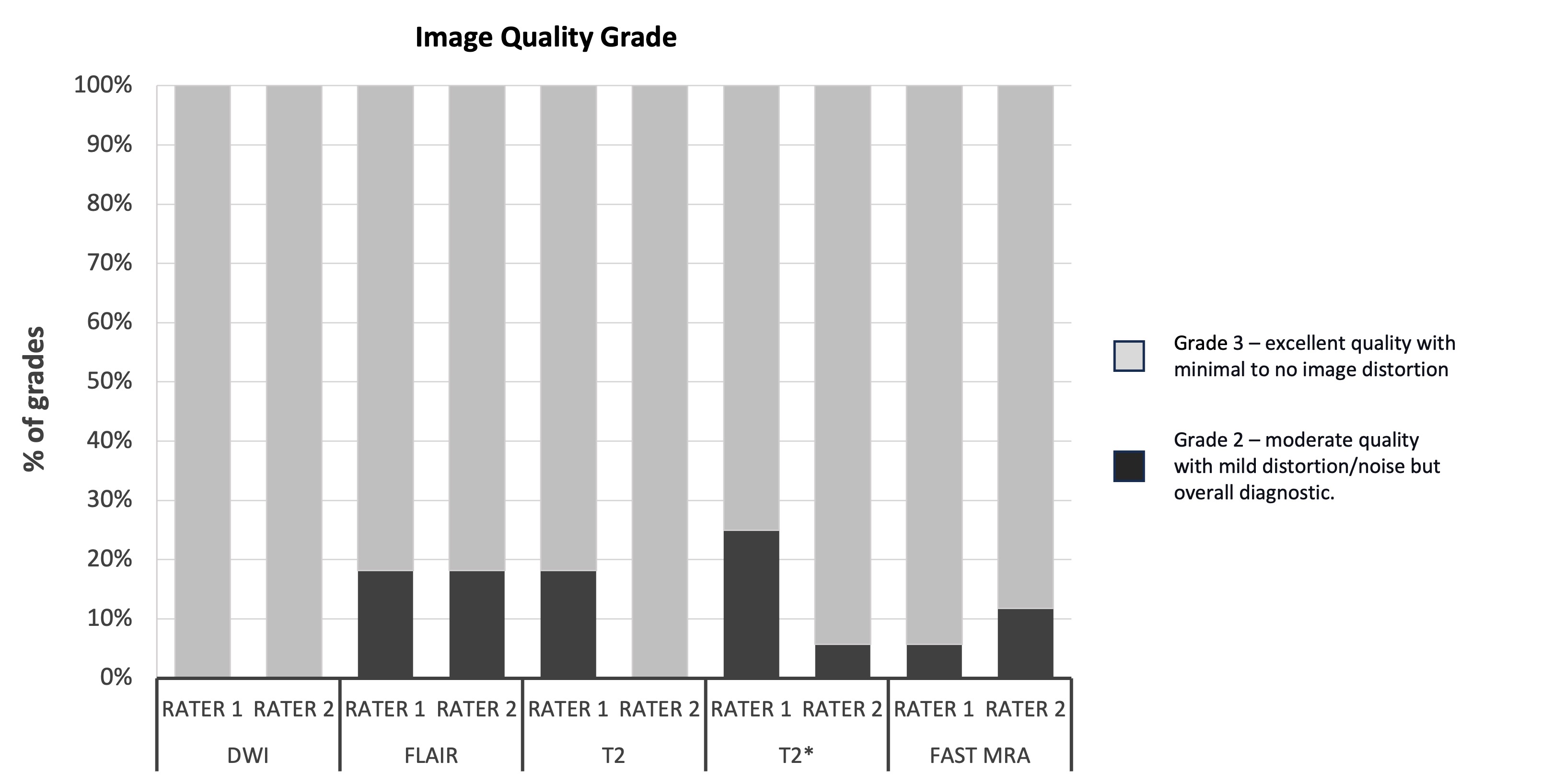
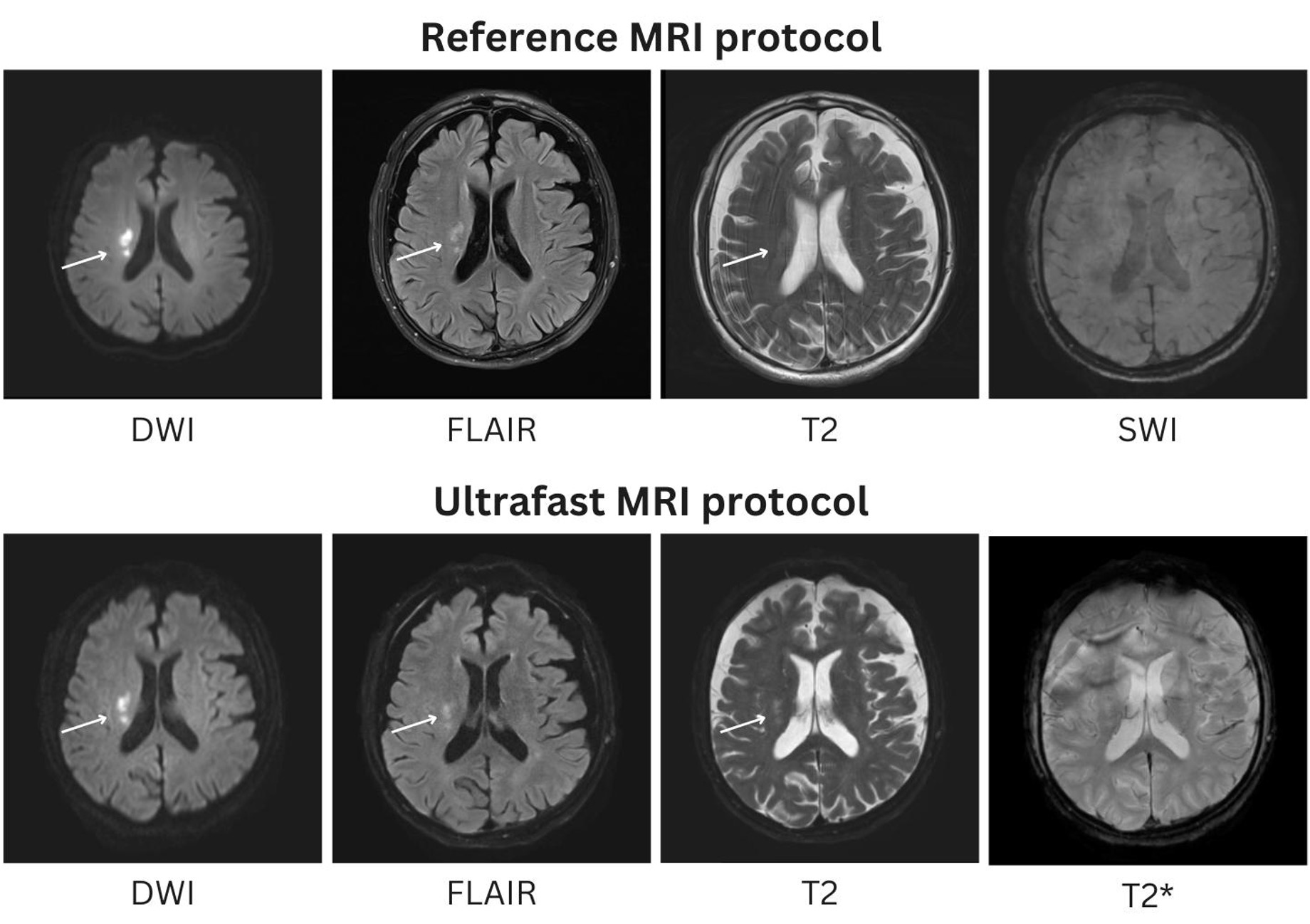
This single center retrospective study included adult inpatients undergoing evaluation for acute stroke. Patients were scanned with the ultrafast stroke MRI/head MRA and reference brain MRI/head MRA protocols between 9/1/2023 and 10/25/2023. Both the ultrafast and reference protocols included: axial DWI, axial FLAIR, axial T2, axial T2* or SWI, and TOF head MRA. The acquisition time was 3.5 minutes for the ultrafast protocol and 9 minutes for the reference protocol. Data was collected on a 3T MRI scanner (MAGNETOM Vida; Siemens Healthcare) using a 20-channel head/neck coil. The MR images from the two protocols were evaluated and rated by two neuroradiologists. The ultrafast MRI/MRA sequences were assessed for diagnostic quality on a 3-point scale (1 – poor quality and nondiagnostic, 2 – moderate quality with mild distortion/noise but overall diagnostic, and 3 – excellent quality with minimal to no image distortion.8 The ultrafast MRI/MRA and reference MRI/MRA protocol images were presented in a blinded, randomized fashion. Raters evaluated the MR images for acute/subacute infarct, acute/old hemorrhage, intracranial mass and mass effect, hydrocephalus, and other intracranial findings. For the MRA images, the raters evaluated for large vessel occlusion, severe arterial stenosis, aneurysm and vascular malformation.Results
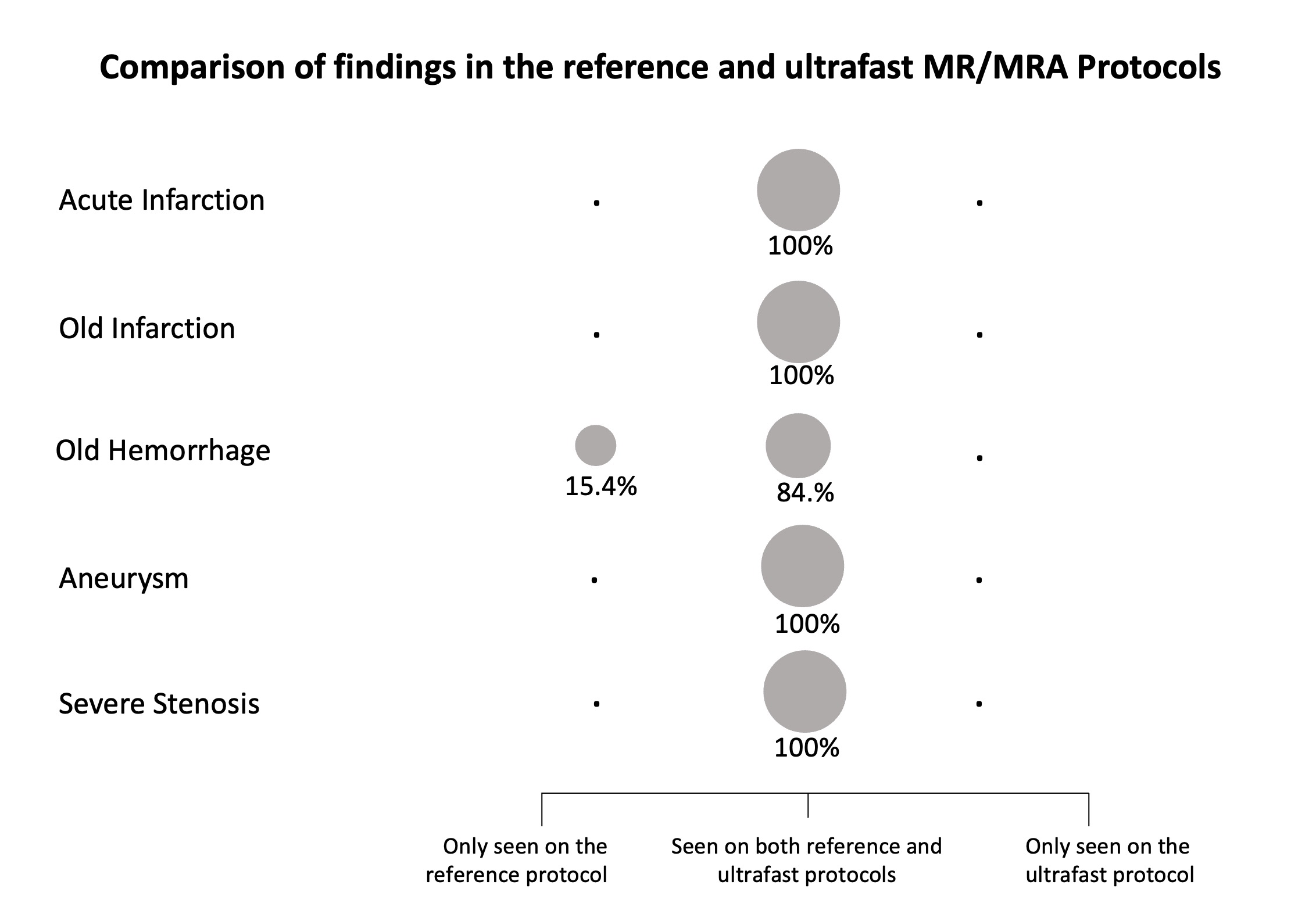
12 patients (4 males, median age 70) were included in this study. Both raters found all the ultrafast protocol sequences to be of diagnostic quality (score>2; Table 1). On the reference MRI, two patients (16.7%) had acute infarct. On the reference MRA, one patient (8.3%) had severe stenosis of the right M1 division, and one patient (8.3%) had a small right supraclinoid ICA aneurysm. There was 100% concordance of these findings on the ultrafast protocol images by both raters. In terms of chronic findings, 2 patients (16.7%) had old infarcts and 6 patients (50%) had chronic microhemorrhages. Aside from rater 1 missing a small chronic microhemorrhage on the ultrafast MR protocol, all other chronic findings were concordant on the ultrafast MR protocol as compared to the reference MR protocol.Discussion
Acute ischemic stroke requires timely diagnosis and intervention to optimize outcomes and to reduce potential neurological deficits. MRI is a powerful tool for ischemic stroke evaluation, but its utility has been limited by accessibility, long scan times and sensitivity to motion.9,10 The acquisition time of the ultrafast MR/MRA protocol was 5.5 minutes faster (61% reduction) compared to the reference protocol, allowing for more rapid diagnosis and intervention. The shorter scan time may also improve patient comfort and reduce the likelihood of motion artifacts, which is especially important for acute stroke patients who may find it challenging to remain still for extended periods.Importantly, the ultrafast MR/MRA protocol was comparable to the reference MR/MRA protocol in the detection of acute ischemic stroke and intracranial findings. Although the results are preliminary and drawn from a small sample size, no acute findings were missed on the ultrafast protocol, and all relevant vascular and chronic findings were identified by both raters. The raters found the overall diagnostic performance to be similar between the two protocols. Our results suggest that inpatient and emergency department patients could benefit immensely from this protocol, as the ultrafast exam would help optimize patient throughput and triage without compromising diagnostic fidelity.
The MR acceleration and reconstruction techniques in this protocol can also be implemented for other brain MRI protocols in the emergency, inpatient, and outpatient settings, as well as other patient populations such as pediatric patients. The broader impact of these techniques include improved patient access, reduced call backs for motion degradation, improved patient throughput, and potentially improved patient outcomes through increasing the availability of imaging in the acute setting.11
Conclusion
Our preliminary results suggest that the ultrafast brain MRI/head MRA protocol was as accurate as the reference MRI/MRA protocol for diagnosis of acute intracranial findings and notable vascular findings and was nearly as good for detecting chronic intracranial findings.Acknowledgements
We'd like to thank RSNA for supporting this project through the RSNA Resident Research Grant.References
1. Kelen GD, Wolfe R, D'Onofrio G, et al. Emergency Department Crowding: The Canary in the Health Care System. N Engl J Med Catalyst 2021.
2. Garcia-Bermejo P, Castano C, Davalos A. Multimodal CT versus MRI in Selecting Acute Stroke Patients for Endovascular Treatment. Interv Neurol 2013; 1(2): 65-76.
3. Chalela JA, Kidwell CS, Nentwich LM, et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet 2007; 369(9558): 293-8.
4. Bash S, Villablanca JP, Jahan R, et al. Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR Am J Neuroradiol 2005; 26(5): 1012-21.
5. Skare S, Sprenger T, Norbeck O, et al. A 1-minute full brain MR exam using a multicontrast EPI sequence. Magn Reson Med 2018; 79(6): 3045-54.
6. Ryu KH, Choi DS, Baek HJ, et al. Clinical feasibility of 1-min ultrafast brain MRI compared with routine brain MRI using synthetic MRI: a single center pilot study. J Neurol 2019; 266(2): 431-9.
7. Clifford B, Conklin J, Huang SY, et al. An artificial intelligence-accelerated 2-minute multi-shot echo planar imaging protocol for comprehensive high-quality clinical brain imaging. Magn Reson Med 2022; 87(5): 2453-63.
8. Nael K, Khan R, Choudhary G, et al. Six-minute magnetic resonance imaging protocol for evaluation of acute ischemic stroke: pushing the boundaries. Stroke 2014; 45(7): 1985-91.
9. Provost C, Soudant M, Legrand L, et al. Magnetic Resonance Imaging or Computed Tomography Before Treatment in Acute Ischemic Stroke. Stroke 2019; 50(3): 659-64.
10. Allen LM, Hasso AN, Handwerker J, Farid H. Sequence-specific MR imaging findings that are useful in dating ischemic stroke. Radiographics 2012; 32(5): 1285-97; discussion 97-9.
Figures