2278
Fast and large coverage lower extremity perfusion evaluation with dual-echo EPI enabled blood oxygen level dependent technique1Siemens Healthineers, Beijing, China, 2Radiology Department, Beijing Cancer Hospital, Beijing, China, 3Radiology Department, Renji Hospital, Shanghai, China, 4Radiology Department, Peking Union Medical College Hospital, Beijing, China
Synopsis
Keywords: Muscle, Muscle, Perfusion, Reactive Hyperemia, BOLD
Motivation: Lower extremity reactive hyperemia BOLD have been used to evaluate the skeletal muscle perfusion status. The existing methods, such as multi-echo GRE and single-echo EPI, have limitations in terms of spatial coverage and signal quantification.
Goal(s): The study aims to apply dual-echo multi-band EPI to achieve high temporal and spatial resolution, and large coverage in BOLD experiment.
Approach: The study applied dual-echo EPI to sample the T2* along the reactive hyperemia experiment. Images at TE of zero were synthesized to investigate the intrinsic signal change.
Results: The proposed method can provide semi-quantitative indicators of the perfusion status of the lower extremity skeletal muscle.
Impact: This work demonstrates the advantages of dual echo EPI acquisition for lower extremity reactive hyperemia experiments. Compared to the commonly used acquisition strategies, the proposed one can be used to enhance the quality and efficiency of lower extremity perfusion imaging.
Introduction
Perfusion evaluation of the lower limbs skeletal muscle at resting state is challenging due to its intrinsic low perfusion level. Reactive hyperemia technique, also termed lower extremity blood oxygen level dependent (BOLD), has been widely used in clinical research to provoke measurable perfusion changes1,2. Multi-echo gradient echo (GRE) is commonly used to sample the T2* changes. However, this method has limitations such as reduced temporal resolution and limited coverage to one slice. Previously, we’ve used single echo echo-planer imaging (EPI) to increase both the coverage and the temporal resolution3. However, this method can only measure the change of R2*, instead of the absolute T2* value, which was more commonly used in BOLD experiment. Besides, the single echo EPI approach cannot account for the potential proton density and T1 changes during the BOLD experiment. This study aims to apply multi-band dual-echo EPI in the lower extremity BOLD experiment and perform a semi-quantitative analysis to evaluate the perfusion status of the lower extremity muscle.Methods
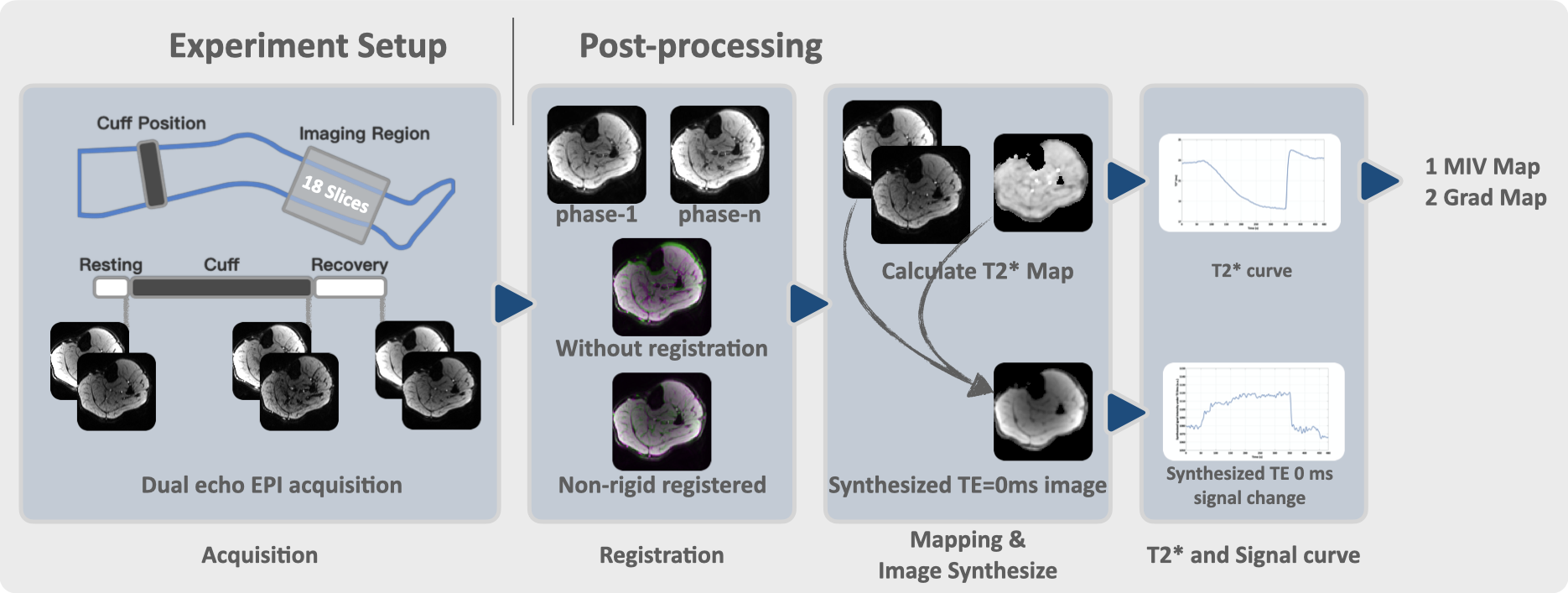
Two subjects were recruited, with informed consent acquired before the study. The experiment was performed on a 3.0T whole body scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) equipped with an 18-channel knee coil. The lower extremity BOLD experiments followed the previously developed workflow, consisting of a 60-second resting session, a 300-second cuff-induced hyperemia session, and 120-second recovery session with the pressure released. The subjects’ position and experiment setting were the same as in our previous study3. The experiment used dual-echo EPI to sample the dynamic process (CMRR Multi-band accelerated EPI prototype sequence)4, with the following parameters: echo time (TE) 11.40ms and 30.26ms, repetition time 1 second, field of view 154x154mm2, base resolution 96x96, slice thickness 8mm, 18 slices acquired without slice gap, partial Fourier 6/8, acceleration factor in phase direction 3, multi-band acceleration factor 2, flip angle 40 degrees. The echo time was the minimum allowed time. Flow compensation was used. To reduce the influence of inflow blood, a parallel saturation band of 50 mm thickness was placed at the inflow side of the imaging region with 10 mm gap. The post-processing pipeline was shown in Figure.1, we used ANTs (Advanced Normalization Tools, version 2.1) for non-rigid registration, which consists of rigid, affine, and non-rigid transformations. The images of each phase were registered to the first phase with the first echo as reference. B-Spline was used for the interpolation. The images of each phase were smoothed with a gaussian kernel of 2.5 mm then to calculate the T2* map. Images with TE of zero were synthesized for each phase to investigate the signal change along the experiment. The minimum ischemia value (MIV) was calculated as the T2* change from the beginning to the end of the ischemia session. The gradient during reactive hyperemia (Grad) was calculated as the T2* change rate over the continuous 10 seconds of the highest slope during the reactive hyperemia session. A pixel-wise MIV and Grad map was generated.Results
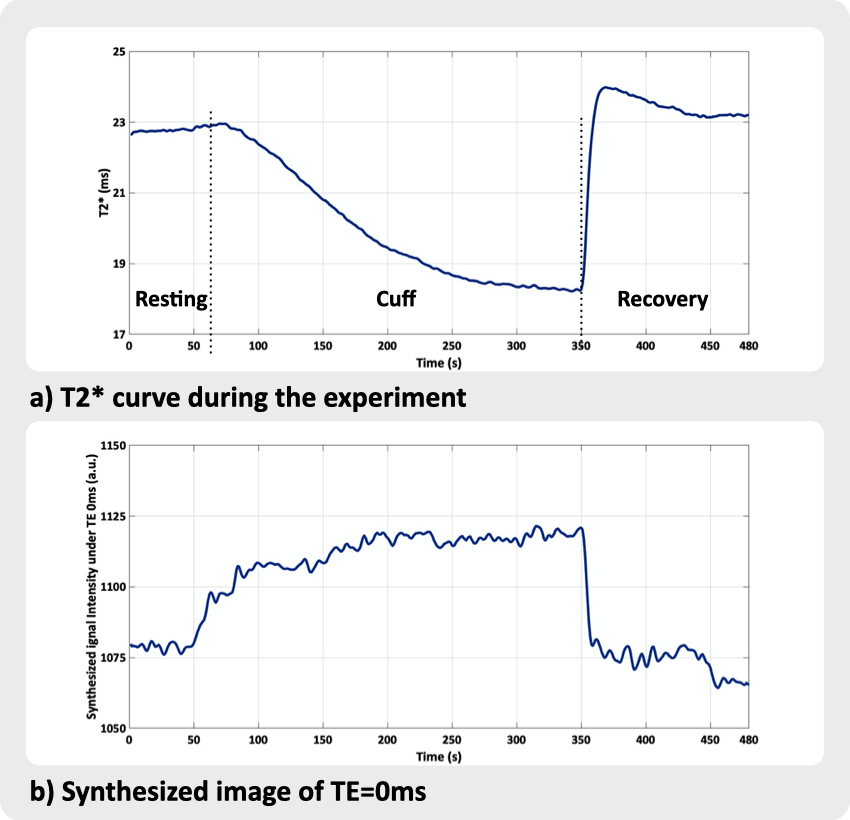
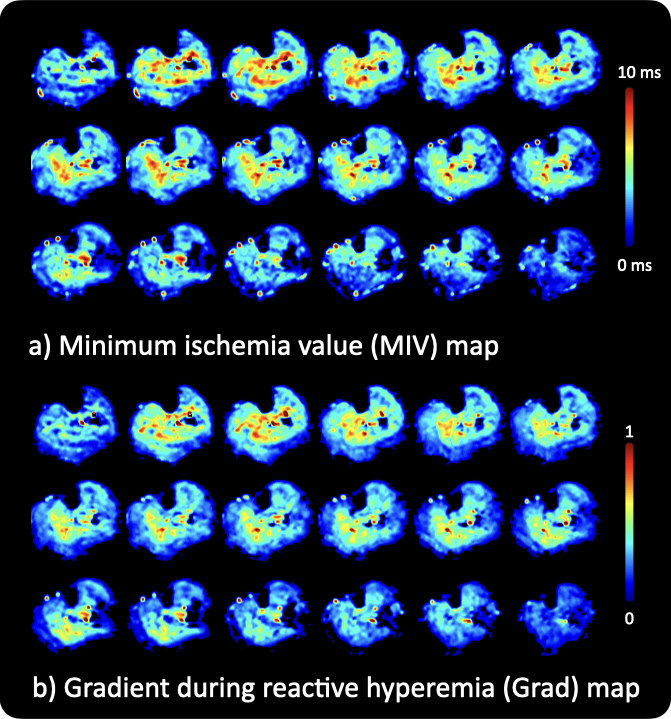
Figure 2 illustrates the T2* change during the experiment. It decreases during the cuff-session and quickly rises back to the baseline during the recovery period. In contrast, during the cuff-session, the synthesized pictures under TE 0ms rose, and during the recovery session, they recovered to the baseline. The MIV and Grad map of the entire volume, which display a distribution according to muscle groups, are displayed in Figure 3. As demonstrated by the comparison in Figure 1, registration markedly lessens deformation throughout the cuff session, making it necessary for this experiment.Discussion and conclusion
This study employed the multi-band dual-echo EPI acquisition in the lower extremity BOLD experiment. Compared to the conventional multi-echo GRE approach, the proposed method achieved much improved coverage, higher temporal resolution, without sacrificing spatial resolution. Compared to the previously developed single echo GRE-EPI approach, the proposed method can measure the more commonly used absolute T2* value, instead of the change of R2*. The synthesized image also revealed the signal intensity changes of certain muscle groups during the cuff-session, which may indicate an accumulation of blood, or hyperemia. Such signal change may bias the changes of R2* in single-echo EPI approach. A small flip angle of 40 degree was used to reduce the influence of T1 changes. The MIV and Grad maps provide a semi-quantitative analysis of the perfusion status of the lower extremity muscle, which can be useful for clinical diagnosis and research. As a limitation, only healthy subjects were included. Subjects with altered perfusion status needs to be recruited to further explore the feasibility of the proposed technique.Acknowledgements
No acknowledgement found.References
[1] Shiteng Suo, et al. Evaluation of skeletal muscle microvascular perfusion of lower extremities by cardiovascular magnetic resonance arterial spin labeling, blood oxygenation level dependent, and intravoxel incoherent motion techniques, JCMR, 2018
[2] Xiaoxi Yu, et al. Blood Oxygen Level-Dependent MR Imaging of Lower Extremities in Peripheral Artery Disease and Its Correlation With Walking Performance, JMRI, 2023
[3] Jianxun Qu, et al., Large coverage, high temporal and spatial resolution lower extremity blood oxygen level dependent imaging, ISMRM, 2023
[4] https://www.cmrr.umn.edu/multiband
Figures