2277
Multi-vendor Multi-site accelerated high-resolution T1ρ mapping with retrospective and prospective compressed sensing reconstruction1Program of Advanced Musculoskeletal Imaging (PAMI), Cleveland Clinic, Cleveland, OH, United States, 2Department of Biomedical Engineering, Lerner Research Institute, Cleveland Clinic, Cleveland, OH, United States, 3Department of Biomedical Engineering, Case Western Reserve University, Cleveland, OH, United States, 4Department Electrical, Computer, and Systems Engineering, Case Western Reserve University, Cleveland, OH, United States, 5Department of Electrical Engineering, University at Buffalo, Buffalo, NY, United States, 6Department of Diagnostic Radiology, Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 7Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 8Department of Radiology, Albert Einstein College of Medicine, Bronx, NY, United States, 9Department of Radiology, University of Kentucky, Lexington, KY, United States, 10Department of Biomedical Engineering, University at Buffalo, Buffalo, OH, United States
Synopsis
Keywords: Cartilage, MSK
Motivation: High-resolution T1ρ mapping is desired to improve the early diagnosis of diseases such as osteoarthritis; however, it suffers from long acquisition times.
Goal(s): To accelerate high-resolution T1ρ mapping using compressed-sensing reconstruction in a multi-site multi-vendor setting.
Approach: We standardized the T1ρ imaging protocol between three sites using three MR platforms (GE/Philips/Siemens). Accelerated high-resolution T1ρ mapping with accelerator factors (AF) ranging 8-12 were performed using both retrospective and prospective downsamplings with compressed-sensing reconstruction.
Results: The coefficients-of-variation between reference and accelerated maps were <5% for all sites. Reliable high-resolution T1ρ mapping of the whole knee can be acquired within 7 mins.
Impact: Standardization of the acquisition and reconstruction of accelerated high-resolution T1ρ mapping across sites and MR platforms will greatly facilitate its future use in clinical trials and clinical practice, significantly improving diagnosis and evaluation of responses to interventions/treatments for OA.
Introduction
Osteoarthritis (OA) is a joint disorder that is characterized by the degeneration of cartilage and other tissues1. To improve early detection and prevention of this disease, quantitative MRI techniques, such as T1ρ mapping, have been suggested as biomarkers to quantify changes of the cartilage extracellular matrix, which happens at the early stages of OA2. Currently, T1ρ mapping is limited to relatively low resolution (e.g., slice thickness of 3-4 is commonly used), which is prone to partial voluming averaging effects, and has limited sensitivity of detecting small lesions. High-resolution T1ρ mapping is desired but suffers from prohibitively long acquisition time. Previously, we showed the feasibility of accelerated high-resolution T1ρ mapping using compressed sensing (CS) reconstruction in a single-site study3. No studies have yet performed and evaluated accelerated high-resolution T1ρ mapping in a multi-vendor multi-site setting, which is critical for the clinical translation of such advanced techniques. Therefore, the goal of this study was to evaluate the accelerated high-resolution T1ρ mapping of the whole knee across multiple sites and multiple MR platforms using CS reconstruction with both retrospective and prospective downsamplings.Method
Data AcquisitionA total of six volunteers were scanned at three sites: three at Site 1 (2 males, 38.7±17.2 years; PrismaFit Siemens Healthineers, 1Tx/15Rx QED knee coil); one at Site 2 (Female, 41 years; SIGNA Premier, GE HealthCare,1Tx/18Rx QED knee coil); two at Site 3 (2 males, age 48.5±16.3 years, Ingenia, Philips Healthcare, 1Tx/16Rx InVivo knee coil).
T1ρ high-resolution images were acquired using 3D MAPSS4,5 sequence with FOV 140x140x96 mm3, imaging matrix 384x192x60, resolution 0.36x0.73x1.6 mm3, spin lock frequency(SLF) 500Hz, and time of spin lock (TSL) 0/8/16/24/32/40/48/56 ms. The reference imaging was collected using GRAPPA with AF 2, while the prospectively undersampled accelerated imaging was collected using acceleration factor (AF) 8 to 12. Morphological imaging was acquired using DESS (Siemens)/MENSA (GE)/SPGR(Philips) with FOV 140x140x112mm3, resolution 0.36x0.4x0.7 mm3.
Data Reconstruction
T1ρ high-resolution reference was reconstructed using GRAPPA reconstruction and coil sensitivity maps were calculated to combine multi-channel images. The reference was retrospectively undersampled with AF 8 to 12. The CS reconstruction was applied to both retrospective and prospective datasets using spatiotemporal finite difference transform (SFTD) 6.
Data Processing and Evaluation
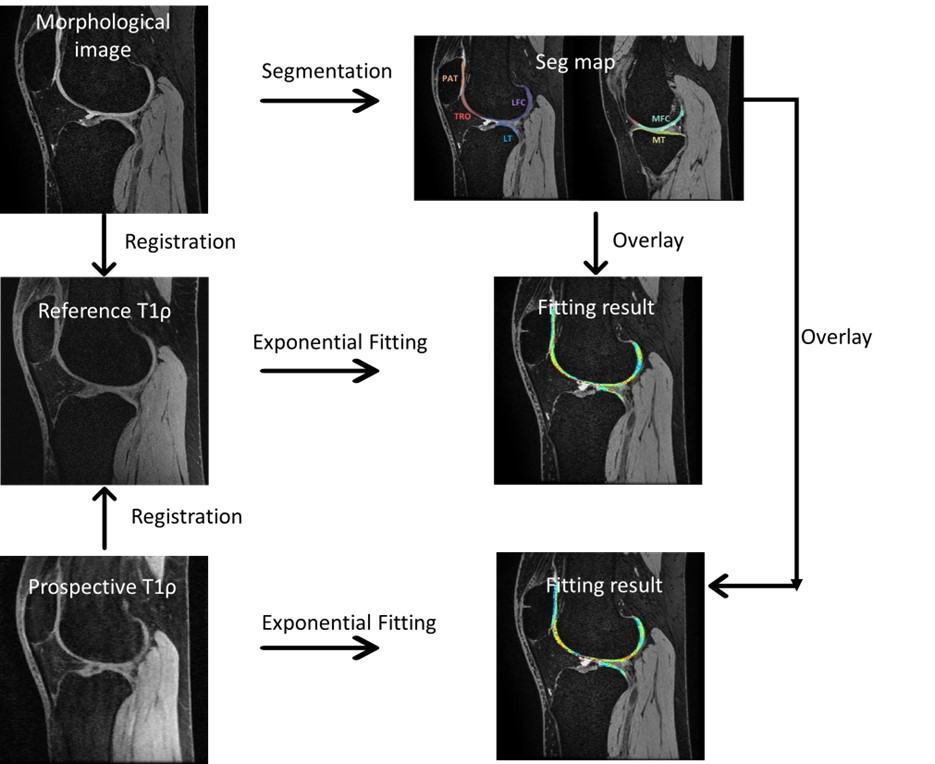
The workflow for data processing is shown in Figure 1. The DESS/MENSA/SPGR images were registered to the first echo of the T1ρ reference scan. Cartilage was segmented into six compartments in the registered DESS/MENSA/SPGR images and the segmentation ROIs were overlaid to T1ρ maps. T1ρ maps were generated with pixel-wise mono-exponential decay fitting using nonlinear least square. Mean and SD of T1ρ values were calculated for each compartment. Coefficients of variation (CVs) between reference and accelerated T1ρ maps were calculated.
Result
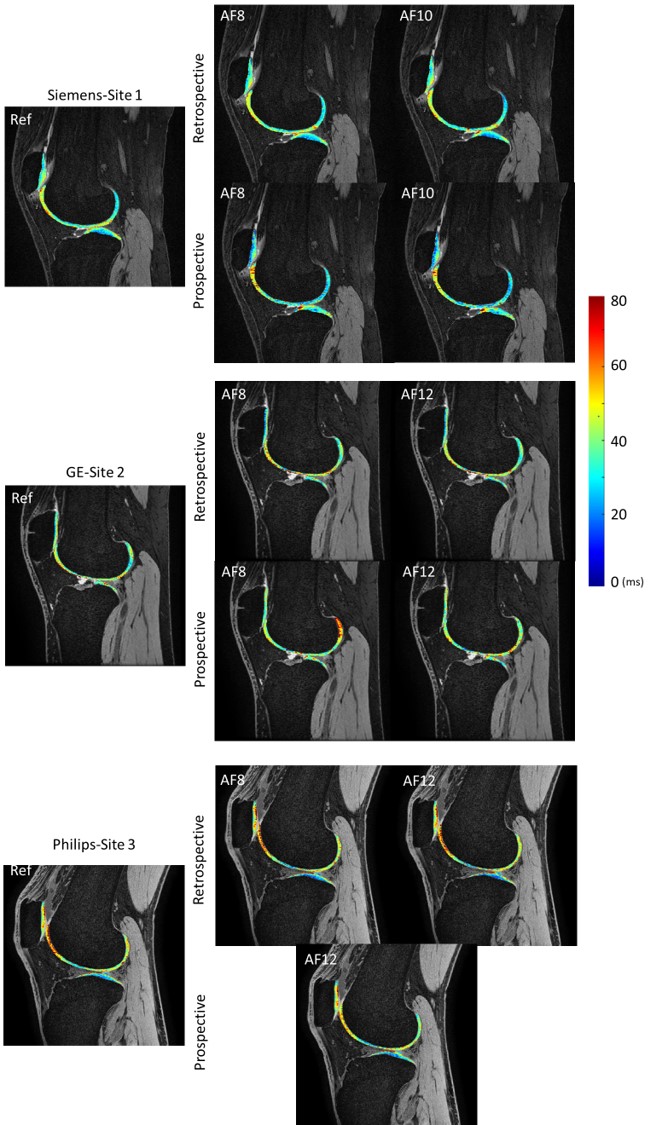
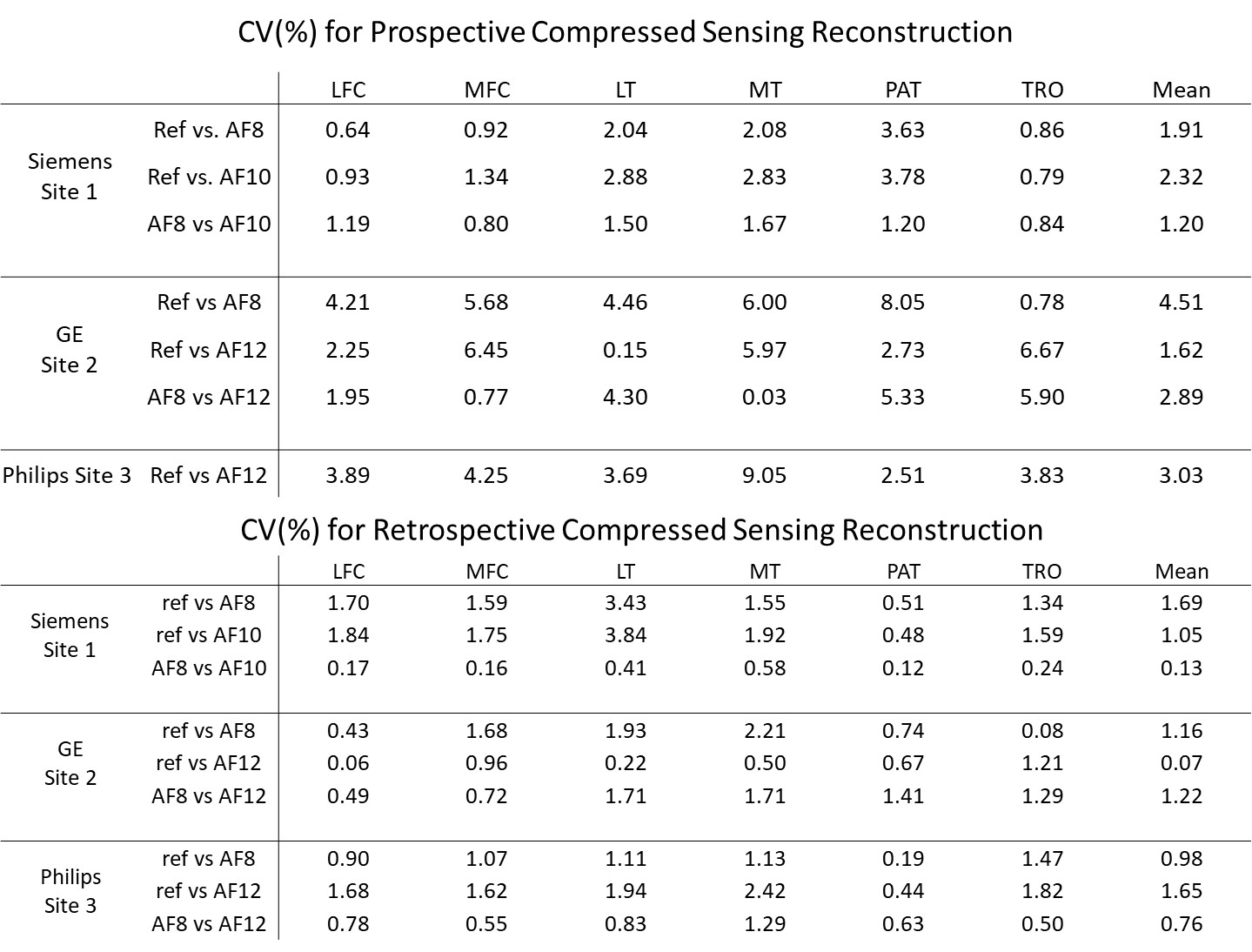
Tables 1 and 2 show means(SDs) and CVs of each site between reference and accelerated T1ρ maps. All sites showed excellent agreement between reference and accelerated maps with retrospective downsamplings. The average CVs were < 2% for all AFs and all sites. The CVs were slightly higher with prospective downsampling, and the average CVs were < 5% for all AFs for Sites all sites. Site 3 only collected prospective AF12 data and the data collection is ongoing. Figure 2 shows an example of accelerated high-resolution T1ρ maps with retrospective and prospective downsamplings, respectively.Discussion
The results of the present study suggested the feasibility of reliably collecting accelerated high-resolution(0.36x0.73x1.6mm3) T1ρ maps of the whole knee within 7 minutes. The accelerated maps with CS reconstruction shows the benefits of reducing acquisition time while preserving quantitative accuracy. In this study, the protocol was standardized and performed in three sites with different MR platforms. All sites show promising results of CV ≤ 2% for retrospective results and of CV ≤ 5% for prospective results. The discrepancy when comparing retrospective and prospective results may be due to patient movement during the scan, or registration error. In particular, patellar cartilage showed the largest CV (8%) with prospective downsampling, which may be most prone to motion between scans. We are currently collecting more data from all sites. Furthermore, we plan to scan traveling volunteers who will travel and be scanned at all sites to evaluate the inter-vendor inter-site variations from the sameConclusion
We showed promising results of reliable accelerated high-resolution T1ρ mapping with CS reconstruction at different sites with different MR platforms. Standardization of the acquisition and reconstruction of accelerated high-resolution T1ρ mapping across sites and MR platforms will greatly facilitate its future use in clinical trials and clinical practice. Reliable fast high-resolution T1ρ mapping will significantly improve diagnosis and evaluation of responses to interventions/treatments for OA.Acknowledgements
The study was supported by NIH/NIAMS R01AR077452.References
- Martel-Pelletier, J., Barr, A., Cicuttini, F. et al. Osteoarthritis. Nat Rev Dis Primers 2, 16072 (2016).
- MacKay JW, Low SBL, Smith TO, Toms AP, McCaskie AW, Gilbert FJ. Systematic review and meta-analysis of the reliability and discriminative validity of cartilage compositional MRI in knee osteoarthritis. Osteoarthritis Cartilage. 2018;26(9):1140-52.
- Kim, J et al. Retrospective and prospective accelerated T1ρ/T2 mapping with Compressed Sensing: high resolution T1ρ mapping and simultaneous T1ρ/T2 mapping. ISMRM 2023
- Li X, Han ET, Busse RF, Majumdar S. In vivo T(1rho) mapping in cartilage using 3D magnetization-prepared angle-modulated partitioned k-space spoiled gradient echo snapshots (3D MAPSS). Magnetic resonance in medicine. 2008;59(2):298-307. Epub 2008/01/30.
- Kim J, Mamoto K, Lartey R, et al. Multi-vendor multi-site T1ρ and T2 quantification of knee cartilage. Osteoarthritis Cartilage. 2020;28(12):1539-1550.
- Zibetti MVW, Sharafi A, Otazo R, Regatte RR. Accelerating 3D- T1ρ mapping of cartilage using compressed sensing with different sparse and low rank models. Magnetic resonance in medicine. 2018;80(4):1475-91. Epub 2018/02/27.
Figures