2264
Knee Cartilage T2 Associates with Foot and Ankle Posture1Orthopaedic Surgery, Stanford Univesity, Stanford, CA, United States, 2Joint Preservation Center, Palo Alto Veterans Healthcare System, Palo Alto, CA, United States
Synopsis
Keywords: Cartilage, Cartilage, ankle, kinematics, eversion
Motivation: Flat-footedness and pronated ankle posture have been observed in patients with knee osteoarthritis.
Goal(s): This works seeks to determine if compositional changes to cartilage assessed from T2 relaxation times are associated with foot and ankle posture.
Approach: Foot center of pressure, ankle eversion and tibial rotation were compared to tibiofemoral cartilage T2 in 24 participants with healthy knees.
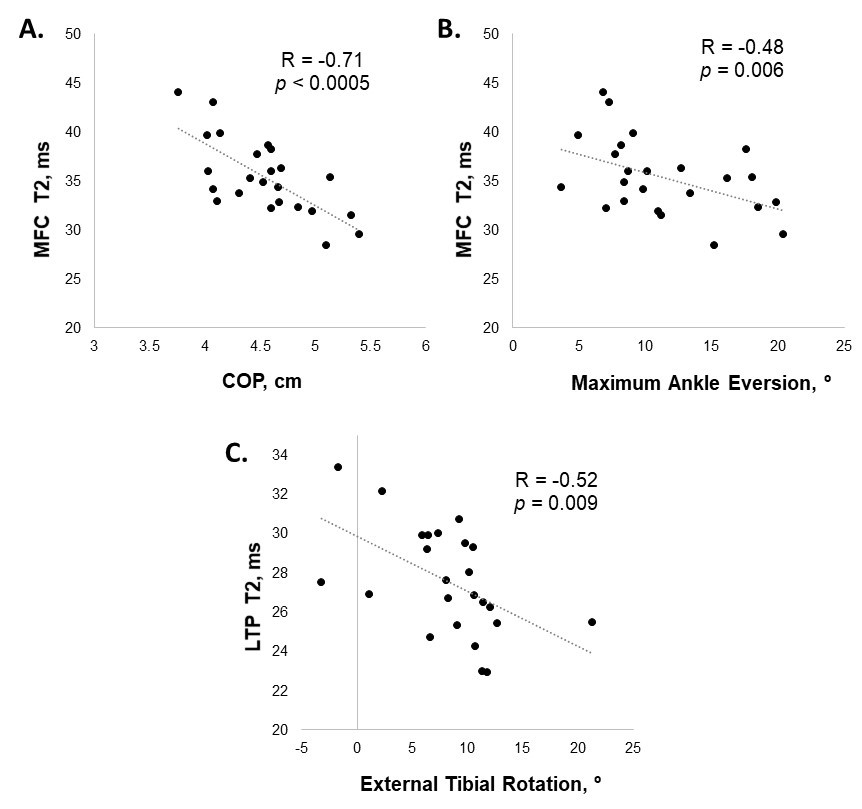
Results: Lower medial femoral cartilage T2 correlated to more medial foot center of pressure and greater ankle eversion (R=-0.71, p<0.0005; R=-0.54, p=0.006; respectively). Higher lateral tibial T2 correlated to more internal tibial rotation (R=-0.52, p=0.009).
Impact: Correlation of foot and ankle posture to cartilage composition at the knee suggest that gait or shoe interventions to appropriately alter weight distribution at the foot and ankle could be utilized to benefit to knee cartilage health.
INTRODUCTION
Planus foot morphology (“flat-footedness”) and pronated ankle posture have been observed in patients with knee osteoarthritis (OA)1,2. Flat-footedness and ankle eversion are thought to influence the knee by coupling with the tibia, where subtalar joint pronation causes internal tibial rotation3 placing rotational stresses on knee cartilage, especially in the medial tibiofemoral (TF) joint4. Previous MRI detection of gross medial TF cartilage damage, including at least partial-thickness defects, were shown to associate with flat-footedness in older adults4. The question arises whether more subtle compositional changes to cartilage, assessed from T2 relaxation times5 in participants without clinical OA, are likewise associated with foot and ankle posture. This study tests the hypotheses that medial foot center of pressure, ankle eversion, and tibial rotation associate with tibiofemoral cartilage T2.METHODS
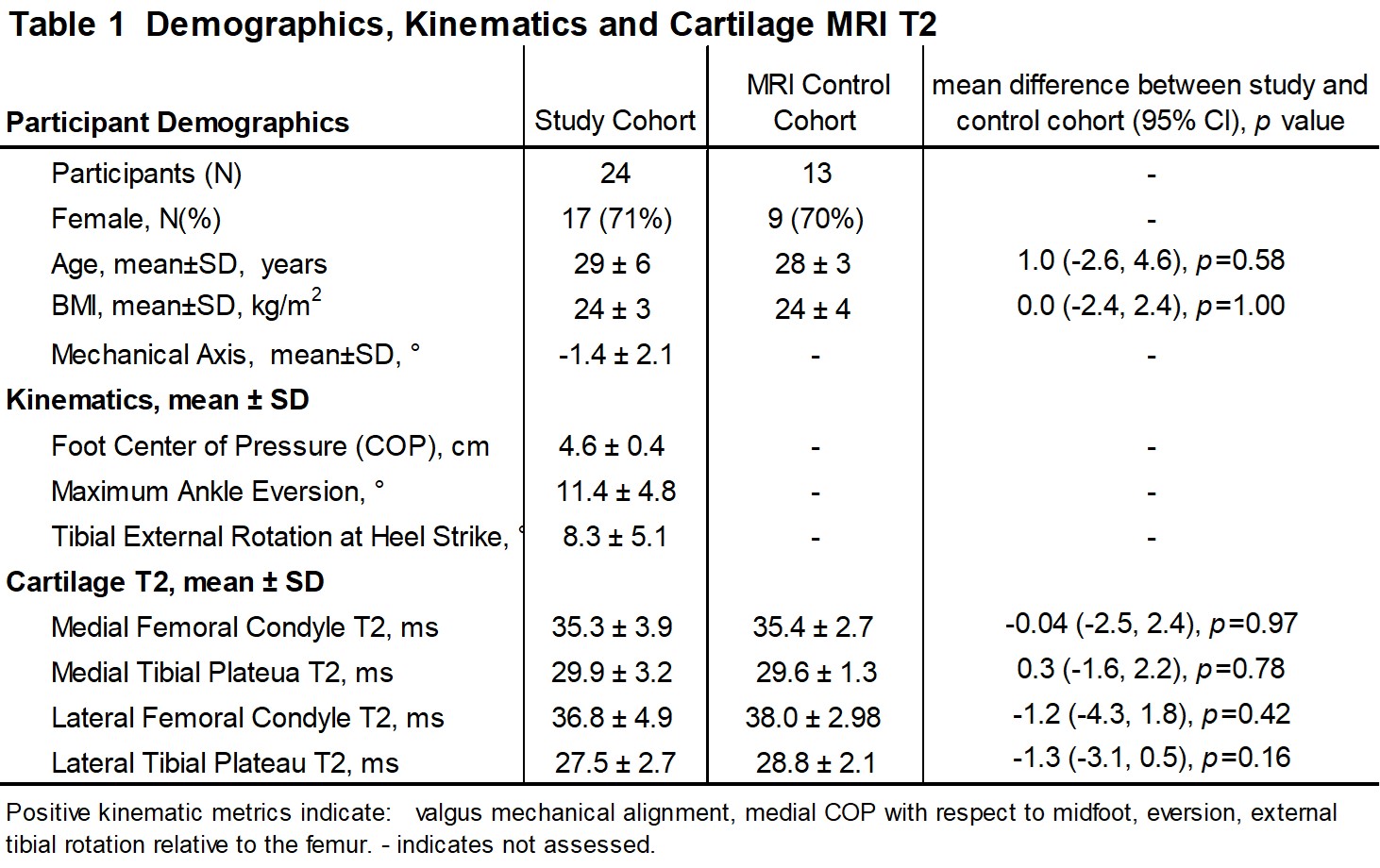
The study cohort comprised 24 participants with 3T knee MRI (GE Healthcare) showing grossly intact cartilage, lower limb radiographs and gait assessments acquired 2 years after unilateral ACL reconstruction, Table 1. MRI, x-ray, COP and gait data from only the uninjured limbs of the study cohort were assessed. To further demonstrate pre-OA status, MRI of the uninjured limbs were evaluated against a healthy control group, Table 1.A 10-camera optoelectronic system (Qualisys) and force plate (Bertec) were used to measure participants’ motion. Foot center of pressure (COP, cm) relative to the lateral midfoot axis was measured from the force plate. Maximum ankle eversion over stance (°) and external tibial rotation at heel strike (°) were calculated from 3 walking trials. Frontal-plane mechanical axis was determined from full-length standing-alignment radiographs of the lower limbs6.
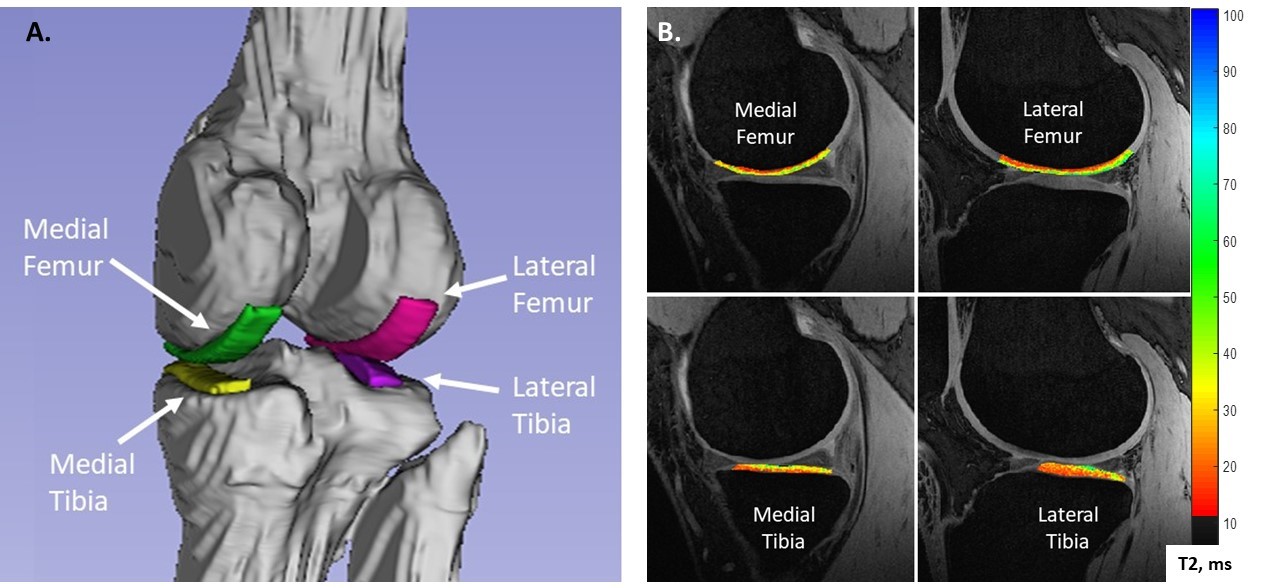
T2 maps were generated from a quantitative double-echo in steady state (qDESS)7 sequence (TR/TEs 21ms/6, 36 ms; 0.417x0.417mm resolution; 1.5mm slice-thickness). Maps were manually segmented to include 10.5mm-wide strips of cartilage (largely consistent with known areas of contact during common daily activities8) on each of 4 knee surfaces: medial and lateral femurs (MFC, LFC) and tibial plateaus (MTP, LTP), Figure 1.
Normality was assessed by Shapiro-Wilk tests. T-tests compared kinematics, COP and T2s of the study cohort to healthy controls with p<0.05 accepted as significant. Dependencies among kinematics, COP and mechanical axis and correlations between those factors and cartilage T2 were assessed with Pearson correlations (Spearman’s rho for non-normal data). Linear regression assessed effects of age, sex, BMI and walking speed on these correlations. Adjusted p<0.013 was accepted as significant where 4 potentially independent factors (COP, ankle eversion, tibial rotation, mechanical axis) were tested for association with cartilage T2.
RESULTS
Appropriateness of study cohort: As expected, cartilage T2 did not differ from those of healthy controls, Table 1. In the study cohort, more medial COP correlated to greater ankle eversion (R=0.58, p=0.003). No other correlations were detected between foot COP, ankle eversion, tibial rotation, or mechanical axis.Correlations of lower limb alignment to knee cartilage T2: More medial foot COP correlated to lower MFC cartilage T2 (R=-0.71, p<0.0005), Figure 2a, and showed a trend for association with lower LFC T2 (R=-0.48, p=0.019). After adjusting for sex, greater ankle eversion correlated with lower MFC T2 (R= -0.54, p=0.006), Figure 2b. More internal tibial rotation correlated to higher LTP T2 (R=-0.52, p=0.009), Figure 2c. Mechanical axis did not correlate to T2 in any TF region. Linear regression found no other effects with age, sex, BMI, or walking speed.
DISCUSSION
In knees without clinical evidence of osteoarthritis, ipsilateral foot and ankle posture are related to tibiofemoral cartilage composition. Biomechanical models linking flat-footedness, ankle eversion and internal tibial rotation3,9 suggest these factors couple to generate rotational stress across the TF joint. Our finding of elevated lateral tibial T2 with increased internal tibial rotation is consistent with this paradigm. Additionally, more medial COP and greater ankle eversion related to lower medial femoral cartilage T2. This observation is in-line with a report relating greater flat-footedness to lower medial TF contact forces in healthy knees10, and may represent evidence of an adaptation strategy similar to that adopted by individuals with knee OA11. Among the many biomechanical factors contributing to knee OA, flat-footedness and ankle eversion are relatively accessible targets for potential therapeutic or preventative interventions. Further study is needed to elucidate the biomechanical linkages between foot and ankle posture and knee cartilage health in both healthy individuals and patients with knee OA.CONCLUSION
Correlation of foot and ankle posture to cartilage composition at the knee suggest that gait or shoe interventions to appropriately alter weight distribution at the foot and ankle could be utilized to benefit to knee cartilage health.Acknowledgements
DOD W81XWH-18-1-0590 (PI-CR Chu)References
- Levinger P, Menz HB, Fotoohabadi MR, Feller JA, Bartlett JR, Bergman NR. Foot posture in people with medial compartment knee osteoarthritis. Journal of foot and ankle research 2010; 3: 29.
- Zhang M, Nie MD, Qi XZ, et al. A Strong Correlation Between the Severity of Flatfoot and Symptoms of Knee Osteoarthritis in 95 Patients. Frontiers in surgery 2022; 9: 936720.
- Lundberg A, Svensson OK, Bylund C, Goldie I, Selvik G. Kinematics of the ankle/foot complex--Part 2: Pronation and supination. Foot Ankle 1989; 9(5): 248-53.
- Gross KD, Felson DT, Niu J, et al. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res (Hoboken) 2011; 63(7): 937-44.
- MacKay JW, Low SBL, Smith TO, Toms AP, McCaskie AW, Gilbert FJ. Systematic review and meta-analysis of the reliability and discriminative validity of cartilage compositional MRI in knee osteoarthritis. Osteoarthritis Cartilage 2018; 26(9): 1140-52.
- Brown G, Amendola A. Radiographic Evaluation and Preoperative Planning for High Tibial Osteotomies. Oper Tech Sports Med 2012; 20: 93-102.
- Chaudhari AS, Black MS, Eijgenraam S, et al. Five-minute knee MRI for simultaneous morphometry and T(2) relaxometry of cartilage and meniscus and for semiquantitative radiological assessment using double-echo in steady-state at 3T. J Magn Reson Imaging 2018; 47(5): 1328-41.
- Thomeer LT, Guan S, Gray HA, Pandy MG. Articular contact motion at the knee during daily activities. J Orthop Res 2022; 40(8): 1756-69.
- Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical model. J Orthop Sports Phys Ther 1987; 9(4): 160-5.
- Kubo T, Uritani D, Ogaya S, et al. Association between foot posture and tibiofemoral contact forces during barefoot walking in patients with knee osteoarthritis. BMC Musculoskelet Disord 2022; 23(1): 660.
- Levinger P, Menz HB, Morrow AD, Bartlett JR, Feller JA, Bergman NR. Relationship between foot function and medial knee joint loading in people with medial compartment knee osteoarthritis. Journal of foot and ankle research 2013; 6(1): 33.
Figures