2302
Quantifying early haemodynamic treatment effects in carotid stenosis using arterial transit artifacts and spatial CoV on ASL-MRI1Neuroradiology, UCL Queen Square Institute of Neurology, London, United Kingdom, 2Neuroradiology, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 3Division of Surgery and Interventional Science, University College London Hospitals, London, United Kingdom, 4Department of Medical Statistics, London School of Hygiene and Tropical Medicine, London, United Kingdom, 5Stroke Research Centre, UCL Queen Square Institute of Neurology, London, United Kingdom, 6Department of Medical Physics and Biomedical Engineering, University College London Hospitals, London, United Kingdom
Synopsis
Keywords: Stroke, Perfusion, sCoV
Motivation: There is little understanding of how arterial transit artefacts (ATA) on ASL-MRI, which indicate regions of haemodynamic compromise, change in patients with carotid artery stenosis following optimised medical therapy versus surgical revascularisation.
Goal(s): To assess treatment effects using visually rated ATA severity and a spatial coefficient of variance before and after optimised medical therapy versus additional surgical revascularisation.
Approach: We visually rated ATAs using an established four-point grading system and computed the spatial coefficient of variance in corresponding regions.
Results: Both methods demonstrated only surgical revascularisation led to significant improvements in haemodynamics 1-month post-treatment, solely within the ipsilateral middle cerebral artery cortical territory.
Impact: A robust method of quantifying early haemodynamic treatment effects could be used to identify who truly benefits from surgical revascularisation in the long-term. Future work will correlate these measures to long-term clinical outcomes.
Introduction
Haemodynamic compromise resulting from stenosis of the upstream circulation can manifest as serpiginous intravascular signals on arterial spin labelling (ASL) MRI called arterial transit artefacts (ATAs). They indicate delayed arrival of blood water protons from the ASL-labelling plane to the brain parenchyma1.To improve cerebral haemodynamics and ultimately clinical outcomes, patients with carotid artery stenosis (CAS) can be offered surgical revascularisation in addition to optimised medical therapy (OMT). This depends on their symptomaticity and degree of stenosis estimated on angiography without input from other imaging modalities such as ASL-MRI2,3. The presence of ATAs is associated with recent ischaemic symptoms in patients with 70-99% stenosis4. Therefore quantification of ATAs has potential to become a biomarker and support identifying other subpopulations who may benefit from surgery and those who will not.
ATAs can be graded semi-quantitatively by a radiologist using a 4-point system without the need for any image post-processing1.However, visual assessment requires training, is time-intensive, affected by inter-rater variability and traditionally is done in ten cortical regions on two slices that could fail to comprehensively capture the full extent of hemodynamic changes.
An alternative automated method of assessing hemodynamic impairment, the spatial coefficient of variation (sCoV), has been proposed. It has been shown as a proxy for arterial transit time measurement and can predict lateralisation of carotid stenosis5. However, it requires advanced processing that might not be available in the standard clinical setting.
This work aims to systematically quantify early hemodynamic changes after two different treatments: OMT or OMT with surgery using both visual grading and sCoV. We hypothesise that in patients with severe hemodynamic impairment, surgery will improve the visual ATA score and reduce sCoV.
Methods
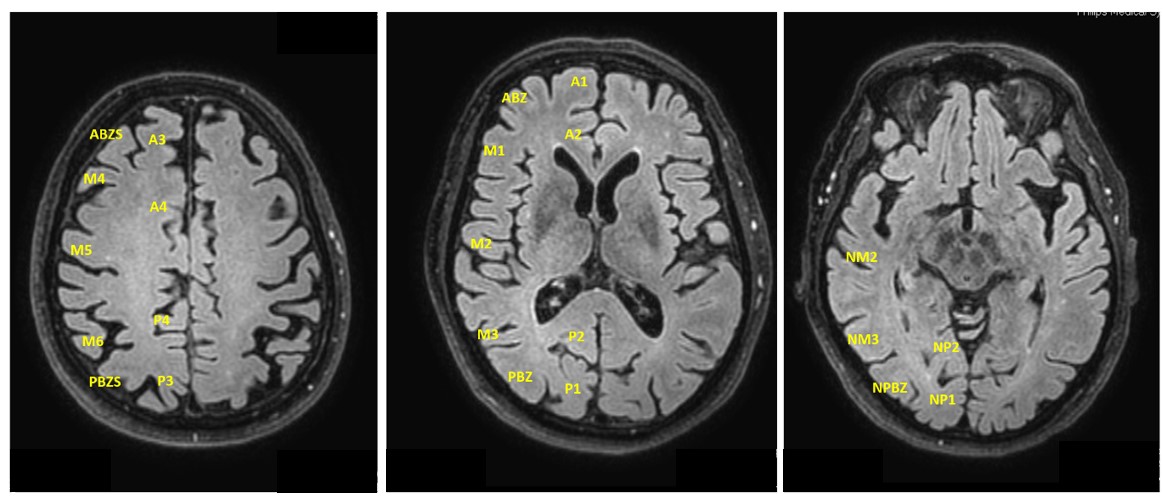
44 participants from the ECST-2 trial6 with ≥50% CAS underwent pseudocontinuous ASL-MRIs (2D-EPI pCASL) and 3D-MPRAGE (table 1) at baseline and 1-month post-surgical treatment (n=22) or initiation of OMT. All scans were performed on a 3T scanner (Achieva, Philips Medical Systems, Best, The Netherlands). ASL consisted of: 35 control-label background-suppressed pCASL pairs with 1.8s labelling, 1.8s post-labelling delay and a separate calibration proton density image. ASL data were motion corrected and cerebral blood flow (CBF) maps were generated using an in-house pipeline7.ATAs were graded on CBF maps from 0-3: 0=no or minimal ASL signal; 1=moderate ASL signal with ATA; 2=high ASL signal with ATA; 3=normal perfusion1. ASPECTS rating1 was expanded to include the superficial border zones between major cerebrovascular territories, the parasagittal cortex and infraganglionic regions resulting in 46 distinct regions across 3 different levels (Figure 1). MRIs were independently rated by two reviewers blinded to clinical information and a consensus score was agreed. A final ATA score was calculated as a percentage of the summed scores of all composite regions within that given hemisphere or large vessel territory divided by the maximum possible. The sCoV was computed for both cerebral hemispheres and each major cerebrovascular territory according to established methodology5,8. Cortical segmentation of 3D-MPRAGE was performed using SynthSeg9 and all co-registrations using Nifty-Reg10.
Changes in the percentage ATA score and sCoV for each region were calculated by subtracting the 1-month values from the baseline. Comparison of the ATA score and sCoV was performed on a hemispheric level. Significance was assessed using one-way ANOVA, two-tailed t-tests and r2. Statistical analysis was performed using R.
Results
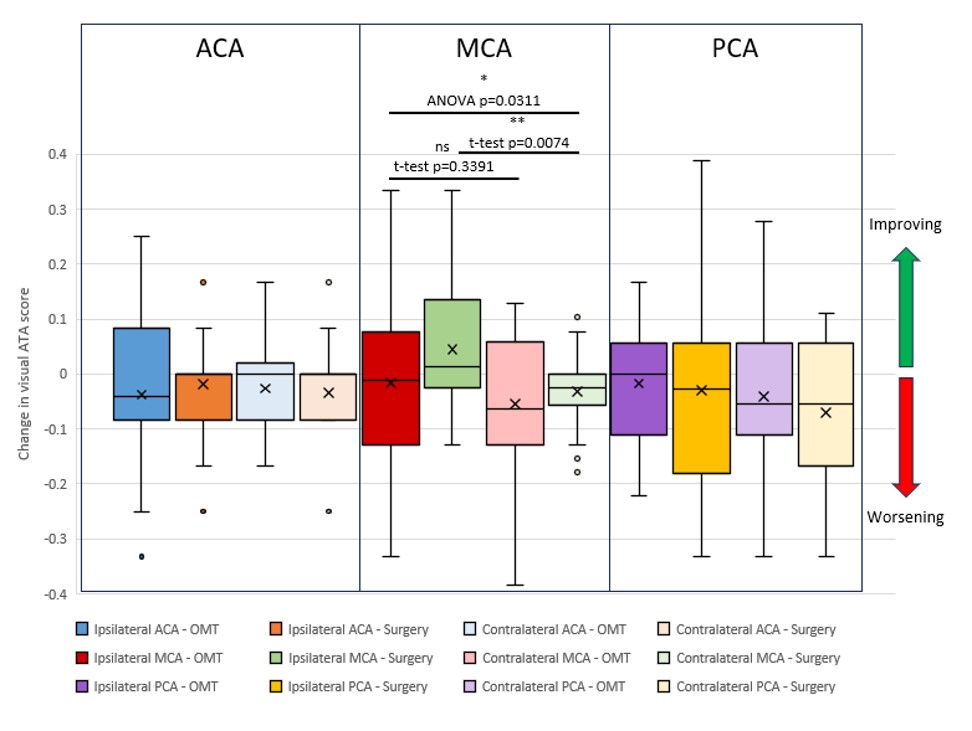
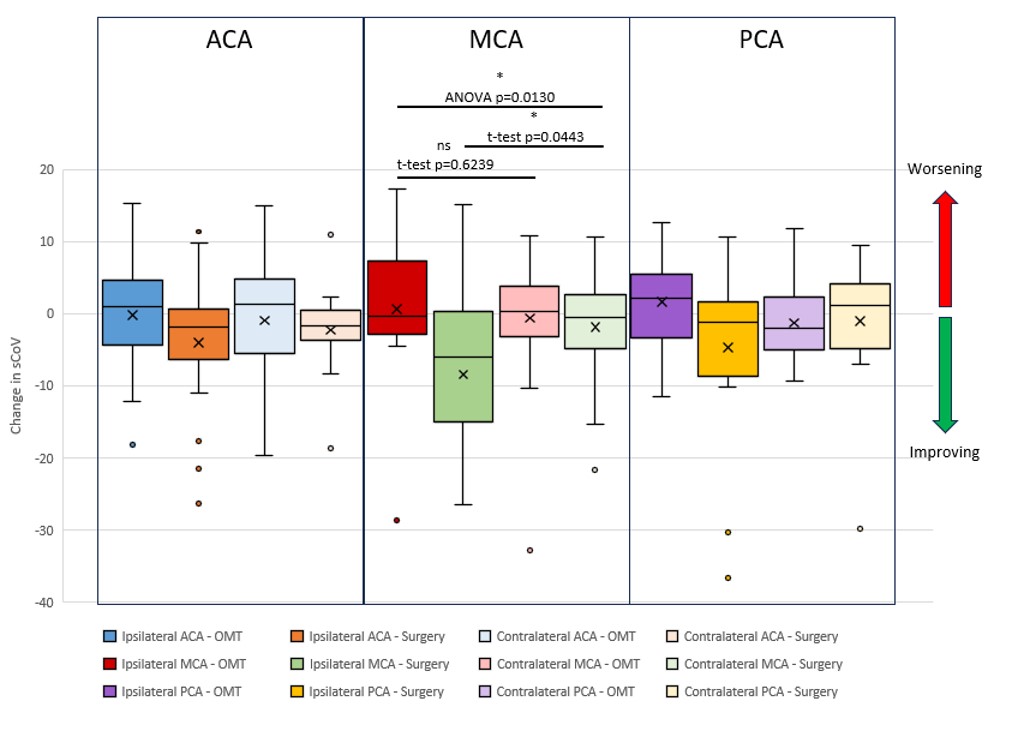
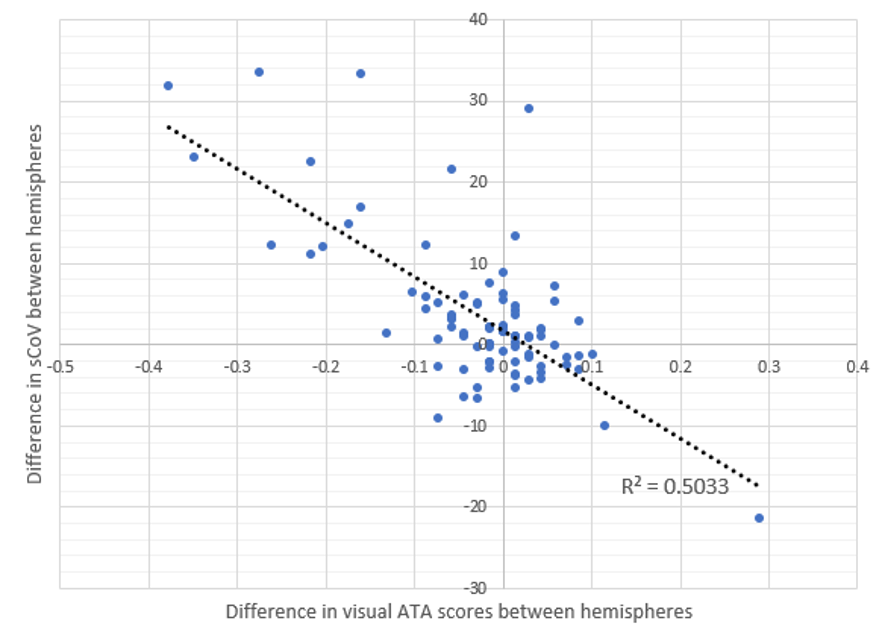
One-way ANOVA demonstrated that only the MCA territory showed significant differences in the mean change in ATA score (p=0.0311) and sCoV (p=0.0130) for different treatment arms and sides. On average, patients who underwent surgery showed significantly higher ATA scores (+4.43%, p=0.0074) and lower sCoV (-8.45, p=0.0443) within the ipsilateral MCA region after 1-month. This was not seen with OMT.There is a significant negative correlation between the hemispheric difference in ATA scores and the hemispheric difference in sCoV (r2=0.5033, p<0.0001). No other statistically significant relationship between the ATA scores and sCoV was found.
Discussion
This work quantifies early hemodynamic changes in CAS patients undergoing OMT or surgery using an ATA score and sCoV on ASL-MRI images. As hypothesised, short-term haemodynamic parameters only improved after surgical revascularisation. The largest improvement was observed in the MCA territory using both the ATAs score and sCoV. A correlation was found between the two, but only when comparing differences between hemispheres within the same scanning session. This suggests that both visual rating and sCoV are consistent within a single scan, but not between different timepoints.Conclusion
Both measures of haemodynamic impairment appear to respond consistently with surgical restoration of adequate flow. Future work will aim to correlate these changes in ATA scores and sCoV to clinical outcomes.Acknowledgements
No acknowledgement found.References
Zaharchuk G, Do HM, Marks MP, Rosenberg J, Moseley ME, Steinberg GK. Arterial spin-labeling MRI can identify the presence and intensity of collateral perfusion in patients with moyamoya disease. Stroke. 2011 Sep;42(9):2485-91. doi: 10.1161/STROKEAHA.111.616466. Epub 2011 Jul 28. PMID: 21799169; PMCID: PMC3164217.
van Laar PJ, van der Grond J, Moll FL, Mali WPTM, Hendrikse J. Hemodynamic effect of carotid stenting and carotid endarterectomy. J Vasc Surg 2006;44(1):73–8. Available from: https://www.sciencedirect.com/science/article/pii/S0741521406004782
Naylor AR, Ricco JB, de Borst GJ et al. Editor's Choice - Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018 Jan;55(1):3-81. doi: 10.1016/j.ejvs.2017.06.021. Epub 2017 Aug 26. PMID: 28851594.
Di Napoli A, Cheng SF, Gregson J, Atkinson D, Markus JE, Richards T, Brown MM, Sokolska M, Jäger HR. Arterial Spin Labeling MRI in Carotid Stenosis: Arterial Transit Artifacts May Predict Symptoms. Radiology. 2020 Dec;297(3):652-660. doi: 10.1148/radiol.2020200225. Epub 2020 Oct 13. PMID: 33048034.
Mutsaerts HJMM, Petr J, Bokkers RPH, Lazar RM, Marshall RS, et al. (2020) Spatial coefficient of variation of arterial spin labeling MRI as a cerebrovascular correlate of carotid occlusive disease. PLOS ONE 15(2): e0229444. https://doi.org/10.1371/journal.pone.0229444
Cheng, S.F., van Velzen, T.J., Gregson, J. et al. The 2nd European Carotid Surgery Trial (ECST-2): rationale and protocol for a randomised clinical trial comparing immediate revascularisation versus optimised medical therapy alone in patients with symptomatic and asymptomatic carotid stenosis at low to intermediate risk of stroke. Trials 23, 606 (2022). https://doi.org/10.1186/s13063-022-06429-z
Alsop DC, et al. Recommended implementation of arterial spin‐labeled perfusion MRI for clinical applications: a consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73:102–116.
Liu CF, Hsu J, Xu X, Kim G, Sheppard SM, Meier EL, Miller MI, Hillis AE, Faria AV. Digital 3D Brain MRI Arterial Territories Atlas. Sci Data. 2023 Feb 4;10(1):74. doi: 10.1038/s41597-022-01923-0. PMID: 36739282; PMCID: PMC9899211.
Billot B, Greve DN, Puonti O, Thielscher A, Van Leemput K, Fischl B, Dalca AV, Iglesias JE; ADNI. SynthSeg: Segmentation of brain MRI scans of any contrast and resolution without retraining. Med Image Anal. 2023 May;86:102789. doi: 10.1016/j.media.2023.102789. Epub 2023 Feb 25. PMID: 36857946; PMCID: PMC10154424.
Figures