2274
Accelerating acquisition of readout-segmented echo planar imaging with a simultaneous multi-slice technique for diagnosing knee lesions1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China, 3MR Collaborations, Siemens Healthineers Ltd., Shanghai, China
Synopsis
Keywords: Whole Joint, Joints
Motivation: knee injury is common in clinical practice. DTI enables quantitative assessment of tissue changes in pathological joints, but its clinical application is limited due to prolonged scan time.
Goal(s): This study aims to explore the feasibility of using SMS technique in RESOLVE- DTI in knee joint to reduce acquisition time without compromising image quality.
Approach: There protocols, Conventional RESOLVE-DTI with 12 directions, and SMS-RESOLVE-DTI with 12 and 20 directions, were used to fully assess the image quality and quantitative parameters.
Results: The use of SMS technique greatly reduced the acquisition time without compromise image quality and quantitative evaluation accuracy.
Impact: The SMS technique greatly shortens the acquisition time of RESOLVE-DTI and provides similar image quality, allowing clinical doctors to simultaneously evaluate cartilage and ligaments of the knee joint in one scan. SMS-RESOLVE-DTI has high clinical application potential.
INTRODUCTION
The knee is the most frequently involved in joint trauma and arthritis diseases, which affects all the tissues of the synovial joint, including cartilage, bone, ligament, and so on. A recent advancement in DTI, known as readout segmentation of long variable echo trains (RESOLVE), has shown promising clinical applications in quantitative assessing tissue changes in pathological joints. RESOLVE-DTI could enhance image quality and spatial resolution but with extended scanning time[1], which limited its clinical application. The Simultaneous multi-slice (SMS) with blipped-controlled aliasing in parallel imaging could accelerate MR imaging by exciting and reading out multiple slices simultaneously[2], which greatly shortened the acquisition time of RESOLVE-DTI, making its clinical application possible.METHODS
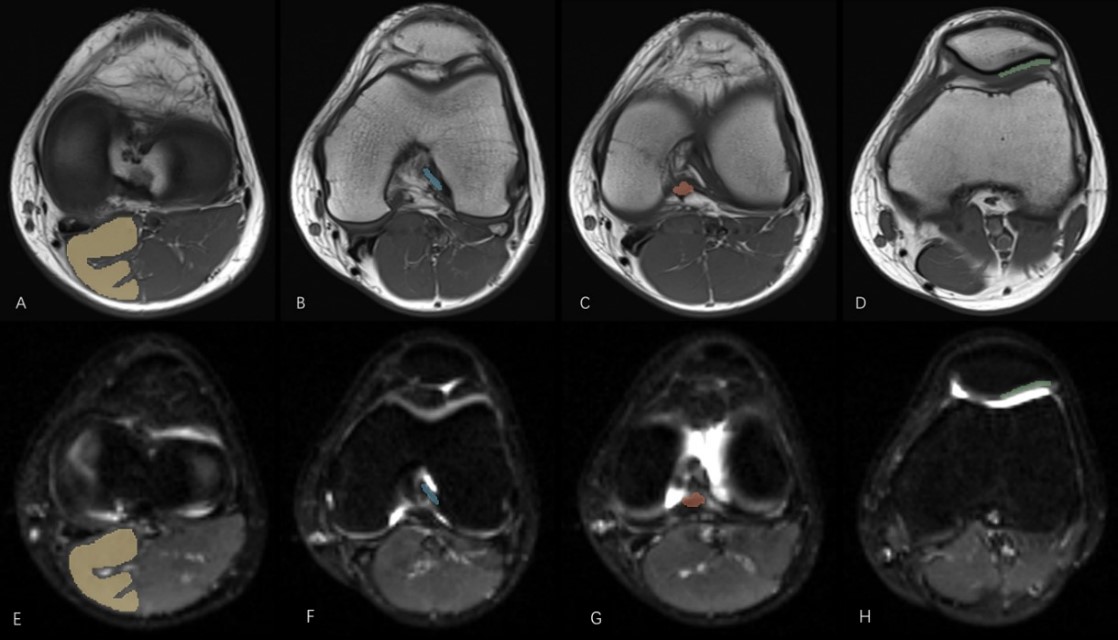
Our study enrolled 23 acute knee injuries patients within 3 weeks (12 cases with complete ACL tear and 16 cases with acute cartilage injury) and 30 healthy volunteers. MRI of all subjects were using a 3-T imaging System with a dedicated 16-channel knee coil. Besides the conventional T1 and T2-weighted imaging, there DTI protocols were used, Conventional RESOLVE-DTI with 12 directions (Protocol 1), SMS-RESOLVE-DTI with 12 directions (Protocol 2) and 20 directions (Protocol 3). The above-mentioned three Protocols were performed on healthy volunteers to evaluate the feasibility of the SMS technique, subsequently, Protocols 1 and 2 were applied on knee injured patients . The SNR and CNR of the gastrocnemius, ACL, PCL, and PC for healthy volunteers were calculated among the above-mentioned three different sequences. DTI parameters of Gastrocnemius, anterior and posterior cruciate ligament and patellar cartilage from three protocols were measured and assessed (Figure 1).RESULT
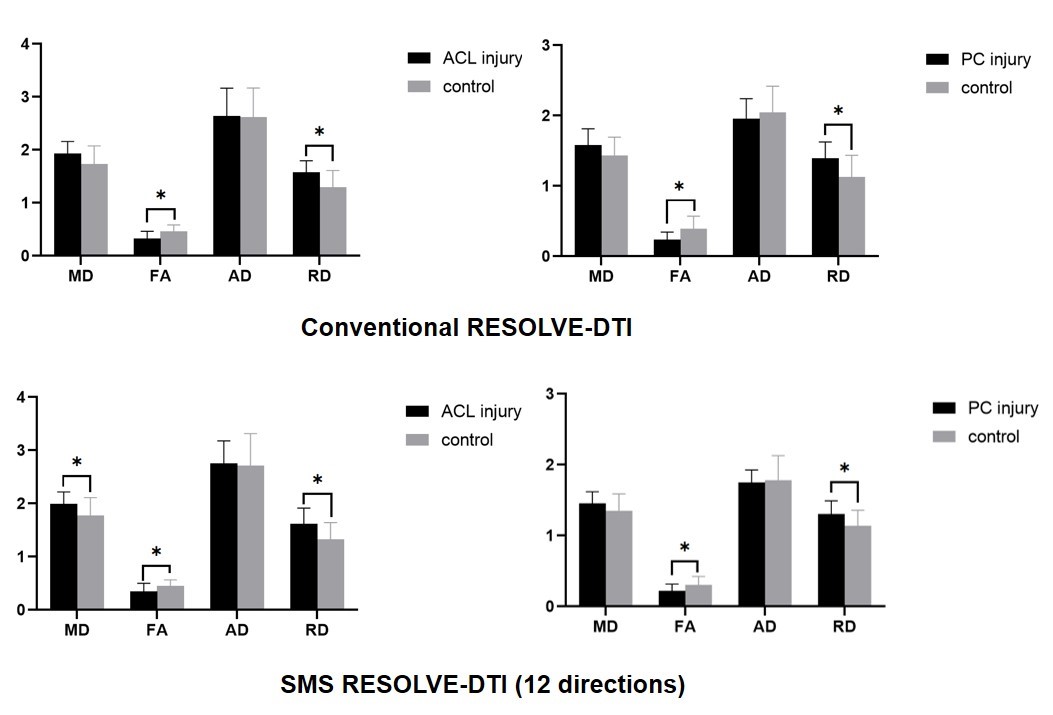
The utilization of Protocol 2 was reduced acquisition time by 38.6% and 34.2% compared with Protocol 1 and 3 while maintaining similar SNR and CNR (P > 0.05). For healthy volunteers, except for AD and FA value of PC (P = 0.005, P = 0.046), all other DTI-derived parameters values for gastrocnemius, ACL, PCL and PC in healthy volunteers showed no significant difference between Protocol 1 and 2. Parameters of all tissues showed no statistically significant between Protocol 2 and 3. For injured ACL and PC group, basically all parameters showed no significant difference between Protocol 1 and Protocol 2 except the AD in PC injured group(P = 0.025). Compared with volunteers, significantly lower FA, and higher RD of Protocol 1 and 2 for injured ACL were respectively demonstrated (P < 0.05). The statistically lower FA and higher RD (P < 0.05) of Protocol 1 and 2 for injured PC were respectively demonstrated (Figure 2).DISCUSSION
The use of SMS technique significantly reduced acquisition time without compromises the SNR and CNR of MR image nor statistically change diffusive parameters for gastrocnemius and ligament. But for PC, FA and AD value of SMS-RESOLVE-DTI were lower than those of RESOLVE-DTI. This result might be caused by two reasons. First, shorter TR used in SMS-RESOLVE-DTI might cause T1effect and decreased SNR in long T1 tissue, which may affect AD and RD, especially AD [3,4,5]. Second, knee joint is an intricate structure that may cause inhomogeneity in the magnetic field (B0) field that could lead to susceptibility artifacts, meanwhile the use of SPAIR technique in three DTI techniques, which is sensitive to B0 inhomogeneities and may cause the partial loss of water signal[6], may influence quantitative measurements of diffusion parameters. We found that the diffusive parameters of the target different tissues were not different between the 12-direction and 20-direction SMS-RESOLVE-DTI protocol. Considering the balance between scanning time and imaging quality, we believe that the 12-direction SMS-RESOLVE-DTI protocol is perfectly suitable for different tissue of knee in clinical application. In cases of injured PC and ACL, both SMS-RESOLVE-DTI and RESOLVE-DTI protocol showed the decreased FA value and increased RD value when compare with healthy volunteers. These findings demonstrated SMS-RESOLVE-DTI with 12-direction and the conventional RESOLVE-DTI with 12-direction have similar diagnostic capabilities. SMS technique showed promise as a potential quantitative assessment tool for evaluating damaged ACL and knee cartilage.Conclusion
The 12-directions SMS-RESOLVE-DTI shows the best balance between acquisition time and highly reliable image quality. It has great promise as an alternative technique to conventional DTI for assessing injured ligament and cartilage.Acknowledgements
No acknowledgement found.References
1.Drake-Perez M, Boto J, Fitsiori A, Lovblad K, Vargas MI. Clinical applications of diffusion weighted imaging in neuroradiology. Insights Imaging 2018;9:535-547https://doi.org/10.1007/s13244-018-0624-3
2. Fritz J, Fritz B, Zhang J, Thawait GK, Joshi DH, Pan L, et al. Simultaneous Multislice Accelerated Turbo Spin Echo Magnetic Resonance Imaging: Comparison and Combination With In-Plane Parallel Imaging Acceleration for High-Resolution Magnetic Resonance Imaging of the Knee. Invest Radiol 2017;52:529-537https://doi.org/10.1097/RLI.0000000000000376
3.Bernstein AS, Chen NK, Trouard TP. Bootstrap analysis of diffusion tensor and mean apparent propagator parameters derived from multiband diffusion MRI. Magn Reson Med 2019;82:1796-1803https://doi.org/10.1002/mrm.27833
4.Song SE, Woo OH, Cho KR, Seo BK, Son YH, Grimm R, et al. Simultaneous Multislice Readout-Segmented Echo Planar Imaging for Diffusion-Weighted MRI in Patients With Invasive Breast Cancers. J Magn Reson Imaging 2021;53:1108-1115https://doi.org/10.1002/jmri.27433
5.Setsompop K, Gagoski BA, Polimeni JR, Witzel T, Wedeen VJ, Wald LL. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med 2012;67:1210-1224https://doi.org/10.1002/mrm.23097
6.Klupp E, Cervantes B, Schlaeger S, Inhuber S, Kreuzpointer F, Schwirtz A, et al. Paraspinal Muscle DTI Metrics Predict Muscle Strength. J Magn Reson Imaging 2019;50:816-823https://doi.org/10.1002/jmri.26679
Figures