2285
Structural and Functional Alterations with Proprioception Deficits in Chronic Ankle Instability1Radiology, Huashan Hospital, Fudan University, Shanghai, China, Shanghai, China, 2Sports Medicine, Huashan Hospital, Fudan University, Shanghai, China, Shanghai, China, 3MR Research Collaboration, Siemens Healthineers Ltd., Shanghai, China, Shanghai, China, 4Application Developments, Siemens Shenzhen Magnetic Resonance Ltd., 518057 Shenzhen, China, Shanghai, China
Synopsis
Keywords: Functional/Dynamic, fMRI (resting state)
Motivation: Understanding the neuropathological mechanisms of chronic ankle instability (CAI) is clearly of interest to both the practicing clinician and researchers on sports medicine.
Goal(s): Ankle proprioception deficits occur in patients with CAI. The underlying central neuropathology is unclear. This study examined cerebellar vermis structure/function in CAI patients vs controls and associations with proprioception deficits.
Approach: This research is a cross-sectional laboratory investigation.
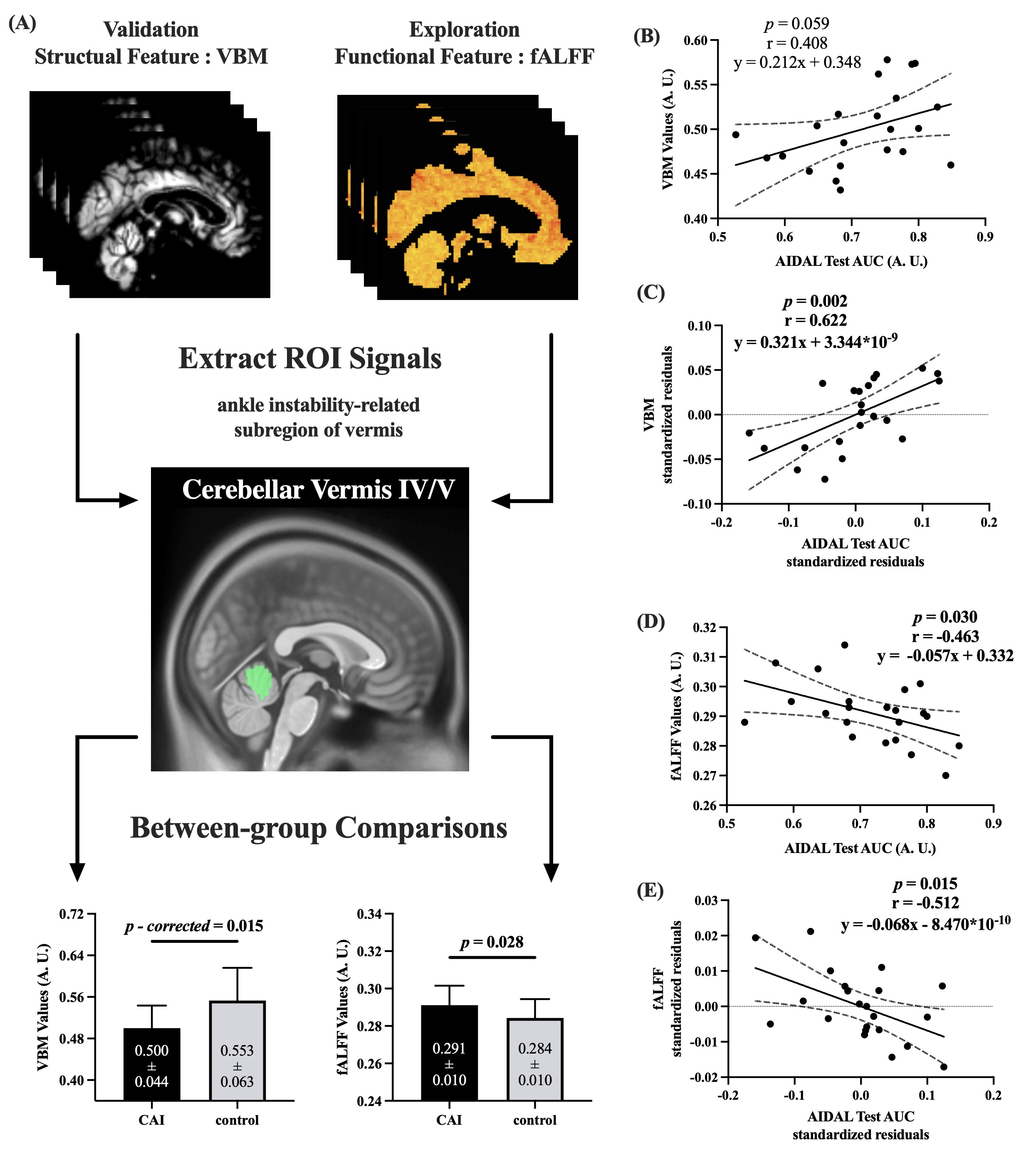
Results: Patients with CAI showed reduced gray matter volume (VBM) and increased functional connectivity (fALFF) in cerebellar vermis subregions IV/V compared to controls. Proprioceptive deficits in CAI patients were associated with lower VBM and higher fALFF values in these subregions.
Impact: We hope the similar strategies could be applied to modulate our observed compensatory overactivation of vermis, make cerebellum more more efficient when handling the increased proprioceptive demands, and finally bring optimal clinical function to the patients with CAI.
Introduction
Ankle sprain is one of the most common injuries incurred during participation in sports, especially the ones involving jumping and landing actions [1]. Furthermore, it is estimated that more than 40% of the patients with a first-time ankle sprain would develop chronic ankle instability (CAI), manifesting as recurrent sprains, self-reported feelings of “instability”, and ankle giving way [2]. Even worse, early-onset osteoarthritis and physical disability would also be induced eventually [3]. Till now, there were still no effective therapeutic strategies for CAI because the sprained ankle might have not only mechanical instability but also persistent sensorimotor deficits [4]. As a result, understanding the neuropathological mechanisms of CAI is clearly of interest to both practicing clinicians and researchers in sports medicine.The cerebellar vermis plays a critical role in proprioception, which collects the proprioceptive information originating from joints ascending through the posterior and anterior spinocerebellar tract to distinguish the appropriate spatial positions of joints [5-6]. Resting-state functional magnetic resonance imaging (rs-fMRI) is a noninvasive technology to measure the blood oxygen level-dependent signals (BOLD) of intrinsic brain activity and its spatial distributions of low-frequency oscillations [7].
The aim of the current study was two-folded: (i) replicating the observation of vermis atrophy (measured by VBM), and then exploring the functional difference of activity intensity (measured by fALFF) in vermis between patients with CAI and healthy controls without a history of ankle injury; (ii) determining the correlation between the ankle proprioception deficits in CAI and the structural/functional features of vermis. We hypothesized that patients with CAI would have lower VBM and fALFF values in vermis than those of controls, which would also be positively correlated with the ankle proprioception in patient group
Method
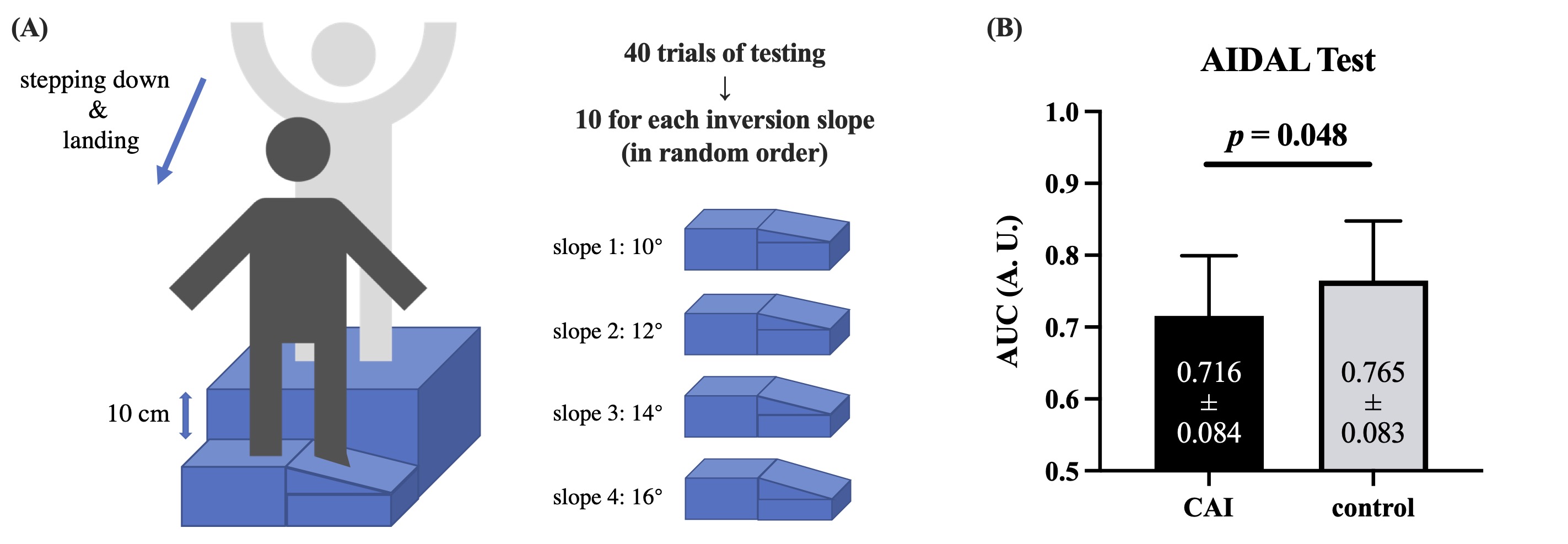
Twenty-two patients and twenty-five control individuals were enrolled in a cross-sectional investigation. All participants underwent structural and resting-state functional magnetic resonance imaging scanning to calculate voxel-based morphometry (VBM) and fractional amplitude of low-frequency fluctuation (fALFF) of the vermis. Between-group comparisons of the ankle instability-related subregions of the vermis were performed. Correlation analyses were performed between the outcomes of the surviving subregions and the proprioceptive scores of the ankle inversion discrimination apparatus for the landing test.All MRI images were quality-controlled by an experienced technologist blinded to the group assignment, and acquired by one 3.0 Tesla Prisma scanner (Siemens, Erlangen, Germany). The participants were fixed with their heads cushioned by foam pads to minimize head motion. Two appropriately sized earplugs were applied to reduce noise, and the scanning would be terminated if the subject complained of any discomfort through a hand-held alarm. Before the functional session, the subjects were asked to stay awake and focus on the cross on the screen, without actively moving and thinking. The scanning sequence was as follows: (i) Structural imaging, matrix size = 208*300*320 slices, 0.8 mm3 isotropic voxels, slice gap = 0 mm, repetition time = 2500 ms, echo time = 2.22 ms, flip angle = 8°; (ii) Functional imaging, matrix size = 104*104*72 slices, 2.0 mm3 isotropic voxels, slice gap = 0 mm, repetition time = 800 ms, echo time = 37 ms, flip angle = 52°, number of acquisitions = 460, ascending interleaved acquisition of axial slices.
Results
The subregion of vermis IV/V survived the multiple comparison correction to reveal a lower VBM value in patients than in healthy controls (Cohen’s d = -0.968). The patients also showed significantly higher fALFF (Cohen’s d = 0.666) in this subregion. After controlling the demographic features, the proprioceptive scores were significantly correlated with VBM (r = 0.622) and fALFF values (r = −0.512) in the group of patients.Discussion
The most important findings of this study were: (i) We not only replicated the lower volume but also observed the higher intrinsic activity intensity in subregions of Cerebellar Vermis IV/V of patients with CAI when compared with healthy controls without a history of significant ankle sprains; (ii) we found that the deficits of ankle inversion proprioception in CAI were significantly correlated with the structural and functional features of the vermis.Conclusion
Patients with CAI have lower gray matter volume (VBM values) and a higher intensity of intrinsic activity (fALFF values) in the cerebellar vermis IV/V subregion than patients in healthy controls. More severe proprioception deficits were significantly associated with decreased volume and increased intrinsic activity of the vermis in patients, which indicates that structural degeneration and functional compensation in the vermis might be part of a pathological process in the proprioception deficits of CAI.Acknowledgements
The authors sincerely thank the subjects for their participation and support in this study.References
[1] Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54(6):572–88.[2] Gribble PA, Bleakley CM, Caulfield BM, et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016;50(24):1496-1505.
[3] Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. 2017;51(2):113-125.
[4] Needle AR, Lepley AS, Grooms DR. Central nervous system adaptation after ligamentous injury: a summary of theories, evidence, and clinical interpretation. Sports Med. 2017;47(7):1271–88.
[5] Song Y, Li H, Sun C, et al. Clinical guidelines for the surgical management of chronic lateral ankle instability: a consensus reached by systematic review of the available data. Orthop J Sports Med. 2019;7(9):2325967119873852.
[6] Terada M, Johnson N, Kosik K, Gribble P. Quantifying brain white matter microstructure of people with lateral ankle sprain. Med Sci Sports Exerc. 2019;51(4):640–6.
[7] Guerra-Carrillo B, MacKey AP, Bunge SA. Resting-state fMRI: a window into human brain plasticity. Neuroscientist. 2014;20(5):522–33.
Figures