2265
Improved Fat Suppression in 3-D Double-Echo Steady-State Sequence with Water Excitation using an Adapted Dixon Technique1GE HealthCare, Waukesha, WI, United States, 2Department of Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States
Synopsis
Keywords: Neurography, MSK
Motivation: In 3-D double-echo steady-state sequence with water excitation, fat suppression may be incomplete due to system imperfections, such as B0 and B1 inhomogeneity.
Goal(s): This study describes implementing an adapted Dixon reconstruction to further suppress residual fat signal.
Approach: The images between default and proposed reconstructions were compared in 16 patients undergoing routine upper extremity MR neurography.
Results: The preliminary results demonstrated the feasibility of using the proposed reconstruction to remove residual fat signals incompletely suppressed by the water excitation.
Impact: A benefit of the further suppressed fat provided by the proposed reconstruction was the improved depiction of small, yet clinically important peripheral nerves (particularly subcutaneous sensory branches surrounded by fat).
INTRODUCTION
For 3-D double-echo steady-state sequence with water excitation, the first free induction decay (FID) readout provides high quality anatomical detail, and the second time-reversed steady-state free precession (SSFP)-echo readout provides additional T2-weighting. This sequence has demonstrated benefits for 3D MR neurography (MRN) [1,2], but due to system imperfections (namely, B0 and B1 inhomogeneities), the fat signals may not be completely suppressed by the spectral-spatial water excitation. Here we propose an adapted Dixon (aDixon) reconstruction to further suppress residual fat signal in 3-D double-echo steady-state sequence with water excitation.METHOD
When fat signals are incompletely suppressed by the spectral-spatial water excitation, the contribution from the residual fat signals in the two readouts SSFP-FID and SSFP-Echo behave similarly to the fat described in the Dixon technique; therefore, we can adapt a Dixon reconstruction to identify and remove the residual fat signals. A total of 16 patients undergoing routine upper extremity MRN on clinical 3T scanners (Premier, GE Healthcare) were scanned with a clinical 3-D double-echo steady-state sequence with water excitation (0.5x.0.5x1.6mm3, TR/TE1/TE2≈14.8ms/5.3ms/9.5ms, scan time≈5.8minutes), hereby referred to by the acronym Multi-Echo iN Steady-state Acquisition (MENSA). The raw k-space data were retrospectively analyzed, with the default reconstructed images from MENSA compared against that from the proposed aDixon reconstruction. A research assistant with 2-years segmentation experience obtained regions of interests in normal appearing muscle (without muscle edema or fatty infiltration), abnormal muscle as determined by EMG, and in nearby subcutaneous fat. The fat-to-normal-muscle contrast and abnormal-muscle-to-normal-muscle contrast was obtained as the ratio between the corresponding signals. A non-parametric Wilcoxon signed rank test was used to compare the contrasts between conventional reconstruction and aDixon, with p<0.05 deemed statistically significant.RESULT
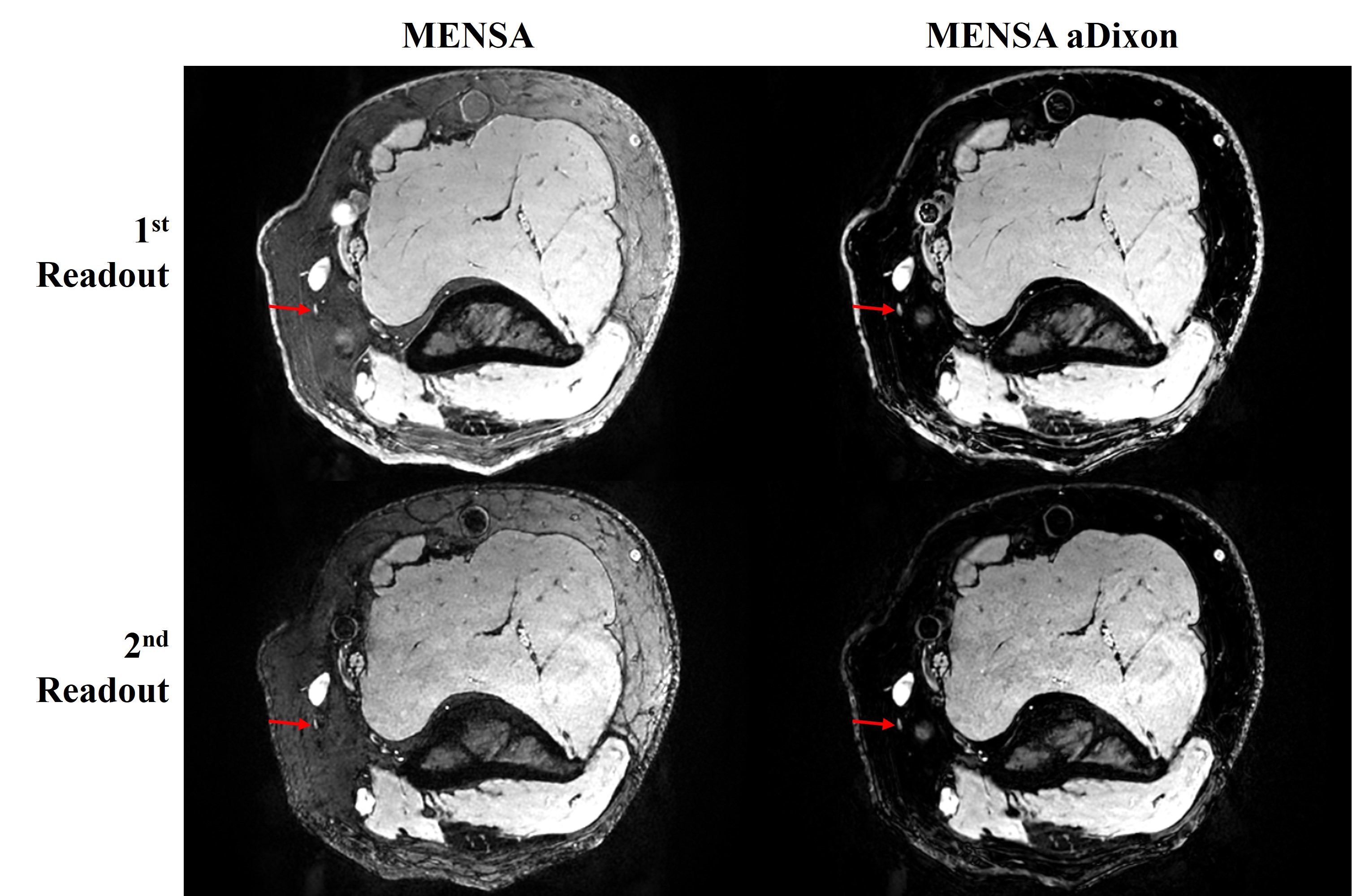
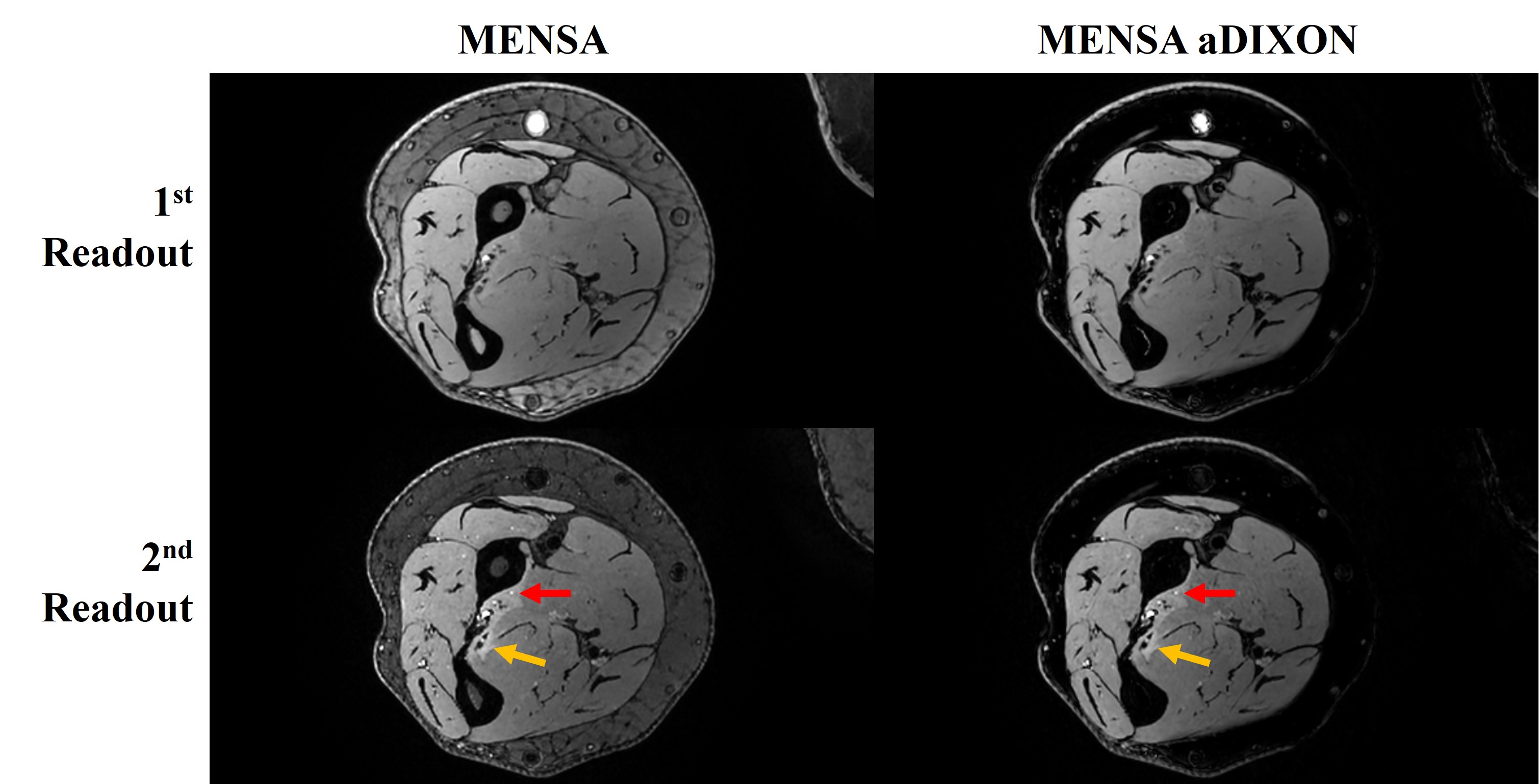
As shown in Figure 1A, compared to MENSA with default reconstruction, the average contrast between subcutaneous fat and normal muscle in MENSA aDixon was 52% lower in 1st readout (p=0.010), and 56% lower in 2nd readout (p<0.001). Figure 1B showed that no significant change in the average contrast between abnormal muscle and normal muscle was observed in MENSA aDixon for both the 1st readout (1.116 vs 1.105, p=0.94) and 2nd readout (1.298 vs 1.296, p=0.99).Figure 2 shows, in a representative case, the images of MENSA from product reconstruction and MENSA from aDixon reconstruction. The medial antebrachial cutaneous nerve surrounded by fat is better depicted after the fat signals were further suppressed in MENSA aDixon (red arrows). Figure 3 shows another representative case demonstrating the improved fat suppression in MENSA aDixon over conventional MENSA, without altering the relative signal levels of the muscle edema to the unaffected, surrounding musculature.
DISCUSSION
These preliminary results demonstrated the feasibility of using aDixon reconstruction to remove residual fat signals incompletely suppressed by the water excitation in the MENSA sequence. The comparison in contrast between subcutaneous fat and normal muscle showed that the residual fat signals were significantly reduced using the proposed reconstruction. A benefit of the further suppressed fat was the improved depiction of small, yet clinically important peripheral nerves (particularly subcutaneous sensory branches surrounded by fat). The lack of significant change in muscle contrast from MENSA aDixon suggests that the reconstruction does not adversely affect the abnormal muscle contrast.The limitations of this study included the lack of qualitative assessment of image quality to determine the conspicuity of nerves and muscle. We plan to enroll more patients prior to making this qualitative comparison. Additionally, we plan to analyze the robustness of the aDixon method in the lumbosacral plexus, and in the neck.
CONCLUSION
An adapted Dixon reconstruction can be adapted to MENSA to further remove residual fat signals incompletely suppressed by the water excitation for evaluation of peripheral nerves in MR neurography exams.Acknowledgements
No acknowledgement found.References
1. Qin Y, Zhang J, Li P, Wang Y. 3D double-echo steady-state with water excitation MR imaging of the intraparotid facial nerve at 1.5T: a pilot study. AJNR Am J Neuroradiol. 2011 Aug;32(7):1167-72. doi: 10.3174/ajnr.A2480. Epub 2011 May 12. PMID: 21566007; PMCID: PMC7966035.
2. Kwon D, Lee C, Chae Y, Kwon IJ, Kim SM, Lee JH. Clinical validation of the 3-dimensional double-echo steady-state with water excitation sequence of MR neurography for preoperative facial and lingual nerve identification. Imaging Sci Dent. 2022 Sep;52(3):259-266. doi: 10.5624/isd.20220035. Epub 2022 May 13. PMID: 36238701; PMCID: PMC9530289.
Figures
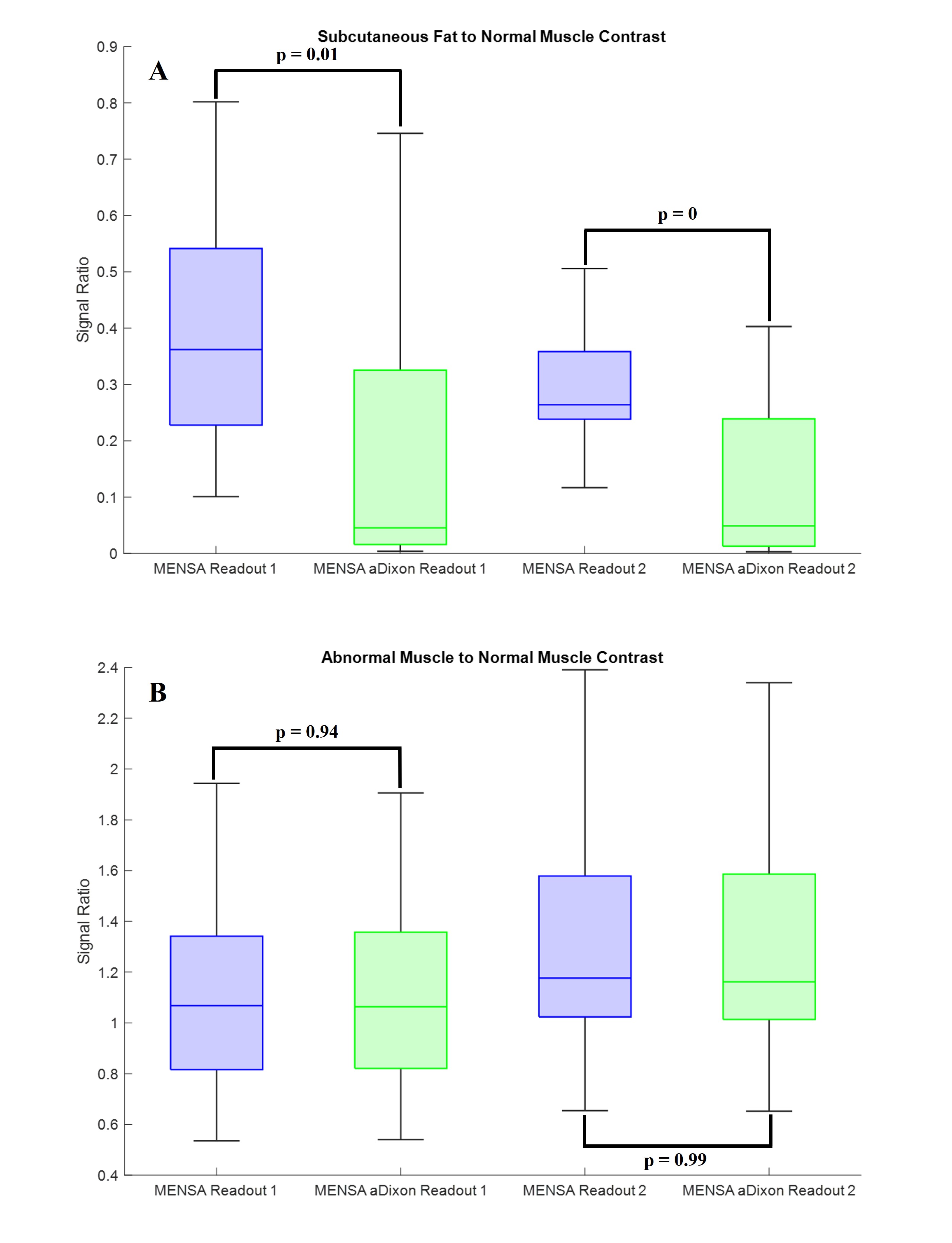
Figure 1 Comparison between MENSA with default reconstruction and MENSA with aDixon reconstruction by measuring A) fat-to-normal-muscle contrast, and B) abnormal-muscle-to-normal-muscle contrast.