2298
Clinical feasibility of accelerated diffusion weighted imaging with deep learning reconstruction for patients with acute neurologic symptoms1Chung-Ang University Hospital, Seoul, Korea, Republic of, 2Severance Hospital, Seoul, Korea, Republic of
Synopsis
Keywords: Stroke, Ischemia
Motivation: Timely diagnosis of patient with acute neurologic symptom is critical. Detecting small lesions on DWI can be challenging and experience plays a significant role, especially when motion artifacts affect image quality.
Goal(s): Our goal was to shorten acquisition time and provide highly sensitive images of small lesions, particularly for emergency clinicians unfamiliar with DWI.
Approach: We included 80 patients, comparing quantitative and qualitative analyses between conventional and deep-learning DWI. We assessed diagnostic performance among experienced neuroradiologists and primary care physician.
Results: Results showed similar image quality between two sequences, but deep-learning DWI exhibited superior lesion conspicuity. Diagnostic accuracy remained consistent between the two.
Impact: Deep-learning DWI offers comparable image quality with significant shorter acquisition time. It also enhances detection of tiny brain lesion, providing diagnostic confidence to less experienced clinicians in emergency situation.
Introduction
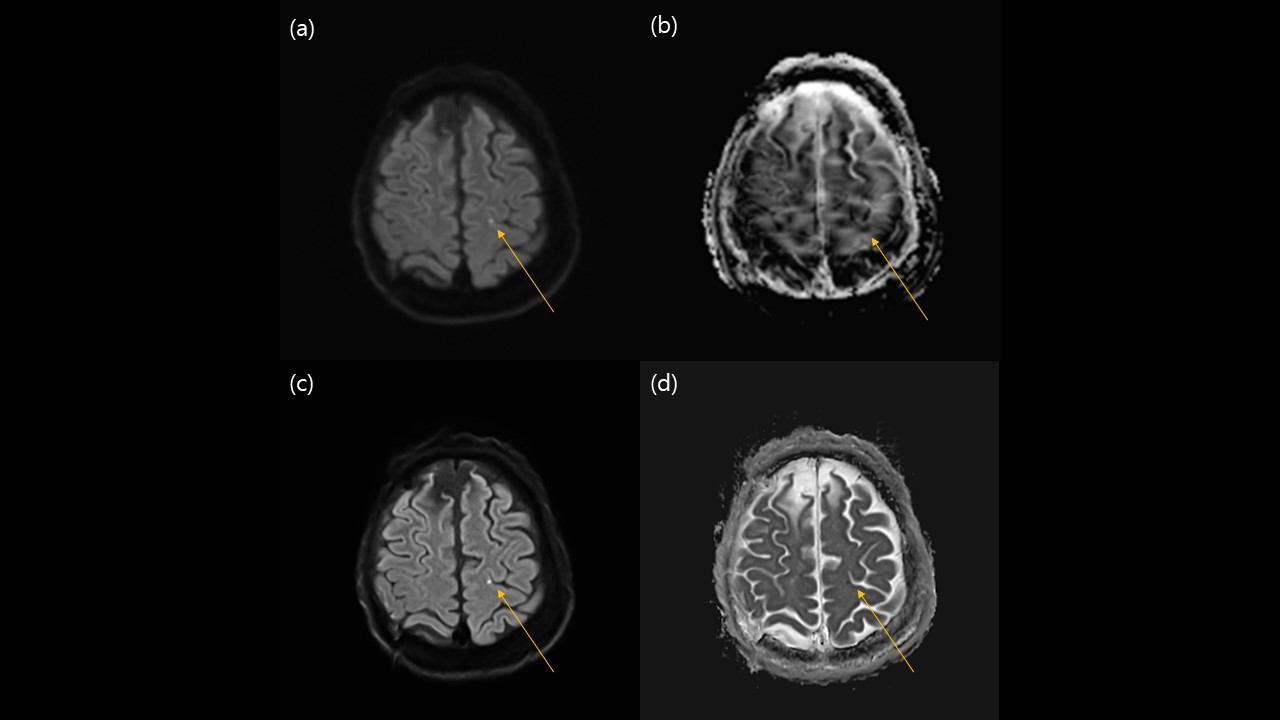
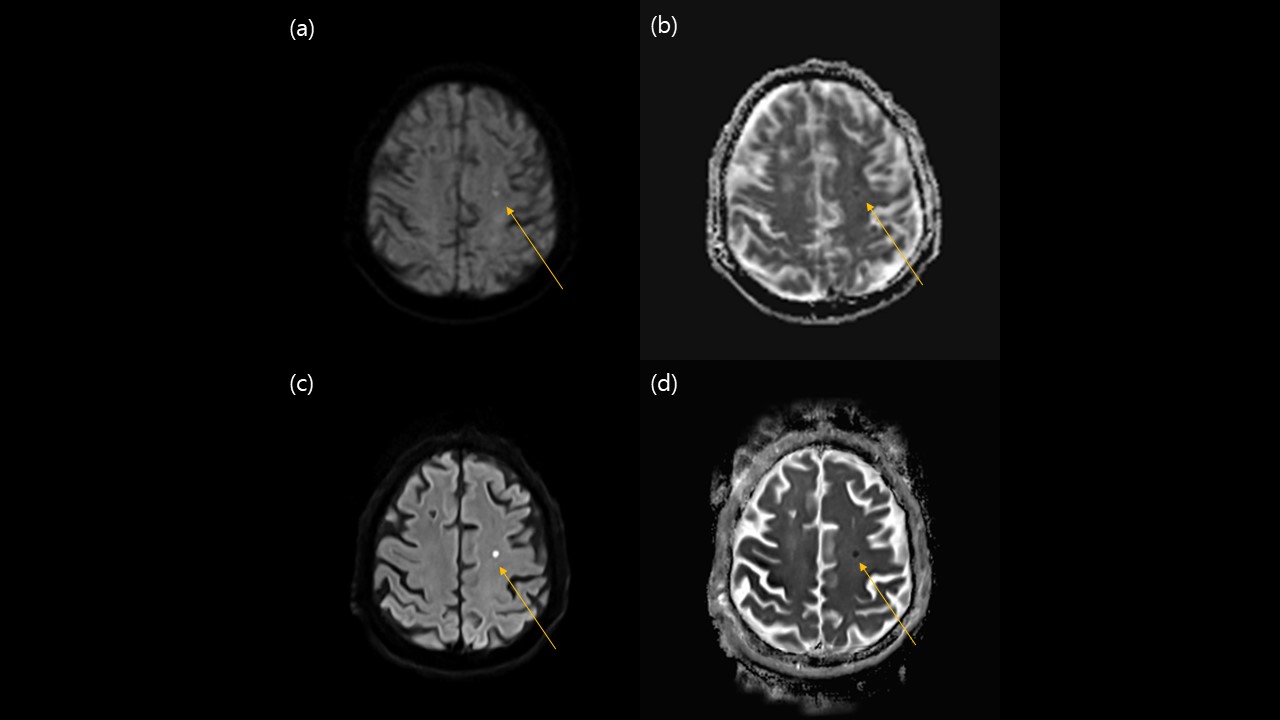
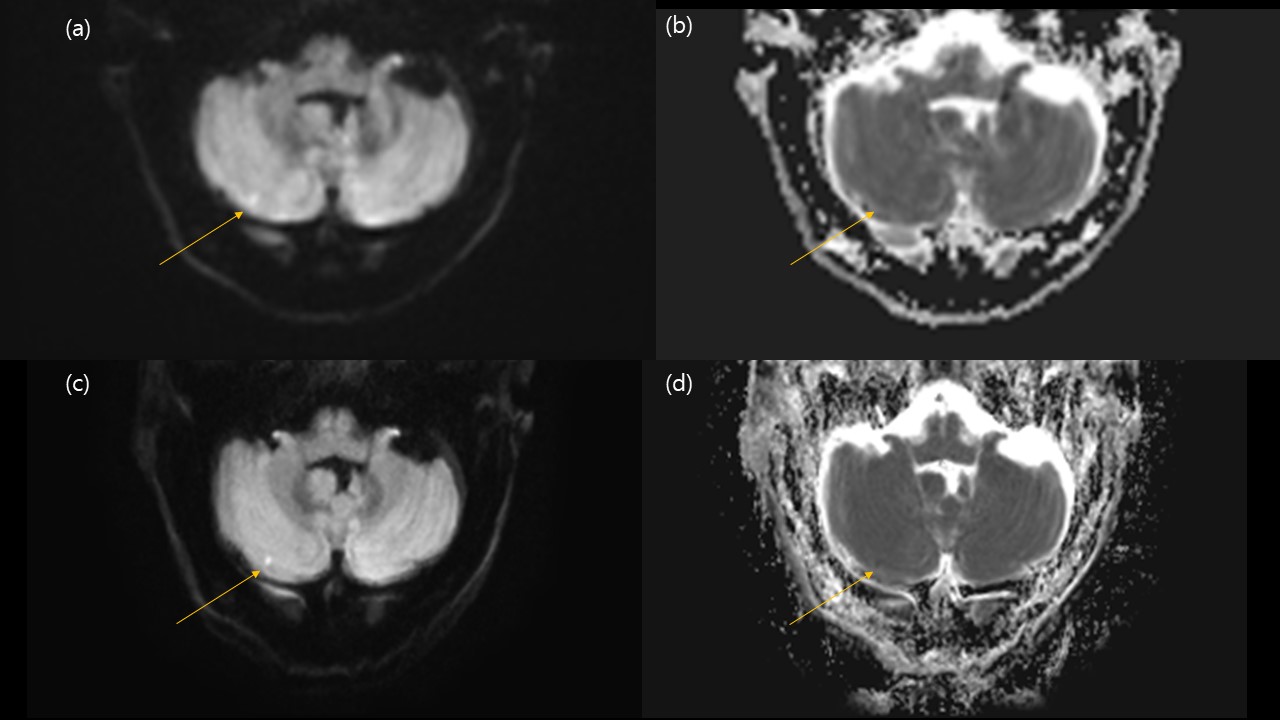
In emergency situations, swiftly diagnosing patients with acute neurologic symptoms is crucial for preventing severe cerebrovascular accidents. Detecting small lesions is important not only to confirm the clinical diagnosis, but also facilitate the recognition of certain patterns of ischemia, thereby providing clues to the underlying etiology (1). However, it is hard and even can be neglected when motion artifact hinders the image quality. It is more challenging for the emergency clinicians who are unfamiliar with diffusion weighted imaging (DWI). This study aimed to evaluate and assess the clinical feasibility of accelerated deep learning reconstructed (DL) DWI (2, 3) in detecting small diffusion restricted lesion (<5mm size) in patients with acute neurologic symptoms.Methods
Total 80 patients (F:M 43:37, 62.15±17.5 years) who visited emergency room with acute neurologic symptoms (dizziness 29, headache 6, weakness 15, loss of consciousness 12, others 18) in single tertiary referral hospital were included. All patients underwent both conventional DWI and DL-DWI. Image quality (overall image quality and lesion conspicuity) was scored by two board-certified neuroradiologists independently and compared using the five-point scale. The apparent diffusion coefficient (ADC) was measured in five locations of the brain (bilateral centrum semiovale, bilateral putamen, and pons) and compared between two DWI sequences. Also, we compared diagnostic performance among two experienced neuroradiologists and one primary care physician who is inexperienced with brain imaging.Results
The mean acquisition time for the DL-DWI (49 sec) was significantly shorter (P < 0.001) than conventional DWI (165 sec). Diagnostic accuracy for conventional DWI was 97.50% and for DL-DWI, it was 97.92%. Inexperienced physician achieved similar diagnostic performance with both conventional DWI and DL-DWI (sensitivity = 87.10%, specificity = 97.96%, PPV = 93.75%, NPV = 96.43%, accuracy = 92.31%). Neuroradiologists evaluated two sequences show similar image quality (4.44 ± 0.60 vs. 4.36 ± 0.59, P = 0.2641), but DL-DWI showed better lesion conspicuity (4.47 ± 0.67 vs. 4.71 ± 0.52, P = 0.0271). ADC value of DL-DWI was significantly lower than that of conventional DWI in centrum semiovale (0.76 ± 0.06 vs. 0.71 ± 0.06 x 10-3 mm2/s, P < 0.0001), basal ganglia (0.74 ± 0.007 vs. 0.66 ± 0.009 x 10-3 mm2/s, P < 0.0001), and pons (0.77± 0.08 vs. 0.73 ± 0.11 x 10-3 mm2/s, P = 0.0072).Discussion and conclusion
Our study demonstrates that DL-DWI is feasible acquisition technique in daily practice dealing with patients at risk of intracranial ischemic events. DL-DWI showed comparable diagnostic performance and maintains good image quality while significantly cutting down on scan time compared to conventional DWI. Additionally, we speculated that DL-DWI offers better lesion conspicuity than conventional DWI, potentially leading to increase confidence in detecting small brain lesions that might otherwise overlooked but could serve as crucial indicators of future cerebrovascular accident.Acknowledgements
No acknowledgement found.References
1. Gass A, Ay H, Szabo K, Koroshetz WJ. Diffusion-weighted MRI for the “small stuff”: the details of acute cerebral ischaemia. The Lancet Neurology. 2004;3(1):39-45.
2. Bae SH, Hwang J, Hong SS, Lee EJ, Jeong J, Benkert T, et al. Clinical feasibility of accelerated diffusion weighted imaging of the abdomen with deep learning reconstruction: Comparison with conventional diffusion weighted imaging. European Journal of Radiology. 2022;154:110428.
3. Kits A, De Luca F, Kolloch J, Müller S, Mazya MV, Skare S, et al. One‐minute multi‐contrast Echo planar brain MRI in ischemic stroke: A retrospective observational study of diagnostic performance. Journal of Magnetic Resonance Imaging. 2021;54(4):1088-95.
Figures